05 January 2022 : Original article
Reconstruction of Separated Intrahepatic Ducts Using the Cystic and Common Hepatic Ducts in Right-Lobe Living-Donor Liver Transplantation: Experiences of Surgical Techniques, Biliary Complications, and Outcomes in a Single Institution
Po-Jung Hsu1ABCDEF, Hao-Chien Hung12ABCDEF, Ching-Sung Lee3A, Kuang-Tse Pan4A, Jin-Chiao Lee32A, Yu-Chao Wang32A, Chih-Hsien Cheng32A, Tsung-Han Wu32A, Chen-Fang Lee32A, Hong-Shiue Chou32A, Kun-Ming Chan32A, Wei-Chen Lee32A, Ting-Jung Wu12ACDEF*DOI: 10.12659/AOT.934459
Ann Transplant 2022; 27:e934459






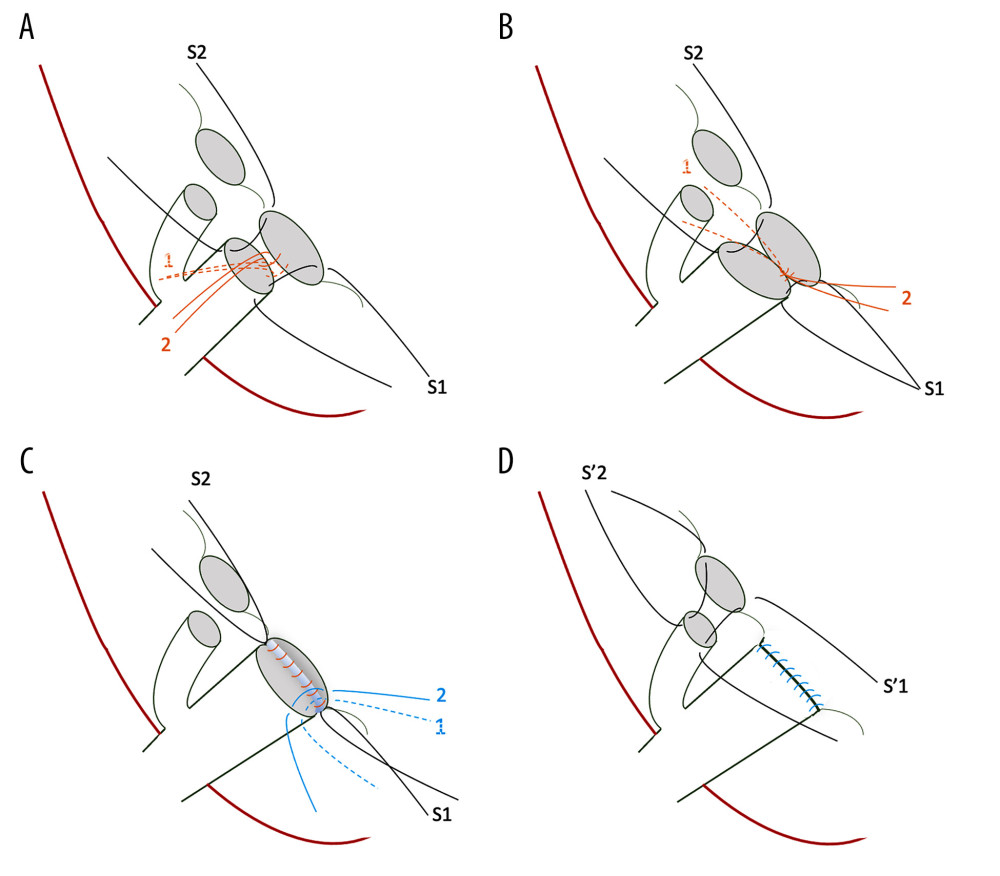
Figure 1 Steps of the dual biliary duct reconstruction, demonstrated as the anastomosis of the right posterior intrahepatic duct (IHD) to the common hepatic duct (CHD)/anastomosis of the right anterior IHD to the cystic duct: (A) S1 and S2 represent 6-0 interrupted sutures through ductal edges on both sides, serving as long stay sutures. Reconstruction is initiated at the posterior wall of the bile duct at the medial side, as shown by the orange lines. (B) The second stitch (orange line 2) is moved in the opposite direction to create a working space and then the knot is secured in the first stitch (orange line 1). Proceed laterally and posteriorly stitch by stitch until the posterior part is completed. Care should be taken to ensure to tie the knots outside the bile duct lumen. (C) After the posterior wall is completed, start the anterior wall from the superior or medial side, and finish by tying knots, which are sutured into the edges of ducts but remain untied until the end for a clearer view. (D) Start the right anterior IHD-cystic duct anastomosis using stay long sutures (S1 and S2) and follow the aforementioned steps.