12 March 2021: Review Paper
Effect of Calcineurin Inhibitors and Mammalian Target of Rapamycin Inhibitors on the Course of COVID-19 in Kidney Transplant Recipients
Nuri Baris Hasbal1AEF*, Didem Turgut2AEF, Ebru Gok Oguz3AEF, Sena Ulu4AEF, Ozkan Gungor5AEFDOI: 10.12659/AOT.929279
Ann Transplant 2021; 26:e929279






Abstract
ABSTRACT: Coronavirus disease 19 (COVID-19) has been an ongoing pandemic since December 2019. Unfortunately, kidney transplant recipients are a high-risk group during the disease course, and scientific data are still limited in this patient group. Beyond the dosage of immunosuppressive drugs, pharmacological immunosuppression may also alter the infection response in the COVID-19 course. The effects of immunosuppressive agents on the development and process of infection should not be decided only by determining how potent they are and how much they suppress the immune system; it is also thought that the direct effect of the virus, increased oxidative stress, and cytokine storm play a role in the pathogenesis of COVID-19 disease. There are data about immunosuppressive drugs like calcineurin inhibitors (CNI) or mammalian target of rapamycin inhibitors (mTORi) therapy related to their beneficial effects during any infection course. Limited data suggest that the use of CNI or mTORi may have beneficial effects on the process. In this hypothetical review, the probable impacts of CNI and mTORi on the pathogenesis of the COVID-19 were investigated.
Keywords: COVID-19, Kidney Transplantation, TOR Serine-Threonine Kinases, adaptive immunity, COVID-19, calcineurin inhibitors, cytokine release syndrome, Graft Rejection, Immunity, Innate, Immunocompromised Host, Immunosuppressive Agents, Postoperative Complications, Protein Kinase Inhibitors
Background
The world has been in a great struggle with COVID-19 for about 1 year. Immunosuppression is a significant risk factor related to the disease, and kidney transplant recipients are one of the high-risk patient groups. There are case reports about COVID-19 infection seen in kidney transplant patients in the literature. These reports have been viewed in a compilation by Imam et al In that review, the data of 129 cases from 24 articles were analyzed; 92% of the patients were receiving tacrolimus-based treatment. Acute kidney damage developed in 31% of the patients. Among all patients, 18.8% had died, in contrast to the reported general population COVID-19 mortality of 3.4% [1].
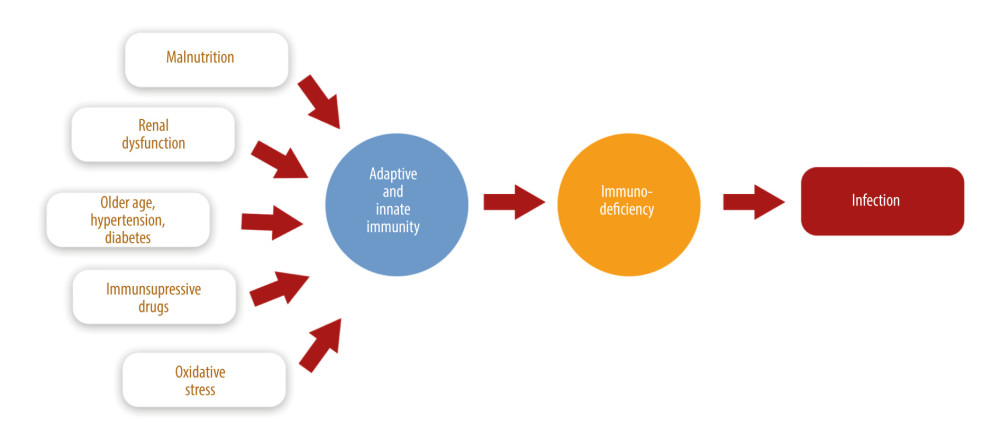
In these patients, different factors might predispose to COVID-19. Factors affecting the disease course in kidney recipients are summarized in Figure 1.
Immunosuppressive drug modification would be helpful at the beginning of the disease course, but the optimal drug modification remains uncertain at present. Poulsen et al stated that continuing the therapy, unless otherwise proven, might have a positive result during COVID-19. This recommendation is not due to a clinical study but is based on the knowledge that calcineurin inhibitors (CNI) may inhibit T cell activation by blocking transcription of cytokines and also cyclosporin analouges such as alisporivir inhibits replication of severe adult respiratory syndrome coronavirus-2 (SARS-CoV-2) in vitro [2]. In a systematic review including 50 studies and 337 patients, Moosavi et al analyzed the drug modification strategies. Generally, anti-metabolite and CNI were reduced or discontinued, and steroid doses were increased, in patients with solid-organ transplantation and COVID-19 [3], but patient outcomes could not be assessed if they were associated with decreased immunosuppression or increased steroid dose. There are different strategies determined according to the patient’s clinical condition and the approach of the transplantation centers. The most common arrangements are to decrease or withhold antiproliferative therapy, decrease CNI to a minimum dose and stop it if there is any infection progression, and to continue steroids at the usual dose or increase it if other immunosuppressive drugs were stopped [4]. In this review, we discuss 2 important drug groups – CNI and mammalian target of rapamycin inhibitors (mTORi) – in kidney transplant patients during the COVID-19 pandemic.
Pharmacological Action of CNIs and mTORi Related to COVID-19
Beyond the dosage of immunosuppressive drugs, pharmacological methods of immunosuppression may also alter the infection response in the course of COVID-19 disease. The effects of immunosuppressive agents on the development and process of infection should not be decided only by determining at how potent they are and how much they suppress the immune system because these drugs also have features other than immunosuppression, such as effects on oxidant stress, complement activation, and drug interactions. CNI and mTORi therapy are 2 groups of drugs that have been compared for many years in many studies in terms of rejection rates, costs, and adverse effects [5–7]. It could be important to know whether CNI and mTORi have different effects on the development and course of COVID-19 infection, but there are no comparative data on the possible effects on COVID-19. A recently published article argued that the use of calcineurin inhibitors would be beneficial in the pandemic course [8]. Studies have shown that the cytopathic effect of the virus, oxidant system activation, and cytokine storm are cornerstones in the pathogenesis of COVID-19 [2,3]. In the early stages of the COVID-19 pandemic, it was speculated that immunosuppressive therapy would facilitate the cytopathic effects of the virus. With a better understanding of the pathogenesis, we might prognosticate that immunosuppressive therapy would lessen the cytokine storm effect. Here, we aimed to consider, in the light of current literature, whether CNI and mTORi have different effects on antiviral activity, oxidant-antioxidant balance, and cytokine storm, which are important mechanisms known in the pathogenesis of COVID-19.
Effects of CNI and mTORi on Viral Infections
CNI and mTORi are the most critical parts of kidney transplant maintenance therapy, but they make kidney recipients more susceptible to infections. In the literature evaluating the possible relationship of CNI and mTORi with viral infections, tacrolimus has been associated with more BK viremia than cyclosporine [9]. mTORi, which are also used in post-transplant lymphoproliferative diseases related to Epstein-Barr Virus viremia, are not mainly related to increased viral infections [10]. In a meta-analysis evaluating the combination of CNI and mycophenolate mofetil (MMF) versus the combination of CNI and mTORi, fewer cytomegalovirus (CMV) infections were detected in patients treated with mTORi [11]. In another multicenter study with kidney transplant recipients, patients taking everolimus had fewer CMV and BK virus infections than patients treated with CNI and MMF [12]. In immunologically low-risk patients, the use of de novo mTORi with low-dose CNI has been reported to decrease viral infection rates [13,14].
Although studies have focused on the increased infection risk of CNI and mTORi due to immunosuppression in renal transplantation, many studies have questioned the antiviral effectiveness according to their mechanism of action [8,15]. Cyclosporin A (CsA) and tacrolimus inhibit gene transcription of interleukin (IL) 2 and produce some cytokines in T cells. Thus, they suppress T cell and T cell-dependent B cell activation [16]. Most viruses use active immunophilin pathways during their life cycle. Both the cyclophilin family and tacrolimus-binding proteins interact with viruses. This interaction allows CNI to control the inflammatory response in viral infections. For example, cyclosporine inhibits the replication of the hepatitis C virus in vitro [17]. CNI (in the therapeutic range) might be useful to control the destructive effects of cytokines in the hyperinflammatory phase of viral infection with reduction of virus-related cytokine storm. This idea was supported by a study evaluating CsA in the treatment of hemophagocytic lymphohistiocytosis, which is related to excessive proinflammatory cytokine release. Activated T cell-mediated IL-2 gene transcription can be inhibited with cyclosporin, and both cell proliferation and cytokine production decreased [18].
The Mechanism of mTORi-Induced Suppression of Cytokines
The mammalian target of rapamycin (mTOR) pathway is a protein kinase inhibited by rapamycin and plays a role in regulating cell proliferation. Protein kinases and inhibitors are divided into 2 groups according to their substrates: protein tyrosine kinases and protein serine/threonine kinases. mTOR, a serine/threonine kinase, has different biological activities and consists of 2 different multiple protein complexes. Rapamycin acts on both mTOR complex 1 (mTORC1) and mTOR complex 2 (mTORC2). mTORC1 plays a role in mitogen (eg, insulin-like growth factor) and cytokine synthesis. The function of mTORC2 is unclear. By inhibiting IL2-mediated signal transmission, mTORi causes cell cycle arrest in the G1-S phase, resulting in disruption of cellular functions such as cell division, T cell activation, and growth factor production. Thus, mTORi inhibits B and T cell proliferation and blocks the proliferative effects of IL 1, 2, 3, 4, 6, insulin-like growth factor, platelet-derived growth factor, and colony-stimulating factors. It is reasonable to conclude that the antiviral activity of mTORi may be associated with mTORC1, which is involved in cytokine synthesis. CMV infections were less prevalent with the use of mTORi and low-dose CNI, and the frequency of polyomavirus infection decreased with mTORi de novo use [19]. The antiviral efficacy of mTORi has been supported in animal studies, too. Rapamycin had protective impacts against influenza type H3N2 in animal studies [20], and the effects of influenza on alveolar type 2 cells were abolished by rapamycin [21]. Influenza studies in humans have produced conflicting results. Although severe H1N1 influenza-induced pneumonia improved with rapamycin and steroids, it was concluded that viral replication is prolonged, resulting in increased mortality [21].
The evidence shows that CNI and mTORi inhibit many pathways used by viruses and can control cytokine synthesis. They might have potential antiviral and immunomodulatory effects.
Antibody-Dependent Enhancement and Cytokine Storm
Based on previous experience with coronavirus (CoV) outbreaks such as Middle-East respiratory syndrome and severe acute respiratory syndrome (SARS) and SARS animal model studies, lung inflammation increases to reach the peak no later than 14 days after viral clearance. This period is the effector phase, which we define as the lymphocyte activation and antigen elimination of the immune system. Tissue damage occurs with uncontrolled and inappropriate antiviral response rather than viral proliferation [22]. Antibody-dependent enhancement (ADE) and cytokine storm need to be further studied to better understand the pathogenesis in this context.
High-affinity antibodies can recognize specific viral epitopes and cause neutralization. Neutralizing antibodies can be identified in vitro with their ability to inhibit virus entry, fusion, or exit. These neutralizing antibodies can interact with the complement system, phagocytes, and natural killer (NK) cells [22]. However, these pathogen-specific protective antibodies can promote pathology in rare cases, resulting in a phenomenon known as ADE [23]. The ADE phenomenon occurs with the participation of Fc receptors (FcR) expressed on different immune cells, including monocytes, macrophages, and B cells. Thus, preexisting specific antibodies can facilitate viral entry into cells expressing FcR. This process is independent of angiotensin-converting enzyme-2 (ACE2) expression, endosomal pH, or proteases, and results in both viral replication in immune cells and immune complex-mediated inflammatory response. Studies have shown that new CoVs increase tumor necrosis factor (TNF) and IL-6 production in macrophages through ADE [24]. In SARS-CoV-infected mice, the ADE phenomenon has been associated with decreased levels of IL-10 and transforming growth factor-β (TGF-β). Increased proinflammatory circulating chemokine ligand (CCL) 2 and CCL3 chemokine levels, which have anti-inflammatory and immunosuppressive properties, are also prominent [25]. Thus, although not fully proven in SARS-CoV-2, the ADE phenomenon can lead to severe disease.
Cytokine storm, macrophage activation syndrome, and hemophagocytic lymphohistiocytosis are not specific to COVID-19. They are leading causes of acute respiratory distress syndrome (ARDS) and can also occur in sepsis, other viral infections, and as the adverse effects of some drugs [26]. Inflammatory damage can be weakened by anti-cytokine or anti-cytokine receptor treatments, as well as small-molecule complement inhibitors at an early stage of infection. Clinical studies on tocilizumab, anakinra, and Janus kinase (JAK) inhibitors are ongoing. The above evidence suggests that maintenance immunosuppression agents can affect COVID-19, since kidney transplant patients who use continuous immunosuppressive drugs overcome the disease, with a possible milder clinical picture.
Surmising Risks and Benefits of CNI and mTORi for Kidney Transplant Recipients
In studies discussing the effects of COVID-19 in kidney transplant patients, immunosuppressive agents were discontinued, or the dose was reduced [27,28], but we do not know if there is a difference in the course of the disease among those using mTORi or CNI. Willicombe et al stated that CNI could be continued to be used in kidney transplant patients for 2 different reasons. The first is the ability of these agents to reduce viral replication, as demonstrated by experimental studies on SARS-CoV. The second is the assumption that they may have the ability to reduce a similar cytokine storm during the course of COVID-19, based on the effectiveness of CNI in hemophagocytic lymphohistiocytosis and capillary leak syndrome [8].
Bourboulis et al evaluated immune responses of COVID-19 patients (n=54) with macrophage activation syndrome and found that CD4+ T lymphocytes, CD19+ B lymphocytes, and NK cells, and their human leucocyte antigen (HLA)-DR expression were significantly decreased [29]. In another study, everolimus reduced the amount of interferon gamma (IFN-gamma)-induced HLA-DR in endothelial cells [30]. In contrast, tacrolimus affects basal or IFN-gamma-induced HLA-DR in monocytic cell lines [31]. It has been reported that mTORi reduces cytotoxic T cells and effector memory T cells in Belatacept-resistant kidney transplant rejections [32]. This benefit may help to prevent the tissue damage caused by viral replication in COVID-19 disease or protect against recurrent infections by under-controlling the immune memory.
The effects of sirolimus and tacrolimus on B cells may differ from each other. Sirolimus has been shown to reduce CD19+ CD27+ memory B cells and their conversion to plasma cells. Sirolimus reduces the total number of B cells more than tacrolimus but makes them stronger by increasing HLA-DR expression [33,34]. In this way, sirolimus may control neutralizing antibody production in COVID-19 patients. In kidney transplant recipients using mTORi (everolimus or sirolimus), there were also higher proportions of regulatory T cells (Treg) [35]. Tregs suppress effector T cell induction and proliferation, which prevents cytokine storm. In contrast, in a cell culture study by Eleftheriadis et al, tacrolimus was more effective in suppressing cellular immunity compared to everolimus and both have similar impacts on humoral immunity [36]. Tacrolimus might be the other option to prevent the production of T cell-induced cytokines in COVID-19 cases.
Effects of CNI and mTORi on Transplantation-Related Oxidative Stress
Oxidative stress results from a disturbance between oxidant and antioxidant balance, producing a large number of reactive oxygen species (ROS, an atom or group of atoms that have 1 or more unpaired electrons) in the cells. ROS are normally generated in a constant amount and are essential to life, but increased numbers of ROS damage proteins, lipids, and deoxyribonucleic acid (DNA) [37]. Antioxidant capacity is related to enzymes catalyzing oxygen radicals (eg, oxidases, glutathione peroxidase, superoxide dismutase (SOD)) and antioxidants (eg, tocopherols, glutathione, ascorbic acid) in the organisms [37]. Triggers of oxidative stress are mainly xenobiotics, microorganisms, inflammation, and radiation. In enhanced inflammatory conditions like chronic kidney disease (CKD) and kidney transplantation, oxidative stress promotes inflammation by activating the proinflammatory transcription factors, and chronic inflammation reciprocally amplifies the oxidative stress [38]. In the early phase of kidney transplantation, end-stage kidney disease (ESKD)-related radicals such as hydrogen peroxide (H2O2) or hypochlorous acid (HOCl), and free radicals such as superoxide (O2−), hydroxyl radical, and nitric oxide, ischemia-reperfusion injury, and immunosuppressive drugs are responsible for oxidative stress. Endothelial injury, atherosclerosis, and increased creatinine participate in oxidative stress in the late phases [39]. Immunosuppressant drugs like CNI and mTORi are candidate drugs that change the balance in the direction of antioxidation.
CNI, especially tacrolimus, has some nonimmunological effects unrelated to transplantation, such as improvement in ischemia-reperfusion injury (IRI). Control of ischemia thought to be related to nitric oxide synthase (NOS) inhibition, resulting in decreased oxidative stress [40]. In an experimental model of IRI, tacrolimus decreased ROS, lipid peroxidation products, and TNF-a expression of cells [41]. CsA-related antioxidant activity is thought to be weaker than that of tacrolimus. In kidney and heart transplantation, it is reported that CsA was related to increased production of ROS, but in another study, CsA and tacrolimus were compared to advanced oxidation protein products in the sixth month of transplantation, and no difference was found [42]. Cvetkovic et al analyzed nitrosative stress parameters (asymmetric and symmetric dimethylarginine), and antioxidative parameters (total SH groups and catalase activity) after 1 year of transplantation. There was no significant difference in parameters concerning the immunosuppressive protocol [43].
The effects of mTORi (including rapamycin and everolimus) on oxidative stress are controversial. Some groups demonstrated that mTOR signaling is crucial to prevent ischemia preconditioning and IRI, but other evidence suggests that mTORi inhibits IRI [44]. In an experimental model of Friedreich’s ataxia, the authors found that rapamycin protects cells against oxidative stress, with increased transcription of antioxidant genes. Lower doses of rapamycin may be beneficially combined with other drugs such as antioxidants and iron chelators [45]. Rapamycin, together with metformin, were also found to reverse age-dependent biomarkers of oxidative stress, suggesting a synergistic response in rats [46].
In the course of COVID-19 disease, it is likely that the antioxidant response is also explicitly changed since there is a clinical spectrum from asymptomatic to systemic inflammatory response syndrome. Recent data shows that lethal outcomes are related to age and underlying clinical conditions like diabetes and hypertension, which are prone to altered oxidant-antioxidant balance. SARS-CoV-2 itself also potentiates this already pathological antioxidant system. The virus uses the encoded protein of ACE2 as a functional receptor to enter cells. ACE2 catalyzes the cleavage of angiotensin II to vasodilator angiotensin 1–7. Angiotensin 1–7 mainly works as a blocker for SOD and decreases ROS, while angiotensin II promotes radical formation. Theoretically, SARS-CoV-2 blocks ACE2 and causes an increased ROS production with the help of increased angiotensin 2 levels [47]. Beyond this specific effect, SARS-CoV-2, as any infection, triggers a nonspecific inflammatory response from macrophages through activation of nicotinamide adenine dinucleotide phosphate (NADPH) oxidase, resulting in increased superoxide levels [48]. Increased ROS also damages host endothelial cells via inactivation of nitric oxide, resulting in thrombosis, which is also commonly in COVID-19.
As a result, in the treatment of COVID-19, controlling the inflammatory response may be as important as targeting the virus. Although there is no proven treatment for oxidative stress yet, routinely used immunosuppressive drugs like tacrolimus, CsA, and mTORi in kidney recipients may control the overreacted system. Further studies of oxidative stress management and to identify biomarkers would help us to triage patients with COVID-19 and underlying diseases like kidney transplantation.
There are several limitations of this review. The review has been built on mechanisms that are well understood in the pathogenesis of COVID-19. However, there may be many mechanisms that we still do not know about regarding the pathogenesis of COVID-19 and that may emerge later. Clinical studies on the effect of CNI and mTORi on the course of COVID-19 are lacking in the literature. Therefore, the present review is theoretical.
Conclusions
During the COVID-19 process, both CNI and mTORi may hypothetically have beneficial effects on kidney transplant patients. Immunosuppressants are not necessarily turned down for kidney transplant recipients in the pandemic of COVID-19. It is recommended to consider the pharmacological action of each immunosuppressive drug. Drug-comparative studies are needed on this subject.
References
1. Imam A, Abukhalaf SA, Imam R, Kidney transplantation in the times of COVID-19 – a literature review: Ann Transplant, 2020; 25; 1-16
2. Poulsen NN, von Brunn A, Hornum M, Cyclosporine and COVID-19: Risk or favorable?: Am J Transplant, 2020; 20; 2975-82
3. Moosavi SA, Mashhadiagha A, Motazedian N, COVID-19 clinical manifestations and treatment strategies among solid-organ recipients: A systematic review of cases: Transpl Infect Dis, 2020; 2; 1-10
4. Ulu S, Gungor O, Gok Oguz E, COVID-19: A novel menace for the practice of nephrology and how to manage it with minor devastation?: Ren Fail, 2020; 42; 710-25
5. Murakami N, Riella LV, Funakoshi T, Risk of metabolic complications in kidney transplantation after conversion to mTOR inhibitor: A systematic review and meta-analysis: Am J Transplant, 2014; 14; 2317-27
6. Lim WH, Eris J, Kanellis J, A systematic review of conversion from calcineurin inhibitor to mammalian target of rapamycin inhibitors for maintenance immunosuppression in kidney transplant recipients: Am J Transplant, 2014; 14; 2106-19
7. Budde K, Lehner F, Sommerer C, Conversion from cyclosporine to everolimus at 4.5 months posttransplant: 3-year results from the randomized ZEUS study: Am J Transplant, 2012; 12; 1528-40
8. Willicombe M, Thomas D, McAdoo S, COVID-19 and calcineurin inhibitors: Should they get left out in the storm?: J Am Soc Nephrol, 2020; 31; 1145-46
9. Suwelack B, Malyar V, Koch M, The influence of immunosuppressive agents on BK virus risk following kidney transplantation, and implications for choice of regimen: Transplant Rev, 2012; 26; 201-11
10. Sampaio MS, Cho YW, Shah T, Association of immunosuppressive maintenance regimens with posttransplant lymphoproliferative disorder in kidney transplant recipients: Transplantation, 2012; 93; 73-81
11. Xie X, Jiang Y, Lai X, MTOR inhibitor versus mycophenolic acid as the primary immunosuppression regime combined with calcineurin inhibitor for kidney transplant recipients: A meta-analysis: BMC Nephrol, 2015; 16; 1-13
12. Pascual J, Berger SP, Witzke O, Everolimus with reduced calcineurin inhibitor exposure in renal transplantation: J Am Soc Nephrol, 2018; 29; 1979-91
13. Pascual J, Berger SP, Chadban SJ, Evidence-based practice: Guidance for using everolimus in combination with low-exposure calcineurin inhibitors as initial immunosuppression in kidney transplant patients: Transplant Rev, 2019; 33; 191-99
14. Mühlbacher F, Neumayer HH, Del Castillo D, The efficacy and safety of cyclosporine reduction in de novo renal allograft patients receiving sirolimus and corticosteroids: Results from an open-label comparative study: Transpl Int, 2014; 27; 176-86
15. Maiese K, The mechanistic target of rapamycin (mTOR): Novel considerations as an antiviral treatment and possibilities for COVID-19: Curr Neurovasc Res, 2020; 17; 1-6
16. Batiuk TD, Halloran PF, The downstream consequences of calcineurin inhibition: Transplant Proc, 1997; 29; 1239-40
17. Duvoux C, Firpi R, Grazi GL, Recurrent hepatitis C virus infection post liver transplantation: Impact of choice of calcineurin inhibitor: Transpl Int, 2013; 26; 358-72
18. Mouy R, Stephan JL, Pillet P, Efficacy of cyclosporine A in the treatment of macrophage activation syndrome in juvenile arthritis: Report of five cases: J Pediatr, 1996; 129; 750-54
19. Nashan B, Gaston R, Emery V, Review of cytomegalovirus infection findings with mammalian target of rapamycin inhibitor-based immunosuppressive therapy in de novo renal transplant recipients: Transplantation, 2012; 93; 1075-85
20. Keating R, Hertz T, Wehenkel M, The kinase mTOR modulates the antibody response to provide cross-protective immunity to lethal infection with influenza virus: Nat Immunol, 2013; 14; 1266-76
21. Lehrer S, Inhaled biguanides and mTOR inhibition for influenza and coronavirus (review): World Acad Sci J, 2020; 176; 139-48
22. Felsenstein S, Herbert JA, McNamara PS, Hedrich CM, COVID-19: Immunology and treatment options: Clin Immunol, 2020; 215; 108448
23. Iwasaki A, Yang Y, The potential danger of suboptimal antibody responses in COVID-19: Nat Rev Immunol, 2020; 20; 339-41
24. Wang SF, Tseng SP, Yen CH, Antibody-dependent SARS coronavirus infection is mediated by antibodies against spike proteins: Biochem Biophys Res Commun, 2014; 451; 208-14
25. Yasui F, Kai C, Kitabatake M, Prior immunization with severe acute respiratory syndrome (SARS)-associated coronavirus (SARS-CoV) nucleocapsid protein causes severe pneumonia in mice infected with SARS-CoV: J Immunol, 2008; 181; 6337-48
26. Ruscitti P, Berardicurti O, Iagnocco A, Giacomelli R, Cytokine storm syndrome in severe COVID-19: Autoimmun Rev, 2020; 4; 102562
27. Banerjee D, Popoola J, Shah S, COVID-19 infection in kidney transplant recipients: Kidney Int, 2020; 21; 1-9
28. The Columbia University Kidney Transplant Program, Early Description of Coronavirus 2019 Disease in Kidney Transplant Recipients in New York: J Am Soc Nephrol, 2020; 51; 1150-56
29. Giamarellos-Bourboulis EJ, Netea MG, Complex immune dysregulation in COVID-19 patients with severe respiratory failure: Cell Host Microbe, 2020; 27; 992-1000e3
30. Maenaka A, Kenta I, Ota A, Interferon-γ-induced HLA Class II expression on endothelial cells is decreased by inhibition of mTOR and HMG-CoA reductase: FEBS Open Bio, 2020; 10; 927-36
31. Woo J, Propper DJ, Thomson AW, Antigen presentation and HLA-DR expression by FK-506-treated human monocytes: Immunology, 1990; 71; 551-55
32. Castro-Rojas CM, Godarova A, Shi T, mTOR inhibitor therapy diminishes circulating CD8+ CD28− effector memory T cells and improves allograft inflammation in belatacept-refractory renal allograft rejection: Transplantation, 2020; 104; 1058-69
33. Traitanon O, Mathew JM, La Monica G, Differential effects of tacrolimus versus sirolimus on the proliferation, activation and differentiation of human B cells: PLoS One, 2015; 10; 1-15
34. Iwasaki K, Kitahata N, Miwa Y, Suppressive effect of everolimus on IL-2, IL-10, IL-21, and IFNγ levels: Implications for the successful minimization of calcineurin inhibitor use in transplantation: Ther Drug Monit, 2019; 41; 371-75
35. Herrera-Gómez F, Vásquez-Seoane M, del Aguila W, Peripheral blood regulatory T cell counts as a predictive biomarker for the outcome of kidney transplant: A systematic review: Med Clin (Barc), 2017; 149; 523-35
36. Eleftheriadis T, Pissas G, Sounidaki M, In human cell cultures, everolimus is inferior to tacrolimus in inhibiting cellular alloimmunity, but equally effective as regards humoral alloimmunity: Int Urol Nephrol, 2017; 49; 1691-97
37. Gagné F, Oxidative stress: Biochemical Ecotoxicology, 2014; 36; 103-15
38. Aveles PR, Criminácio CR, Gonçalves S, Association between biomarkers of carbonyl stress with increased systemic inflammatory response in different stages of chronic kidney disease and after renal transplantation: Nephron Clin Pract, 2010; 116; c294-99
39. Treska V, Kobr J, Hasman D, Ischemia-reperfusion injury in kidney transplantation from non-heart-beating donor – do antioxidants or antiinflammatory drugs play any role?: Bratisl Lek List, 2009; 110; 133-36
40. Dawson TM, Steiner JP, Dawson VL, Immunosuppressant FK506 enhances phosphorylation of nitric oxide synthase and protects against glutamate neurotoxicity: Proc Natl Acad Sci USA, 1993; 90; 9808-12
41. Nito C, Ueda M, Inaba T, FK506 ameliorates oxidative damage and protects rat brain following transient focal cerebral ischemia: Neurol Res, 2011; 33; 881-89
42. Zadražil J, Štrebl P, Krejčí K, Effect of different calcineurin inhibitors on AOPP and TAS after kidney transplantation: Clin Biochem, 2010; 43; 559-65
43. Cvetković T, Veličković-Radovanović R, Stojanović D, Oxidative and nitrosative stress in stable renal transplant recipients with respect to the immunosuppression protocol – differences or similarities?: J Med Biochem, 2015; 34; 295-303
44. Zhang T, Guo J, Gu J, Protective role of mTOR in liver ischemia/reperfusion injury: Involvement of inflammation and autophagy: Oxid Med Cell Longev, 2019; 2019 7861290
45. Calap-Quintana P, Soriano S, Llorens JV, TORC1 inhibition by rapamycin promotes antioxidant defences in a drosophila model of friedreich’s ataxia: PLoS One, 2015; 10; 1-18
46. Singh AK, Garg G, Singh S, Rizvi SI, Synergistic effect of rapamycin and metformin against age-dependent oxidative stress in rat erythrocytes: Rejuvenation Res, 2017; 20; 420-29
47. Delgado-Roche L, Mesta F, Oxidative stress as key player in severe acute respiratory syndrome coronavirus (SARS-CoV) infection: Arch Med Res, 2020; 51; 384-87
48. Khomich OA, Kochetkov SN, Bartosch B, Ivanov AV, Redox biology of respiratory viral infections: Viruses, 2018; 10; 392
In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988