05 April 2022: Original Paper
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver Transplantation
Okjoo LeeDOI: 10.12659/AOT.935604
Ann Transplant 2022; 27:e935604






Abstract
BACKGROUND: Liver transplantation (LT) has been validated widely all over the world as the curative treatment for hepatocellular carcinoma (HCC). Statins have been reported to prevent the progression of HCC. There are many factors that affect recurrence of HCC, but the precise role of statins is unknown. Therefore, we examined whether statin therapy is associated with decreased HCC recurrence in patients who underwent living-donor LT (LDLT) for HCC.
MATERIAL AND METHODS: We retrospectively analyzed 844 HCC patients who underwent primary adult-to-adult LDLT in our center between January 2007 and December 2016. Statin therapy was defined as administration of statins for more than 30 cumulative defined daily doses (cDDDs) after LT. We compared HCC recurrence and patient survival between non-statin (n=334) and statin (n=52) groups.
RESULTS: The recurrence rate was higher in the non-statin group; however, time-dependent multivariate analysis with Kaplan-Meier curves showed that statin users did not significantly benefit in terms of HCC recurrence-related survival or overall survival. Further, risk factor analysis of HCC recurrence and patient survival confirmed multiple regional treatments (≥3 times), high alpha fetoprotein level (≥100 ng/mL), large tumor size (≥3 cm), and microvascular invasion as risk factors for HCC recurrence, but statin treatment was not associated with a significantly lower recurrence rate of HCC or reduced mortality after adjusting for other risk factors.
CONCLUSIONS: Statin use might be associated with prevention of HCC progression, but no significant decrease in HCC recurrence rates in LDLT patients was recorded in this study.
Keywords: 3-hydroxy-3-methylglutaryl-coenzyme A, Carcinoma, Hepatocellular, HMG-CoA reductase phosphatase, Liver Transplantation, Recurrence, Adult, Humans, Hydroxymethylglutaryl-CoA Reductase Inhibitors, Liver Neoplasms, Living Donors, Neoplasm Recurrence, Local
Background
Liver transplantation (LT) is established widely around the world as the only curative treatment for end-stage liver disease. Moreover, it is expected that LT not only can remove the tumor, but also cure the underlying liver disease. Therefore, LT can be a life-saving intervention in patients with hepatocellular carcinoma (HCC). However, although the survival rate of HCC patients treated with LT has improved steadily, recurrence of HCC remains an important clinical challenge. The first case of recurrent HCC after LT was reported in 1995 [1]. Recently, the recurrence rate of HCC after LT was estimated to range between 10% and 20%, with a median time to recurrence of 14 months after LT and a post-recurrence median survival period of 12.2 months [2–5]. In addition, at Samsung Medical Center, the median length of the recurrence-free period was 9.3 months (range, 0.89–97.25 months), and the median follow-up period after recurrence was 13.4 months (range, 0.59–118.28 months). The 1-, 3-, and 5-year survival rates after recurrence were 65.2%, 34.0%, and 20.5%, respectively [6,7].
Statins, which are 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors, have a long history of use as treatments for dyslipidemia and cardiovascular disease [8]. However, there has been emerging interest in the potential therapeutic application of statins as anticancer agents given their pro-apoptotic, antiproliferative, cell-cycle regulation, anti-invasive, and immunomodulatory effects [9–11].
For these reasons, many studies have sought to assess the effects of statins in patients with HCC. In previous research, statin use was associated with a reduction in the risk of HCC, and a meta-analysis showed that statin use was associated with a 37% lower risk of HCC [12,13]. Furthermore, statin use has been linked to reduced risk of HCC development in chronic hepatitis B virus (HBV)-infected patients, suggesting that statins have a chemopreventive role in this population [14,15].
However, relatively few studies have investigated the effect of statins on HCC recurrence in patients who underwent living-donor LT (LDLT) for HCC. One retrospective study showed that statin use was associated with a reduction in the risk of HCC recurrence in LT recipients [17]. However, that study included a heterogeneous donor spectrum of clinical conditions, including patients who underwent deceased-donor LT (DDLT). Statins might prevent HCC recurrence in LT recipients, but this association has not been studied fully in patients who underwent LDLT for HCC. Therefore, in the present study, we aimed to investigate the association between statin use and risk of HCC recurrence in LDLT recipients.
Material and Methods
STUDY POPULATION:
From January 2007 to December 2016, 844 LTs were performed at Samsung Medical Center (Figure 1). Patients with DDLT or multi-organ transplants (including simultaneous kidney grafts and re-transplantation) and pediatric transplants were excluded from this study (n=226). Additionally, 6 patients with missing follow-up data were excluded, leaving 386 patients in this study.
After enrollment, the study participants were divided into 2 groups, a no-statin-medication group (n=334) and a statin-medication group (n=52). We compared the HCC recurrence and patient survival rates between these 2 groups and conducted a risk factor analysis of HCC recurrence after LDLT.
LIVING-DONOR LIVER TRANSPLANTATION FOR HEPATOCELLULAR CARCINOMA:
In our center, we did not set strict criteria for liver transplantation in HCC patients. However, whether to perform LDLT was decided after the discussion of a multidisciplinary team, and HCC invading the main portal vein was considered a contraindication for transplantation. Living donors were selected among family members or relatives if the recipient did not have a matched donor within his or her family members. A graft-recipient weight ratio (GRWR) of 0.8% and future liver remnant of 30% were considered as the cut-off for donation.
USE OF STATINS:
According to pharmacokinetic features, statins are classified as either lipophilic or hydrophilic. Lipophilic statins include simvastatin, atorvastatin, fluvastatin, and lovastatin, whereas hydrophilic statins include rosuvastatin and pravastatin. Data on the prescription of statins during the study period were extracted from our electronic prescription databases. Statin dosage, type(s), date(s) of prescription, and cumulative number(s) were analyzed. The defined daily dose (DDD) is the standard dose of a statin recommended by the World Health Organization for measuring a prescribed amount of drug. The cumulative DDD (cDDD), which was calculated as the summation of the DDD values of all statins during the follow-up period, considered the exposure duration. Patients who used statins for at least 30 cDDDs during the follow-up period were defined as statin users. For patients who were taking statins before transplantation, the cDDD was counted from the first prescription after transplantation. Statin use and cDDD were considered as time-dependent covariates.
IMMUNOSUPPRESSION PROTOCOL:
Depending on routine induction medication, basiliximab was administered at a dose of 20 mg/day at the time of surgery and on the fourth postoperative day. All patients received triple immunosuppressive therapy regimens consisting of tacrolimus, mycophenolate mofetil, and methylprednisolone. Any patient who did not receive this regimen was excluded from the study. Tacrolimus (FK506, Prograf; Astellas Fujisawa, Osaka, Japan, and generic tacrolimus) was started on postoperative day 5 at 0.1 to 0.15 mg/kg/day and adjusted to maintain whole-blood trough level at 8 to 10 ng/mL for 1 month postoperatively and administered at 6 to 8 ng/mL until 3 months and tapered down thereafter. Mycophenolate mofetil (Myfortic; Novartis Pharma AG, Basel, Switzerland) was started at a dose of 500 to 1000 mg/day on postoperative day 3 and adjusted according to the general condition of the recipient considering the potential for opportunistic infection. Methylprednisolone was started on the day of surgery at an intravenous dose of 500 mg/day, administered for 2 days, and then tapered by half every day to 60 mg/day. Thereafter, oral methylprednisolone was administered at 32 mg/day for 7 days, at 16 mg/day for the next 2 weeks, at 8 mg/day for the next month, and at 4 mg/day for maintenance.
STATISTICAL ANALYSIS:
All variables are expressed as mean±standard deviation or number and percentage. Between-group differences of mean values were compared with independent
Results
BASELINE CHARACTERISTICS AND POSTOPERATIVE OUTCOMES:
A total of 386 patients who underwent adult LDLT between January 2007 to December 2016 were reviewed. The statin group (n=52) and non-statin group (n=334) were compared according to demographics and perioperative characteristics (Table 1).
Patients in the statin group were significantly older (55.85±7.33 vs 53.89±7.54 years;
Regarding operative and postoperative outcomes, the proportion of macroscopic fatty changes in the liver graft (8.50±7.01 vs 6.99±5.78; P=0.026) was greater in the statin group (Table 2). Operation and cold and warm ischemic times as well as pathologic outcomes did not differ between the 2 groups. Postoperative peak levels of liver enzymes were higher in the statin group than in the non-statin group (aspartate aminotransferase, AST, 463.56±507.85 vs 368.02±399.98, P=0.012; alanine aminotransferase, ALT, 461.56±363.76 vs 395.71±433.17, P=0.015). Postoperative complication rates were similar between the 2 groups.
The recurrence rate of HCC (9.62% vs 32.34%;
ANALYSIS FOR RECURRENCE OF HCC AND PATIENT SURVIVAL:
The cumulative recurrence rate was estimated using an extended Kaplan-Meier method that can be used with time-varying covariates (Figure 2). The Kaplan-Meier curve showed similar rates of HCC recurrence-related survival between the 2 groups (P=0.602). Furthermore, the results of cumulative overall survival analysis were similar between the 2 groups (P=0.203) (Figure 3).
Risk factor analysis of HCC recurrence was performed using Cox proportional hazard models (Table 3). Statin use and cDDD were considered as time-dependent covariates. Three or more locoregional treatments (hazard ratio [HR], 1.775, 95% confidence interval [CI], 1.204–2.616; P=0.004) tumor size ≥3 cm (HR, 1.570; 95% CI, 1.070–2.304; P=0.021), AFP level ≥100 ng/mL (HR, 1.912; 95% CI, 1.293–2.828; P=0.001), and microvascular invasion (HR, 3.408; 95% CI, 2.085–5.572; P<0.001) showed significant relationships with HCC recurrence. However, statin treatment was not associated with HCC recurrence after adjusting for other risk factors (HR, 0.929; 95% CI, 0.366–2.357; P=0.877). Regarding risk factors for overall survival, AFP ≥100 ng/mL (HR, 1.592; 95% CI, 1.068–2.372; P=0.022) and microvascular invasion (HR, 1.966; 95% CI, 1.287–3.002; P=0.002) were significantly related to poor prognosis, while statin treatment was not related to prognosis (HR, 0.388; 95% CI, 0.121–1.242; P=0.111) (Table 4).
Discussion
This study investigated the correlation between statin medication and HCC recurrence in patients who underwent LDLT for HCC. The possibility of administering statins as anticancer agents was evaluated, focusing on recurrence of HCC after LDLT. The background of this study was that several investigations have reported the beneficial impact of statin for various types of cancer [18–20]. Use of statin prior to allograft procurement of kidney transplant reduced the acute kidney inflammatory burden profile and promoted improved kidney function recovery following transplantation [21]. Hence, statins significantly reduced hyperlipidemia and tended to reduce cardiovascular events in kidney transplant recipients [22].
It is not definite which mechanism of statins contributes to prevention of HCC, although HMG-CoA reductase by statins can reduce concentrations of mevalonate pathway metabolites that are essential for cancer cell growth [23]. Various liver disorders, particularly cholestasis, affect cholesterol metabolism and can trigger variable levels of hypercholesterolemia, including the appearance of Lp-X. Mistaking Lp-X for low-density lipoprotein cholesterol can interfere with cardiovascular risk assessment, leading to prescription of futile lipid-lowering therapies [24]. Therefore, it was expected that statins would have a strong effect in the liver, which is a major organ that experiences inflammation caused by steatosis related to lipid metabolism.
However, our study showed no difference in recurrence-free survival rates between the statin and non-statin groups. While the statin group demonstrated a significantly lower recurrence rate (9.62% vs 32.34%;
While statins usually are well-tolerated, they often are associated with various statin-associated symptoms, including statin-associated muscle symptoms (SAMS), DM, and central nervous system problems [25]. SAMS are difficult to treat because there are no validated biomarkers or tests that can be used to confirm patient self-reports of SAMS, and a number of patients who report SAMS have nonspecific muscle pain not attributable to statin therapy [26]. Therefore, in clinical practice, the decision to prescribe statins should be made carefully so as not to result in their misuse or abuse in consideration of the above adverse effects. Furthermore, while the phenomenon of statins acting on lipid metabolism is well established in long-term cumulative studies, the use of statins as anticancer agents has not been established. Therefore, statin prescription with the expectation of an anticancer effect for preventing HCC recurrence should be considered after more evidence is gathered. Also, in transplant patients, it is necessary to determine whether there are any interactions or adverse effects due to long-term combined administration of immunosuppressant and statin.
A study by Cho et al reported a significant impact of statins on HCC recurrence after LT [17]. However, the population of the abovementioned study was 30% DDLT patients. Thus, our study is the only one to include elective LDLT patients with homogeneous donor factors. However, it is difficult to determine the difference between the results of these 2 similar studies based on the difference between LDLT and DDLT. There are well-known radiologic or pathologic risk factors, such as tumor size larger than the Milan criteria and vascular invasion, that were significant in our study. However, various biologic factors that were not measured in the 2 studies can lead to differences in their results. Recently, several laboratory findings, including AFP as a risk factor for recurrence of HCC, have been reported. The ratio of neutrophils to lymphocytes and des-γ-carboxy prothrombin were reported as postoperative independent risk factors associated with HCC recurrence [27,28]. Therefore, study of the relationships between these biologic markers and statins would be helpful in identifying their protective role in HCC recurrence.
There are some limitations to this study. First, it was a retrospective, single-center analysis with a cohort composed of Korean patients; therefore, the results might not be generalizable to other countries or continents. Second, all patients in the statin group had variable statin initiation, maintenance, and termination times after transplantation; however, the exact period and amount of statin exposure were evaluated and adjusted for the analysis. Third, a statistical technique with an on–off period was used, but there is a possibility that the calculated cDDD was different from the actual use. Next, using the retrospective cohort, adjustments were not made for several factors known to be associated with HCC recurrence risk, including alcohol intake, smoking, and family history of HCC. Nevertheless, our well-selected LDLT samples, time-dependent variable analysis to reduce immortal time bias, and careful adjustment for important factors are strengths of this study.
Conclusions
In conclusion, while recent studies have reported the anticancer potential of statin administration, our study, which included LDLT recipients with HCC, showed that the impact of statin administration after LT was not correlated with recurrence-free survival. As such, a large-scale, prospective, randomized study is needed to investigate the long-term outcomes of statin administration in patients who underwent LDLT for HCC.
Figures
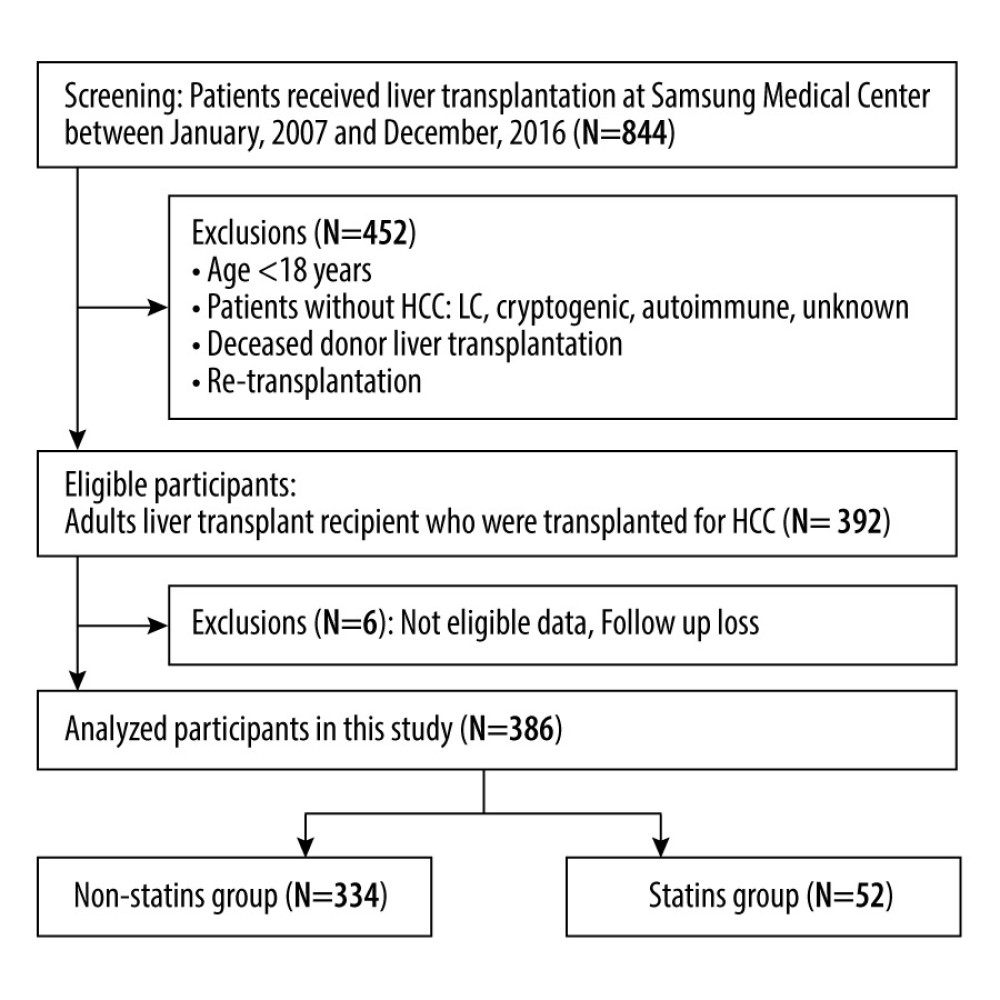 Figure 1. Patient selection.
Figure 1. Patient selection. 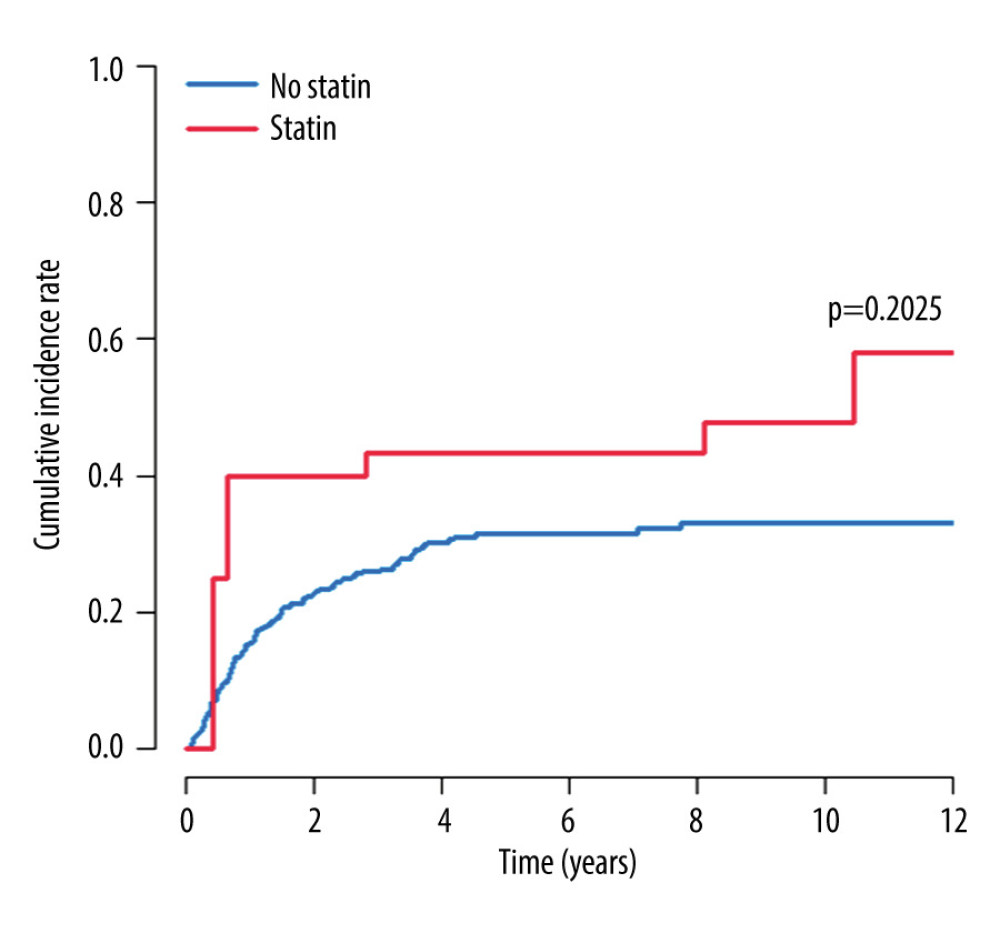 Figure 2. Cumulative recurrence rates estimated using an extended Kaplan-Meier method that can be used with time-varying covariates.
Figure 2. Cumulative recurrence rates estimated using an extended Kaplan-Meier method that can be used with time-varying covariates. 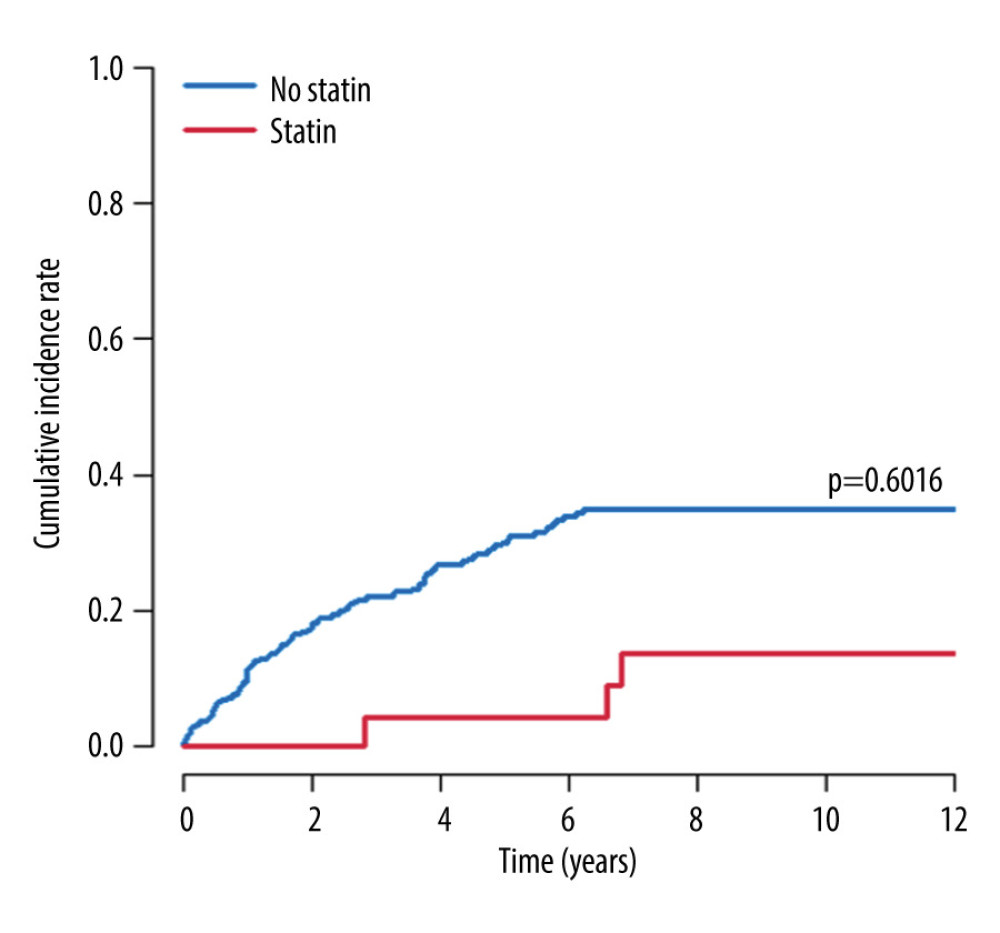 Figure 3. Cumulative overall survival rates estimated using an extended Kaplan-Meier method that can be used with time-varying covariates.
Figure 3. Cumulative overall survival rates estimated using an extended Kaplan-Meier method that can be used with time-varying covariates. References
1. Ringe B, Boker K, Schlitt HJ, Recurrence of hepatitis B virus cirrhosis and hepatocellular carcinoma: An indication for retransplantation?: Clin Transplant, 1995; 9(3 Pt 1); 190-96
2. Gabutti A, Bhoori S, Cascella T, Bongini M, Hepatocellular carcinoma recurrence after liver transplantation: Oncology (Williston Park), 2020; 34(3); 692516
3. Welker MW, Bechstein WO, Zeuzem S, Trojan J, Recurrent hepatocellular carcinoma after liver transplantation – an emerging clinical challenge: Transpl Int, 2013; 26(2); 109-18
4. de’Angelis N, Landi F, Carra MC, Azoulay D, Managements of recurrent hepatocellular carcinoma after liver transplantation: A systematic review: World J Gastroenterol, 2015; 21(39); 11185-98
5. Sapisochin G, Goldaracena N, Astete S, Benefit of treating hepatocellular carcinoma recurrence after liver transplantation and analysis of prognostic factors for survival in a large Euro-American series: Ann Surg Oncol, 2015; 22(7); 2286-94
6. Kim M, Rhu J, Choi GS, Risk factors for poor survival after recurrence of hepatocellular carcinoma after liver transplantation: Ann Surg Treat Res, 2021; 101(1); 28-36
7. Rhu J, Kim JM, Choi GS, Validation of the alpha-fetoprotein model for hepatocellular carcinoma recurrence after transplantation in an Asian population: Transplantation, 2018; 102(8); 1316-22
8. Baigent C, Blackwell LCholesterol Treatment Trialists’ (CTT) Collaboration, Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials: Lancet, 2010; 376(9753); 1670-81
9. Relja B, Meder F, Wilhelm K, Simvastatin inhibits cell growth and induces apoptosis and G0/G1 cell cycle arrest in hepatic cancer cells: Int J Mol Med, 2010; 26(5); 735-41
10. Cao Z, Fan-Minogue H, Bellovin DI, MYC phosphorylation, activation, and tumorigenic potential in hepatocellular carcinoma are regulated by HMG-CoA reductase: Cancer Res, 2011; 71(6); 2286-97
11. Pisanti S, Picardi P, Ciaglia E, Novel prospects of statins as therapeutic agents in cancer: Pharmacol Res, 2014; 88; 84-98
12. Singh S, Singh PP, Singh AG, Statins are associated with a reduced risk of hepatocellular cancer: A systematic review and meta-analysis: Gastroenterology, 2013; 144(2); 323-32
13. Li X, Liu L, Hu Y, Statin use and the prognosis of patients with hepatocellular carcinoma: A meta-analysis: Biosci Rep, 2020; 40(4); BSR20200232
14. Goh MJ, Sinn DH, Kim S, Statin use and the risk of hepatocellular carcinoma in patients with chronic hepatitis B: Hepatology, 2020; 71(6); 2023-32
15. Tsan YT, Lee CH, Wang JD, Chen PC, Statins and the risk of hepatocellular carcinoma in patients with hepatitis B virus infection: J Clin Oncol, 2012; 30(6); 623-30
16. Kim G, Jang SY, Nam CM, Kang ES, Statin use and the risk of hepatocellular carcinoma in patients at high risk: A nationwide nested case-control study: J Hepatol, 2018; 68(3); 476-84
17. Cho Y, Kim MS, Nam CM, Kang ES, Statin use is associated with decreased hepatocellular carcinoma recurrence in liver transplant patients: Sci Rep, 2019; 9(1); 1467
18. Voorneveld PW, Reimers MS, Bastiaannet E, Statin use after diagnosis of colon cancer and patient survival: Gastroenterology, 2017; 153(2); 470-9e4
19. Raymakers A, Sin DD, Sadatsafavi M, Statin use and lung cancer risk in chronic obstructive pulmonary disease patients: A population-based cohort study: Respir Res, 2020; 21(1); 118
20. Zhang Y, Liang M, Sun C, Statin use and risk of pancreatic cancer: An updated meta-analysis of 26 studies: Pancreas, 2019; 48(2); 142-50
21. Fuentes-Orozco C, Garcia-Salazar SJ, Gomez-Navarro B, Anti-inflammatory effect of atorvastatin on the kidney graft of living donor transplants: Ann Transplant, 2018; 23; 442-49
22. Navaneethan SD, Perkovic V, Johnson DW, HMG CoA reductase inhibitors (statins) for kidney transplant recipients: Cochrane Database Syst Rev, 2009(2); CD005019
23. Mullen PJ, Yu R, Longo J, The interplay between cell signalling and the mevalonate pathway in cancer: Nat Rev Cancer, 2016; 16(11); 718-31
24. Nemes K, Aberg F, Gylling H, Isoniemi H, Cholesterol metabolism in cholestatic liver disease and liver transplantation: From molecular mechanisms to clinical implications: World J Hepatol, 2016; 8(22); 924-32
25. Thompson PD, Panza G, Zaleski A, Taylor B, Statin-associated side effects: J Am Coll Cardiol, 2016; 67(20); 2395-410
26. Taylor BA, Thompson PD, Statin-associated muscle disease: Advances in diagnosis and management: Neurotherapeutics, 2018; 15(4); 1006-17
27. Meguro M, Mizuguchi T, Nishidate T, Prognostic roles of preoperative alpha-fetoprotein and des-gamma-carboxy prothrombin in hepatocellular carcinoma patients: World J Gastroenterol, 2015; 21(16); 4933-45
28. Halazun KJ, Najjar M, Abdelmessih RM, Recurrence after liver transplantation for hepatocellular carcinoma: A new MORAL to the story: Ann Surg, 2017; 265(3); 557-64
Figures
Tables
 Table 1. Baseline characteristics.
Table 1. Baseline characteristics. Table 2. Postoperative outcomes.
Table 2. Postoperative outcomes.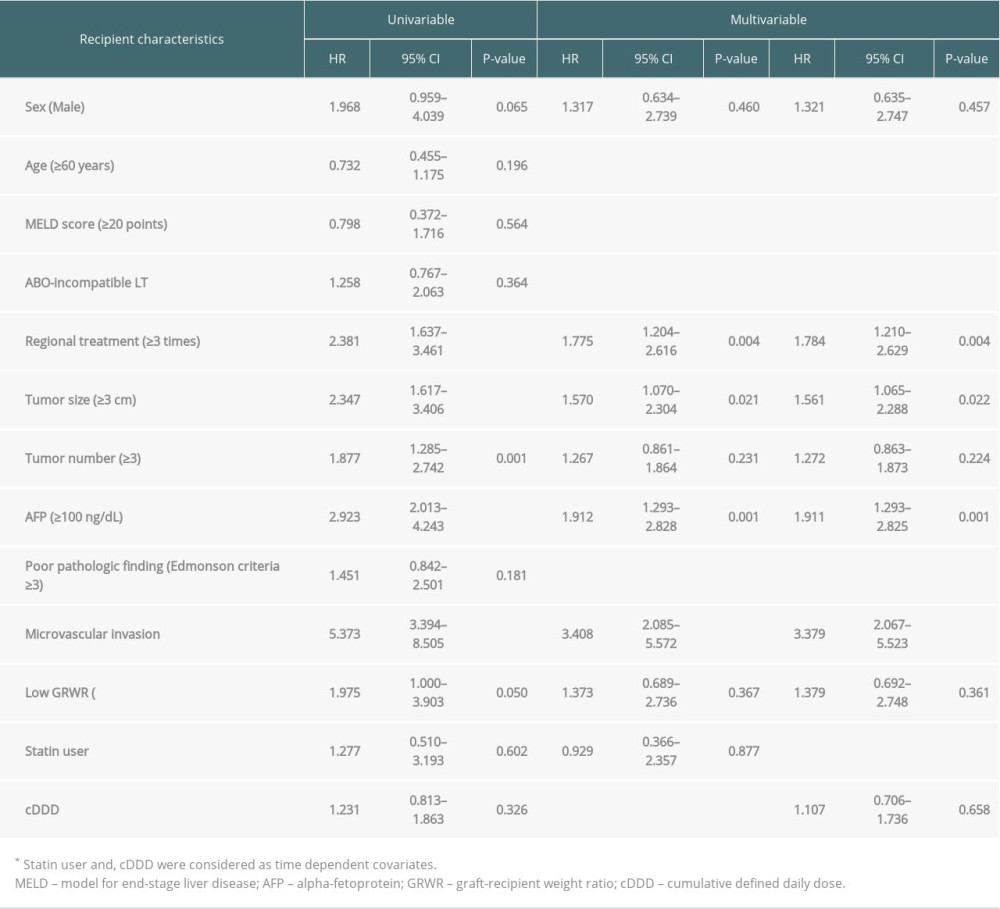 Table 3. The risk factors of hepatocellular carcinoma recurrence analyzed by Cox proportional-hazards regression models.
Table 3. The risk factors of hepatocellular carcinoma recurrence analyzed by Cox proportional-hazards regression models.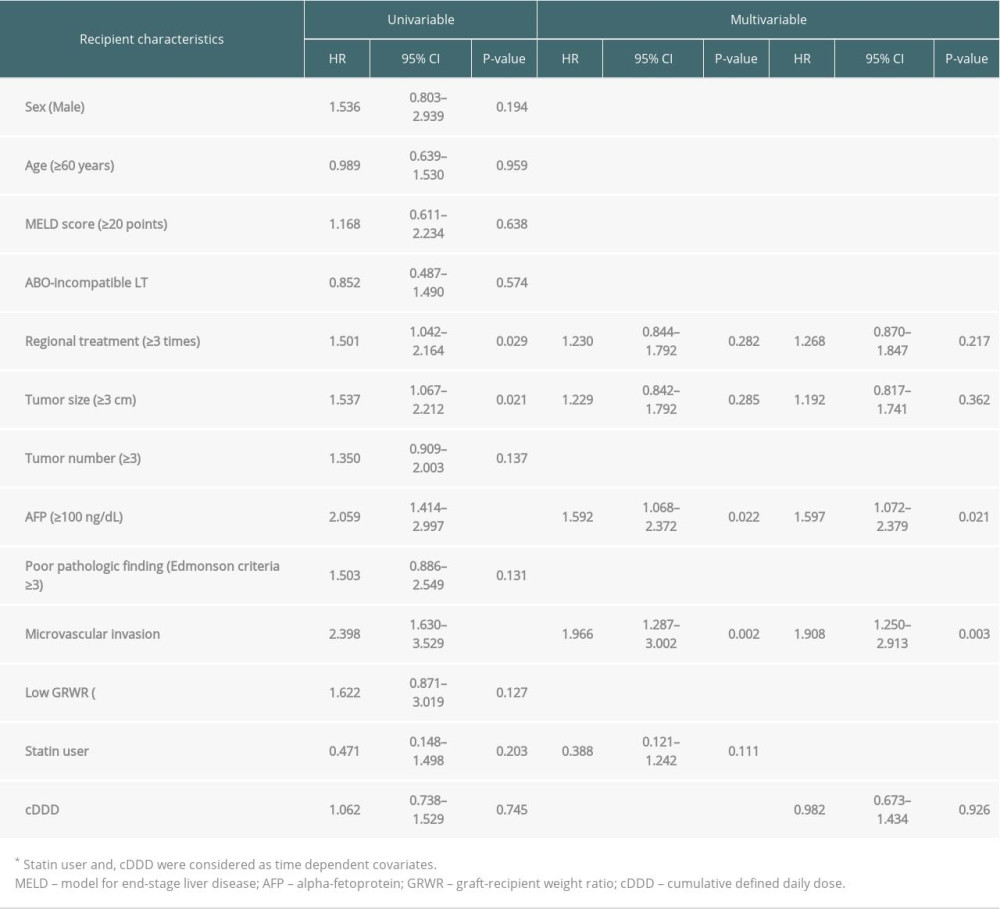 Table 4. The risk factors of patient survival analyzed by Cox proportional-hazards regression models.Table 1. Baseline characteristics.Table 2. Postoperative outcomes.Table 3. The risk factors of hepatocellular carcinoma recurrence analyzed by Cox proportional-hazards regression models.Table 4. The risk factors of patient survival analyzed by Cox proportional-hazards regression models.
Table 4. The risk factors of patient survival analyzed by Cox proportional-hazards regression models.Table 1. Baseline characteristics.Table 2. Postoperative outcomes.Table 3. The risk factors of hepatocellular carcinoma recurrence analyzed by Cox proportional-hazards regression models.Table 4. The risk factors of patient survival analyzed by Cox proportional-hazards regression models. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988