19 August 2022: Original Paper
Risk Factors for Erythrocytosis in Renal Transplantation: Is Ganciclovir Therapy One of Them?
Fatma Özge Kayhan Koçak1ABCDEF*, Musa Bali2ADEFDOI: 10.12659/AOT.936814
Ann Transplant 2022; 27:e936814






Abstract
BACKGROUND: The purpose of this study was to identify the prevalence and risk factors of post-transplant erythrocytosis (PTE) and its relationship with cytomegalovirus (CMV).
MATERIAL AND METHODS: The study consisted of patients who received a kidney allograft and followed-up in our nephrology transplantation clinic from 2000 to 2014. Patient age, sex, length of dialysis, etiology of end-stage kidney disease, date of transplantation, medications, types of donors, the development of PTE were recorded.
RESULTS: Among 185 adult kidney recipients, 43 (23.2%) had PTE. The average time between transplantation and diagnosis was 36 months. PTE was more common in male patients (P<0.05) and patients with living donors and those who had been treated with ganciclovir after transplantation (P<0.05). There were 79 patients treated for CMV – 54 in the non-PTE group and 24 in the PTE group. There was no significant difference in patient age, etiology of end-stage kidney disease, and immunosuppressive therapy when comparing the PTE group and non-PTE group. Univariate analysis showed ganciclovir therapy was significantly associated with PTE. However, this was not seen in the multivariate analyses.
CONCLUSIONS: Treatment with ganciclovir can precipitate development of PTE. Prospective studies are needed to assess the association of between PTE and CMV infection, valganciclovir, and ganciclovir.
Keywords: Cytomegalovirus, Ganciclovir, Kidney Transplantation, Polycythemia, Risk Factors, Adult, Antiviral Agents, Cytomegalovirus Infections, Humans, Kidney Failure, Chronic, Male
Background
Post-transplant erythrocytosis (PTE) is defined as a hemoglobin level above 17 g/dl or a hematocrit level above 51% after a successful kidney transplantation, independent of sex and duration [1]. It is a common, well-established complication seen in 5–15% of renal transplant patients and has been reported globally for more than 30 years.
The etiology of PTE is unclear and is generally thought to have a multifactorial etiology [2]. Well-known risk factors include younger recipient age, young donor age, polycystic kidney disease, male sex, retention of a native kidney with adequate erythropoiesis before transplant, renal artery stenosis, and a well-functioning graft [2,3]. The relationships between PTE and certain immunosuppressive agents used in renal transplant are unclear [4–6].
Cytomegalovirus (CMV) is one of the most common viral infections in solid-organ transplant patients [7,8]. CMV infection is usually seen within the first 1–6 months after renal transplantation, and clinical manifestations of CMV range from asymptomatic CMV seroconversion to mononucleosis syndrome. The diagnosis of CMV infection is made by demonstration of CMV replication; serological changes in the recipient (seroconversion: CMV IgM positivity, 4-fold or greater increase in pre-existing CMV IgG titer), detection of CMV antigen in infected cells (pp65 antigen), CMV replication in cultures (throat, sputum, urine), detection of CMV-DNA by PCR [9]. CMV prophylaxis is recommended for kidney transplant recipients except when both recipients and donors have negative CMV serology. The present study evaluated risk factors for erythrocytosis in patients with renal transplantation and to assess the relationship with CMV prophylaxis and PTE.
Material and Methods
DATA ANALYSIS AND STATISTICAL METHODS:
SPSS version 25.0 was used to evaluate data. Normality was assessed by Kolmogorov-Smirnov test. Normally distributed quantitative variables are expressed as mean and standard deviation, while those without normal distribution are expressed as median, minimum, and maximum values. Qualitative variables are expressed as frequency and percentage. The chi-square (χ2) test and Fisher’s exact test were used in the analysis of qualitative variables. Patients were divided into 2 subgroups: patients with PTE (PTE group) and patients with PTE (non-PTE group). The 2 groups were compared using the
Results
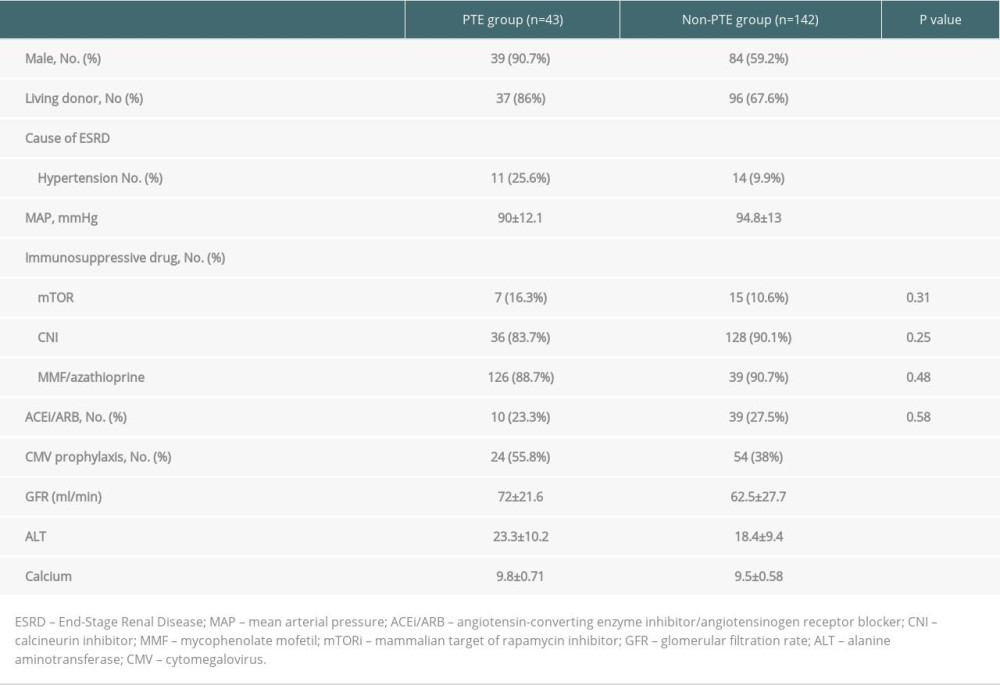
The study included 185 kidney transplant recipients followed up in the nephrology transplantation outpatient clinic at the Faculty of Medicine in University between 2000 and 2014. The age distribution was 38±14 years (18–77), and there was no statistically significant difference in age between the PTE group and the non-PTE group. Of the 185 patients, 62 (33.5%) were female and 123 (66.5%) were male. Of the 185 adult kidney recipients, 43 (23.2%) developed PTE. The mean time from transplantation to diagnosis of PTE was 36 months. Thirty-nine of the patients with PTE were male (90.7%), and PTE was 3 times higher among males (
There was no significant difference in weight, current smoking status, pre-transplant red cell transfusion history, kidney rejection, duration of dialysis prior to transplantation, or nephrectomy between the PTE group and non-PTE group (
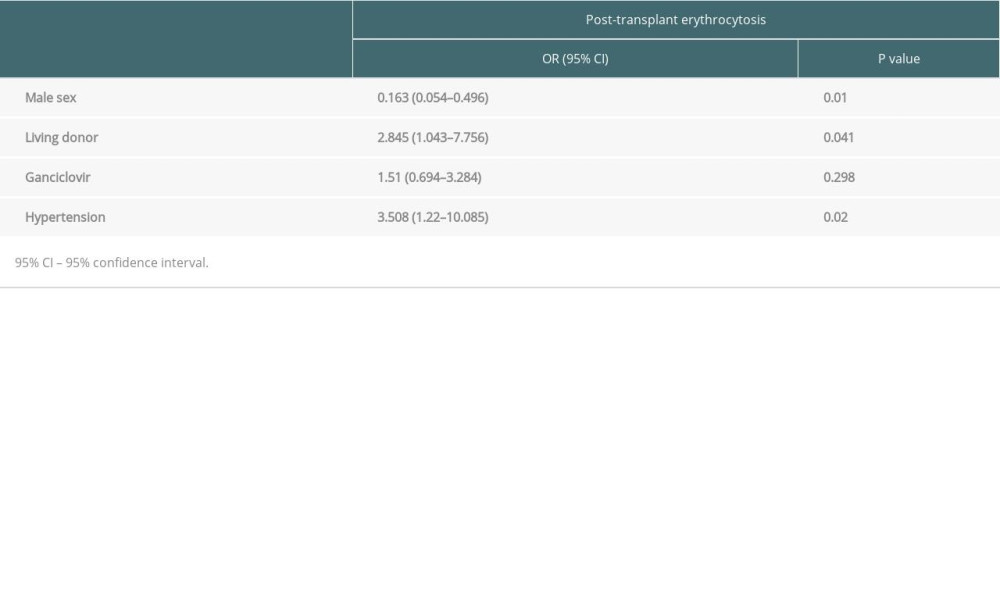
Of the 185 adult kidney recipients, 79 received CMV treatment – 54 in the non-PTE group and 24 in the PTE group. Univariate analysis showed ganciclovir treatment was significantly associated with PTE, but this was not shown by multivariate analyses. Multivariate analysis showed that risk factors for PTE were male sex, living donor, and presence of hypertension (Table 2).
Discussion
In this study, the frequency and risk factors of PTE were investigated in 185 kidney transplant patients. Male sex, living donor, hypertension, CMV prophylaxis, high GFR, high ALT level, and high calcium level were significantly associated with increased risk of PTE in the univariate analysis, while multivariate logistic regression analysis revealed male sex, living donor, and hypertension to significantly predict the increased risk of erythrocytosis among kidney transplant recipients.
The characteristics of patients in this study were found to be similar to the general demographic characteristics of other studies [10–12]. In our study, PTE was common particularly in men (90.7% male) similar to the literature [2,6,10–12]. It has been shown that male patients undergoing hemodialysis need less exogenous replacement of erythropoietin than female patients undergoing hemodialysis. Androgens indirectly stimulate erythrocytosis by stimulating endogenous erythropoietin, which is thought to cause PTE to occur more frequently in men. The risk of cardiovascular events due to hypertension is higher in patients who receive kidney transplantation. Therefore, treatment and follow-up of HT have an important role in survival. Ghahramani et al observed that PTE was not seen in normotensive patients, and they reported that PTE was observed in 35% of hypertensive patients [13]. A study of living-donor kidney transplant recipients found that pre-transplant hypertension was significantly more frequent in the PTE group than in the non-PTE group [14]. Contrary to our study, deceased donor KT recipient status was associated with PTE in a recent meta-analysis [2].
Ganciclovir treatment was given for 3 months after transplantation in patients who were CMV PCR-positive before kidney transplantation. In our study, ganciclovir treatment was given to 24 of 43 patients with PTE, and it was a statistically significant risk factor for PTE. It is known that ganciclovir usually causes a lower neutrophil count [15]. A study that evaluated kidney transplant patients with deep venous thrombosis found no significant relationship between CMV infection and thrombosis [16]. CMV infection usually causes anemia via hemophagocytic syndrome [17]. However, there is a previous review arguing that CMV infection increases hypercoagulopathy with endothelial cell damage [18]. It was reported that tissue factor expression is increased in endothelial cells infected with CMV [19,20]. CMV has been suggested to have important role in hemostasis and thrombosis formation [21,22]. To the best of our knowledge, the present study is the first to find a relationship between PTE and ganciclovir.
There is limited research on the impact of CMV on PTE, which adds to the value of our study. Although the present study has several strengths, there are some limitations that should not be overlooked. The first of these is that we could not prove a causal relationship by performing a cross-sectional study. Another important limitation is the small numbers of patients. Additionally, we did not include data on use of valganciclovir.
Conclusions
PTE causes thromboembolic events and negatively affects the prognosis of kidney transplant patients when not treated. Therefore, risk factors for PTE should be carefully observed during follow-up and should not prevent proper treatment. In conclusion, ganciclovir treatment can precipitate PTE development. Prospective studies are needed to assess the effects of CMV infection, valganciclovir, and ganciclovir on PTE.
References
1. Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group, Special Issue: KDIGO clinical practice guideline for the care of kidney transplant recipients: Am J Transplant, 2009; 9; S1-155
2. Mekraksakit P, Boonpheng B, Leelaviwat N, Risk factors and outcomes of post transplant erythrocytosis among adult kidney transplant recipients: A systematic review and meta analysis: Transpl Int, 2021; 34(11); 2071-86
3. Alzoubi B, Kharel A, Machhi R, Post-transplant erythrocytosis after kidney transplantation: A review: World J Transplant, 2021; 11(6); 220-30
4. Koziak K, Rell K, Lao M, Does erythropoietin production after renal transplantation depend on the type of immunosuppression?: Nephron, 1995; 71(2); 236-37
5. Augustine JJ, Knauss TC, Schulak JA, Comparative effects of sirolimus and mycophenolate mofetil on erythropoiesis in kidney transplant patients: Am J Transplant, 2004; 4(12); 2001-6
6. Kiberd BA, Post-transplant erythrocytosis: A disappearing phenomenon?: Clin Transplant, 2009; 23(6); 800-6
7. Razonable RR, Humar A, Cytomegalovirus in solid organ transplant recipients – Guidelines of the American Society of Transplantation Infectious Diseases Community of Practice: Clin Transplant, 2019; 33(9); e13512
8. Li Y, Yan H, Xue WJ, Treatment of Cytomegalovirus infection after renal transplantation: Experience from a Single Center in China: Ann Transplant, 2013; 18; 125-35
9. Ljungman P, Boeckh M, Hirsch HH, Definitions of cytomegalovirus infection and disease in transplant patients for use in clinical trials: Clin Infect Dis, 2017; 64(1); 87-91
10. Alzoubi B, Kharel A, Osman F, Incidence, risk factors, and outcomes of post transplant erythrocytosis after kidney transplantation: Clin Transplant, 2021; 35(2); e14166
11. Sreeadhara C, Narayanaswamy R, Lingaraju U, Early initiation of angiotensin-converting enzyme inhibitors in postrenal transplant period: A study from a state-run tertiary care center: Saudi J Kidney Dis Transplant, 2018; 29(3); 637-42
12. Yeter HH, Fettahoglu F, Yesiloglu E, Risk factors for posttransplant erythrocytosis: Parathyroid hormone paradox?: Exp Clin Transplant, 2020 [Online ahead of print]
13. Ghahramani NL, Malek-Hosseini SA, Rais-Jalali GA, Factors relating to posttransplant erythrocytosis in renal allograft recipients: Transplant Proc, 1998; 30(3); 828-29
14. Abouelenein RK, Refaie AF, Alhendy YA, Posttransplant erythrocytosis among egyptian living-donor kidney transplant recipients: Exp Clin Transplant, 2018 [Online ahead of print]
15. Billat PA, Woillard JB, Essig M, Plasma and intracellular exposure to ganciclovir in adult renal transplant recipients: Is there an association with haematological toxicity?: J Antimicrob Chemother, 2016; 71(2); 484-89
16. Todeschini P, la Manna G, Dalmastri V, Incidence of late deep venous thrombosis among renal transplant patients: Transplant Proc, 2013; 45(7); 2666-68
17. Marinella MA, Hematologic abnormalities following renal transplantation: Int Urol Nephrol, 2010; 42(1); 151-64
18. Kazory A, Ducloux D, Acquired hypercoagulable state in renal transplant recipients: Thromb Haemost, 2004; 91(04); 646-54
19. van Gorp ECM, Suharti C, ten Cate H, Review: Infectious diseases and coagulation disorders: J Infect Dis, 1999; 180(1); 176-86
20. Irish A, Hypercoagulability in renal transplant recipients: Am J Cardiovasc Drugs, 2004; 4(3); 139-49
21. Squizzato A, Gerdes V, Büller H, Effects of human cytomegalovirus infection on the coagulation system: Thromb Haemost, 2005; 93(03); 403-10
22. Wang L, Hsu Y, Sharma N, Thrombosis associated with cytomegalovirus (CMV) in a kidney transplant recipient: Cureus, 2021; 13(9); e17745
In Press
15 Mar 2024 : Review article
Approaches and Challenges in the Current Management of Cytomegalovirus in Transplant Recipients: Highlighti...Ann Transplant In Press; DOI: 10.12659/AOT.941185
18 Mar 2024 : Original article
Does Antibiotic Use Increase the Risk of Post-Transplantation Diabetes Mellitus? A Retrospective Study of R...Ann Transplant In Press; DOI: 10.12659/AOT.943282
20 Mar 2024 : Original article
Transplant Nephrectomy: A Comparative Study of Timing and Techniques in a Single InstitutionAnn Transplant In Press; DOI: 10.12659/AOT.942252
28 Mar 2024 : Original article
Association Between FEV₁ Decline Rate and Mortality in Long-Term Follow-Up of a 21-Patient Pilot Clinical T...Ann Transplant In Press; DOI: 10.12659/AOT.942823
Most Viewed Current Articles
05 Apr 2022 : Original article
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
12 Jan 2022 : Original article
Risk Factors for Developing BK Virus-Associated Nephropathy: A Single-Center Retrospective Cohort Study of ...DOI :10.12659/AOT.934738
Ann Transplant 2022; 27:e934738
22 Nov 2022 : Original article
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988
15 Mar 2022 : Case report
Combined Liver, Pancreas-Duodenum, and Kidney Transplantation for Patients with Hepatitis B Cirrhosis, Urem...DOI :10.12659/AOT.935860
Ann Transplant 2022; 27:e935860