21 September 2021: Original Paper
Kidney Transplantation in Low- to Middle-Income Countries: Outcomes and Lessons Learned from Armenia
Sergey Babloyan12BCDE*, Milena Voskanyan3BC, Shant Shekherdimian4ADE, Helen Nazaryan3B, Sahak Arakelyan1D, Khachatur Kurkchyan5B, Poghos Geyikyan1B, Ara Babloyan12DF, Ashot Sarkissian67ACDEFDOI: 10.12659/AOT.930943
Ann Transplant 2021; 26:e930943






Abstract
BACKGROUND: Treatment of end-stage renal disease constitutes a heavy financial burden, especially in developing countries. Maintaining a kidney transplantation program is an extremely complex task in countries with limited resources. It often requires expertise and support from developed countries. Living donor kidney transplantations (LDKT) have been performed regularly in the Republic of Armenia since 2002. The purpose of this article is to review the history and outcomes of kidney transplantation in Armenia.
MATERIAL AND METHODS: A chart review was performed retrospectively on all patients who had undergone LDKT in Armenia. The key personnel involved in the development and operation of the unique kidney transplant program in the country were interviewed for a comprehensive review of the history and challenges of transplantation.
RESULTS: There were 172 LDKT (4 re-transplantations) performed between 2002 and 2019. The mean age of recipients was 35.9±13.4 years (range 7.1-65.7): 116 (67.4%) were male and 12 (6.9%) were children (<18 years). Seventy-four patients (43%) had peri- (n=5) and postoperative (n=69), mostly mild, surgical complications. Delayed graft function occurred in 17 (9.9%) patients, requiring hemodialysis in 16, and 6 patients stayed HD-dependant. Sixty-nine patients (40.1%) had at least 1 episode of acute rejection, with 26 (15.1%) having more than 1. Late complications were mostly infectious (n=49) or malignant processes (n=13). Follow-up studies showed that out of 172 patients, 126 had functioning grafts, 17 died with functioning grafts, 3 were lost to follow-up, and 26 lost grafts. Graft survival at 1, 3, 5, and 10 years, non-censored for death, after LDKT was 96.4% (CI 93.6-99.2), 93.7% (CI 89.9-97.5), 90.5% (CI 85.7-95.3), and 75.3% (CI 66.9-83.7), respectively.
CONCLUSIONS: Findings from this study suggest that a renal transplant program with acceptable outcomes can be successfully introduced in countries with limited resources.
Keywords: Armenia, Kidney Transplantation, Living Donors, Postoperative Complications, Adolescent, Child, Developing Countries, Female, Graft Rejection, Graft Survival, Humans, young adult
Background
Treatment of end-stage renal disease (ESRD) imposes a heavy financial burden, especially in countries with limited resources. Kidney transplantation (KT) is the most cost-effective option among renal replacement therapy modalities [1,2]. However, establishing a sustainable transplant program is an extremely complex task in countries with limited resources. It often requires expertise and support from developed countries. Studies describing the challenges of developing a KT program in low- and middle-income countries are scarce [3,4].
Armenia is a small, landlocked country (as part of the Union of Soviet Socialist Republics (USSR) from 1922 to 1991) that has recently gained independence (since 1991). It is located in West Asia with a population of around 2.9 million. The first 3 deceased donor kidney transplantation (DDKT) in Soviet Armenia were performed in the late 1970s followed by a small series in the 1980s. Outcomes concerning graft and patient survival were uniformly poor [5].
Upon becoming an independent state, 20 DDKT were performed between 1991 and 1995 with kidneys being transported from St. Petersburg (Leningrad), Russia. Results, with a few exceptions, were extremely unsatisfactory [5]. Despite unforeseen economic difficulties following the collapse of the USSR, the program continued to operate until the establishment of new customs regulations in 1995 which precluded access to deceased donor organs from abroad. The period that followed saw the development of a more organized KT program focusing exclusively on living donor kidney transplantations (LDKT), which exists to date. The purpose of this article is to review the history and outcomes of kidney transplantation in Armenia, focusing primarily on the LDKT program.
Material and Methods
A chart review was performed retrospectively on all patients who had undergone LDKT in Armenia. The key personnel involved in the development and operation of the unique kidney transplant program in the country were interviewed for a comprehensive review of the history and challenges of transplantation.
Microsoft Excel and life table analysis NCSS (v21.0.2) programs were used for statistical analysis. Results for continuous variables are expressed as mean ± standard deviation. The frequency of different complications (surgical, rejection episodes, infectious and oncological complications) were evaluated.
The graft and patient survival rates are expressed with their 95% confidence intervals (CI).
Results
HISTORY OF TRANSPLANTATION IN ARMENIA:
Armenia inherited many of the features of the former Soviet system. The Soviet healthcare system was highly centralized and guaranteed free medical assistance with access to secondary and tertiary care for the entire population. Nevertheless, certain services such as dialysis and KT were seriously underdeveloped and were available only in large centers such as Moscow and St. Petersburg.
Renal replacement therapy was non-existent in Armenia until a catastrophic earthquake in 1988 resulted in a large number of crush injuries and a robust international humanitarian response. Dozens of dialysis machines reached Armenia, and hemodialysis (HD) units were gradually established [6]. These initial successes were then offset by the collapse of the Soviet Union in 1991, which led to a deep financial crisis resulting in severe underfinancing of the health care system.
Currently, there are 13 HD centers, 5 of them in the capital city of Yerevan, with approximately 1000 patients receiving HD. All transplants take place at a referral center in Yerevan, with up to 20 transplants performed annually.
The first 3 DDKT in Soviet Armenia were performed in the late 1970s. According to the available information, 2 kidneys rapidly failed: one due to primary non-function and the other due to rupture. The third patient displayed preserved renal function 1 year after the operation, and then was lost to follow-up [5].
In the 1980s, a small series of KT were performed under the supervision of Russian specialists. Unfortunately, the follow-up data are not available.
The first successful pediatric KT was performed on May 16, 1991. A kidney from a deceased donor was transported from St. Petersburg. This was made possible by the establishment of an inter-institutional agreement which was widely in place during the Soviet period and which allowed for the exchange of organs [5].
Between 1991 and 1995, 20 deceased donor KT were performed, with poor results. Of 20 recipients transplanted from deceased donors (1991–1995), 8 (40%) had primary nonfunctioning grafts and 1 patient lost his graft due to hydronephrosis 3 months after KT. Six patients had functioning grafts with a median of 4.8 years (25% and 75%: 3.6 and 10.3 years). Two patients died with functioning grafts. Currently, 3 patients have functioning grafts >25 years. One-, 5-, and 10-year graft survival was 73%, 53%, and 33%, respectively.
The main cause of poor results in recipients from deceased donors was the high rate of severe acute rejection eventually leading to graft loss. The high incidence of severe acute rejection in that group has been associated with several factors such as long cold ischemia time (as no machine perfusion was available), lack of diagnostic methods, and important immunosuppressive medications as a result of the precarious economic situation and transportation problems in Armenia.
Beginning in 2002, with the support of colleagues from Belgium and Switzerland, LDKTs were performed. This was made possible by the introduction of HLA (human leukocyte antigen) matching, established through a partnership with the Armenian Bone Marrow Donor Registry Program.
In 2017 a new collaborative program with the International Society of Nephrology (ISN) and Guy’s Hospital (London) was established to expand the existing LDKT program and introducing DDKT.
TRANSPLANTATION DEMOGRAPHICS, EPIDEMIOLOGY, AND OUTCOMES:
Herein, we focus on data from 172 recipients who underwent KT between 2002 and 2019. Donors were the first-degree relatives (n=71; 41.3%), remote relatives (n=68; 39.5%), and spouses and emotionally related (n=33; 19.2%). During the first 5 years, there was a clear trend towards a continuous increase in the number of KT. Thereafter, there was some decline and further slight fluctuations at around 10 cases per year. In 2019, a record number of 20 transplantations were performed (Figure 1). Nevertheless, there is a need to increase KT volumes in Armenia (Figure 2).
Recipients’ characteristics were as follows: mean age: 35.9±13.4 years (range: 7.1–65.7), number of recipients in childhood (<18 years): 12 (6.9%), number of male recipients: 116 (67.4%). The mean age of the donors was 44.7±8.2 (28.6–65.0) years, with a female predominance (64.5%).
ETIOLOGY OF ESRD:
Primary kidney disease in 70 (40.7%) patients remained unknown. Twenty-seven (15.7%) patients had different types of glomerulonephritis, 21 (12.2%) had amyloidosis secondary to Familial Mediterranean Fever (FMF), 15 (8.7%) had congenital anomaly of kidney and urinary tract and reflux nephropathy, 8 (4.7%) had autosomal dominant polycystic kidney disease, 9 (5.2%) had renal involvement in vasculitis and systemic disorders, 5 (2.9%) had diabetic nephropathy, and 17 (9.9%) were other eg, hypertensive nephropathy, chronic allograft nephropathy, Bardet-Biedl Syndrome, Alport Syndrome (Figure 3).
Since colchicine was not widely available in the 1980s, patients with amyloid nephropathy constituted up to 10–15% of the entire dialysis population about 20–25 years ago. To not compromise the start of the transplant program, such patients (like those with diabetes mellitus) were not considered as candidates for renal transplantation in the 1990s due to the well-known number of adverse events complicating the post-transplant course. Later on, 21 patients with FMF and 5 with diabetes mellitus were transplanted, with comparable patient and graft survival rates.
PRE-TRANSPLANTATION TREATMENT:
One hundred sixty patients (93%) received HD, with a median duration of 9.8 months. Preemptive transplantation was performed in 12 patients (7%). There were no patients on peritoneal dialysis (no program exists yet in Armenia). Since 2002, all donors and recipients met inclusion criteria per European protocols adopted for Armenia [7].
IMMUNOSUPPRESSION:
Immunosuppression consists of triple therapy including steroids, calcineurin inhibitors (cyclosporine A or tacrolimus), and antimetabolites (azathioprine, mycophenolic acid or mycophenolate mofetil), purchased from the governmental budget. In addition, some patients with high immunological risks received induction with basiliximab. Since 2018, basiliximab is routinely used in all cases, but it must be purchased by patients out-of-pocket.
SURGERY:
The recipient’s kidneys were retrieved by open surgery in 159 cases and by laparoscopic technique in 13 cases. In most cases, 132 (76.7%) left donor kidneys were placed in the recipient’s right iliac fossa. The cold and warm ischemia times were 158.7±81.9 (range: 41–780) and 43.2±9 (range: 25–67) minutes, respectively. In 7 cases with supplementary kidney polar arteries, the warm ischemia time was 69.3±9.7 (range: 60–85) minutes. In 3 cases due to intraoperative vascular problems after reperfusion, kidneys were removed and re-implanted: in the same (n=2) and the contralateral side (n=1), and warm ischemia average time for these cases was 97.7±16.7 min. Ureteral implantations were performed using the Lich-Gregorie technique in 170 patients [8]. In 2 patients, ureteroureterostomies (end-to-side) with native right ureter were performed due to short ureter (in 1 case the damage of ureter was iatrogenic during donor-nephrectomy). Ureteral stents were placed during ureterovesical anastomoses or ureteroureterostomies in all cases except one, where the donor’s kidney had incomplete duplication of the collecting system. In another case, 2 stents were placed due to complete duplication of the collecting system. The mean period of stent removal was 11.9±7.8 (range: 3.4–46.8) weeks.
SURGICAL COMPLICATIONS:
There were 5 intraoperative complications (Table 1): bleeding from renal vein (n=3, 1.7%), detachment of iliac external artery intima with further thrombosis of transplant renal artery (n=1, 0.6%), and subcapsular hematoma with further rupture of the transplanted kidney at implantation (n=1, 0.6%).
The most common postoperative complication was the development of lymphoceles (n=47, 27.3%), most of which resolved spontaneously (n=36, 21%) (Table 1). Percutaneous aspiration was performed in 4 (2.3%) patients, external temporary drainage in 4 (2.3%), and laparoscopic fenestration/marsupialisation in 3 (1.7%) patients. The development of lymphoceles was observed, although in all cases the lymphatic ducts in the hilum of the donor’s kidneys, as well as during the mobilization of vessels for kidney implantation, were carefully tied.
Two patients (1.2%) had subcutaneous seromas with spontaneous absorption. Postoperative bleeding requiring recurrent interventions in 2 (1.2%) patients and bleeding with conservative management also in 2 (1.2%). Other complications were as follows: stenosis of distal ureter of transplanted kidney (n=2, 1.2%), necrosis of distal ureter (n=3, 1.7%), proximal stenosis of ureter (n=2, 1.2%), secondary wound healing (n=3, 1.7%), renal artery thrombosis (n=2, 1.2%), and arteriovenous (A-V) fistula formation after graft biopsy (n=1, 0.6%). All complications were managed, with good outcomes, except for renal artery thrombosis and A-V fistula formation leading to graft rupture.
MEDICAL COMPLICATIONS:
Overall, 69 (40.1%) patients had 1 episode of
The high level of rejections was due to difficulties with immunosuppressive medication supply. Seventeen patients (9.9%) had acute tubular necrosis (ATN), and 10 of them required HD. Prophylaxis of cytomegalovirus (CMV) infection is not routinely done due to the high cost. Thirty-one patients (18%) developed CMV disease (main symptoms were fever, malaise, and leukopenia), which is within the range (8–32%) reported in the literature in the absence of prophylaxis [9]. CMV was treated successfully in all patients, suggesting that this approach was warranted and could safely and significantly reduce the cost of KT.
Other infectious complications included pulmonary tuberculosis (n=1), varicella-zoster (n=5), herpes zoster (n=11), and measles (n=1). Varicella-zoster and measles in adult patients were a result of the interruption of the immunization program for some years in their childhood in the early 1990s. We had only 1 patient with post-transplant tuberculosis, which seems to be a major issue in developing countries, occurring in up to 15% of transplanted patients in Pakistan [4].
Thirteen patients (7.6%) had oncological complications, with 4 (2.3%) deaths.
PATIENTS AND GRAFT SURVIVAL:
We evaluated kidney graft and patient survival in 172 patients (as of July 2020): 126 patients had functioning grafts, and 26 patients lost grafts and went back to HD. Seventeen patients died with a functioning graft and 3 were lost to follow-up. The main reasons for graft loss were non-compliance (n=8) and rejection (n=6.2 of them had rupture of the graft), chronic transplant nephropathy (n=5), renal artery thrombosis (n=3.2 surgical complications and 1 hyperhomocysteinemia), and A-V fistula after biopsy (n=1).
Graft survival at 1, 3, 5, and 10 years, non-censored for death, after LDKT was 96.4% (CI 93.6–99.2), 93.7% (CI 89.9–97.5), 90.5% (CI 85.7–95.3), and 75.3% (CI 66.9–83.7), respectively (Figure 4).
Seventeen patients (9.9%) died with functioning grafts. Survival at 1, 3, 5, and 10 years was 98.8% (CI 97.1–100.0), 98.1% (CI 95.9–100.0), 96.4% (CI 93.2–99.5), and 87.1% (CI 80.2–93.9), respectively (Figure 5). The leading causes of death were cardio-vascular events (n=7) and cancer (n=4).
FINANCIAL CONSIDERATION:
All patients diagnosed with ESRD are treated exclusively with HD, creating a significant burden on the health care system. The mean annual treatment cost for HD is 6375 USD, which is typically reimbursed by the government. The mean total cost of KT during the first 12 months and annually thereafter were 8950 and 4150 USD, respectively. Furthermore, as most patients have decreased disability and increased ability to return to work, kidney transplantation offers additional economic benefits on a societal level.
Discussion
Patients with renal failure living in the developing world face many common obstacles, finally leading to the lack of transplantation activity. Notwithstanding, there are challenges unique for each country. In this paper, we presented problems we encountered and results we obtained during 18 years of LDKT in Armenia.
In more than half of recipients, the original kidney disease remained unknown. This was mainly due to late referral and poor control of hypertension and diabetes. Effective implementation of CKD screening could be a solution.
Unique to Armenia is the high prevalence of FMF. Renal amyloidosis is a serious complication of FMF if not prevented by colchicine.
Screening of potential recipients for donor-specific antibodies (DSA) must be implemented, especially for the development of DDKT. Currently, this is conducted through cooperation with Inselspital (Bern, Switzerland).
Another challenge was non-compliance with medications, leading to a high rate of rejection, which was the reason for graft loss in 8 recipients. The change of immunosuppressants used from syrups to capsules led to a significant decrease in such complications.
In our series, the majority of kidneys were removed by open surgery. The laparoscopic technique was implemented recently as appropriate equipment became available.
Seventy-four (43%) patients had surgical complications, which is relatively high compared to other series [10]. Fortunately, the most common complication, the formation of lymphocele in 47 (27.3%) patients, was a relatively minor one as most of them did not require any interventions and resolved spontaneously. Only 3 patients lost the grafts: 2 due to renal artery thrombosis and 1 due to A-V fistula formation after graft biopsy with further rupture of the graft.
A high incidence of oncological complications after KT was noted. Further assessments are warranted to determine the need for screening programs directed to early diagnosis and treatment.
Another challenge of Armenia’s KT program is infectious complications. Given the high cost of CMV prophylaxis, this practice is restricted to seronegative patients.
With all the aforementioned challenges and obstacles results of the LDKT program in terms of patient and graft survival are satisfactory and close to that of large transplant centers worldwide.
Finally, there is an increasing need for donor organs in Armenia, which can be alleviated by introducing a deceased donor transplantation program, as well as by increasing the volume of LDKT. Both of these initiatives would require a thorough assessment of capacity and acceptability.
In addition, numerous system-level challenges must be addressed to allow for a safe and effective DDKT program in Armenia. These include the development of appropriate legislation and policies to allow for deceased organ transplantation, the establishment of an organ donor network, identification of appropriate financing, and relevant training for personnel who will be involved in such a program.
Our study contains all of the inherent risks of a retrospective study design, including the potential for missing or inaccurate data. As transplantation continues to develop in Armenia, however, we hope that a national registry will be established to allow for prospective data collection and assessment.
Conclusions
Treatment of renal failure is challenging and often costly, particularly in resource-limited settings. Our data suggest that renal transplant programs with acceptable outcomes can be successfully and safely introduced in countries with limited resources. Moreover, KT offers cost savings starting from year 2 post-transplantation. The transplant program in Armenia is a good example of local stakeholder alignment along with effective international collaboration. Nevertheless, Armenia’s kidney transplant program is not comprehensive and robust enough to meet the needs of the country. Consideration should be given to expanding (with specific consideration to introducing a deceased donor program), improving quality and outcomes, and developing a prospective transplant registry.
Figures
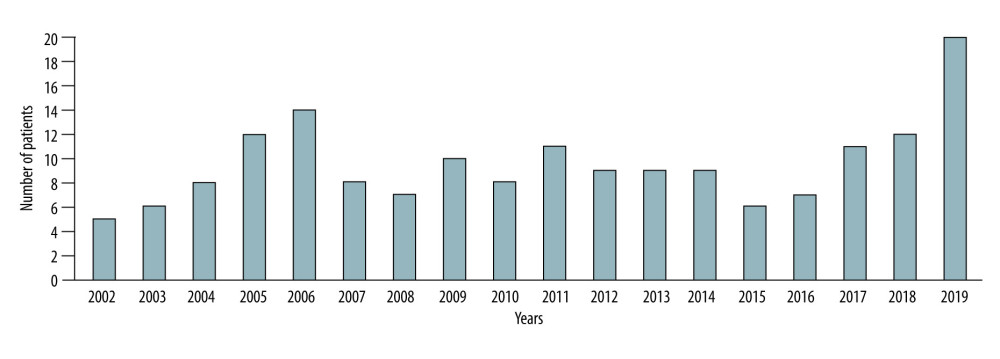 Figure 1. The number of living donor kidney transplantations per year (n=172).
Figure 1. The number of living donor kidney transplantations per year (n=172). 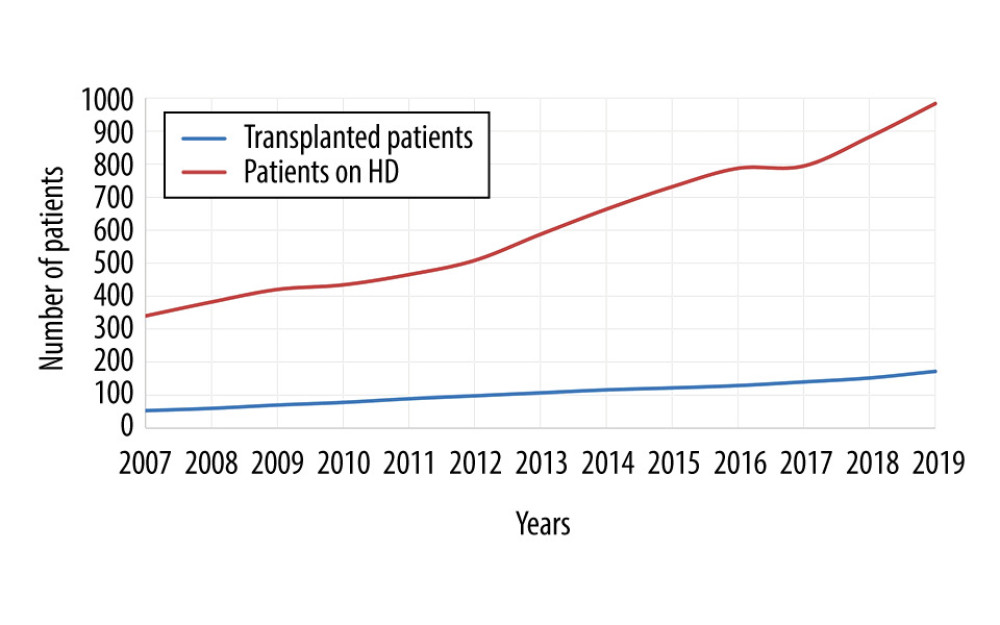 Figure 2. Increase in the number of patients awaiting transplantation as highlighted by trends in the number of transplants vs the number on HD.
Figure 2. Increase in the number of patients awaiting transplantation as highlighted by trends in the number of transplants vs the number on HD. 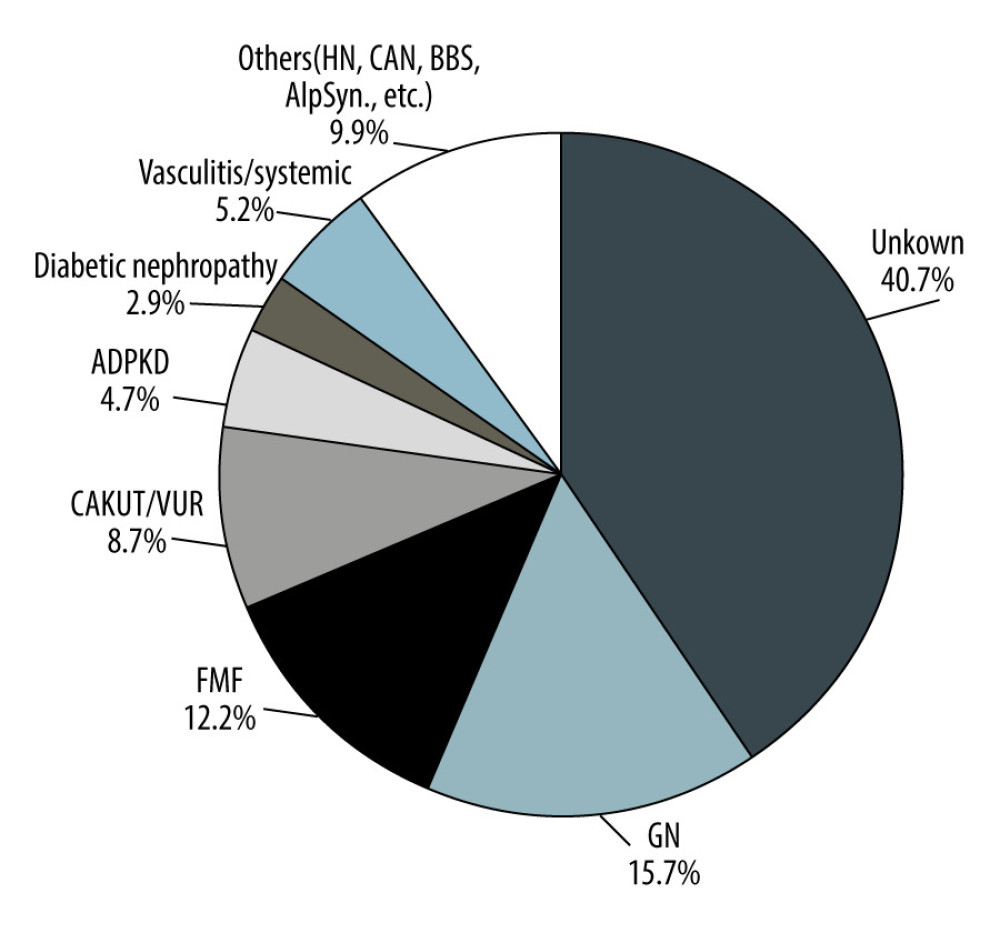 Figure 3. Etiology of end-stage renal disease among kidney transplant patients in Armenia. GN – glomerulonephritis; FMF – familial mediterranean fever; CAKUT/VUR – congenital anomalies of the kidney and urinary tract/vesicoureteral reflux; ADPKD – autosomal dominant polycystic kidney disease; Systemic – dsystemic disease; HN – hypertensive nephropathy; CAN – chronic allograft nephropathy; BBS – Bardet-Biedl syndrome; AlpSynd – Alport syndrome.
Figure 3. Etiology of end-stage renal disease among kidney transplant patients in Armenia. GN – glomerulonephritis; FMF – familial mediterranean fever; CAKUT/VUR – congenital anomalies of the kidney and urinary tract/vesicoureteral reflux; ADPKD – autosomal dominant polycystic kidney disease; Systemic – dsystemic disease; HN – hypertensive nephropathy; CAN – chronic allograft nephropathy; BBS – Bardet-Biedl syndrome; AlpSynd – Alport syndrome. 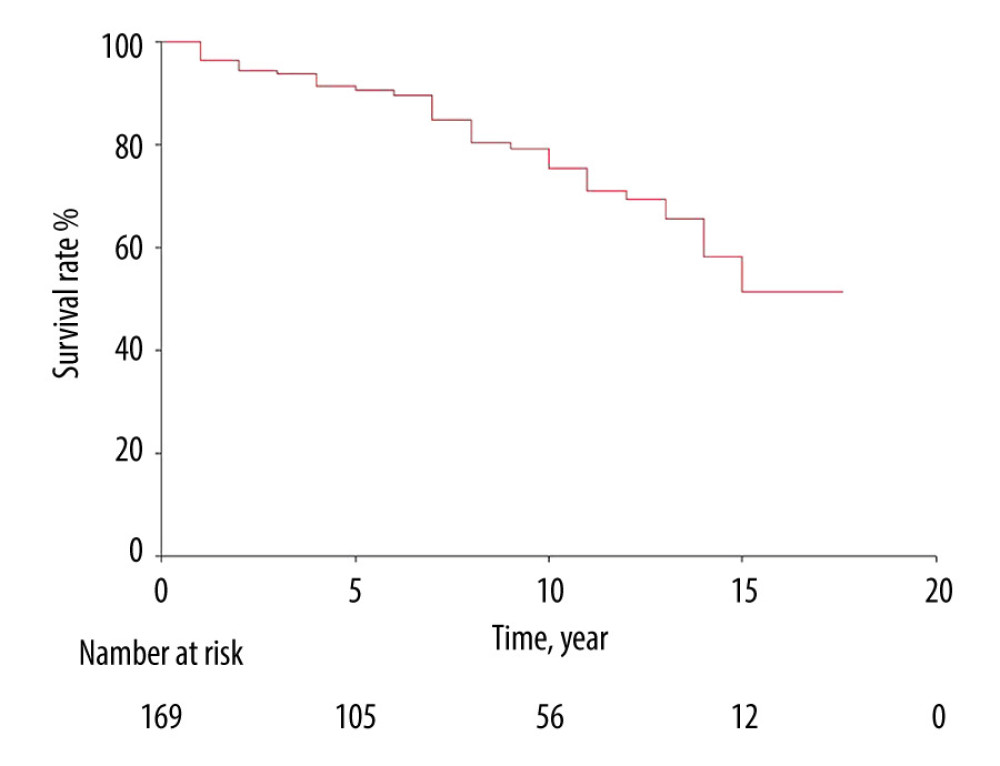 Figure 4. Graft survival in living donor kidney transplantation. The number at risk defines the number of patients in follow-up at each time point.
Figure 4. Graft survival in living donor kidney transplantation. The number at risk defines the number of patients in follow-up at each time point. 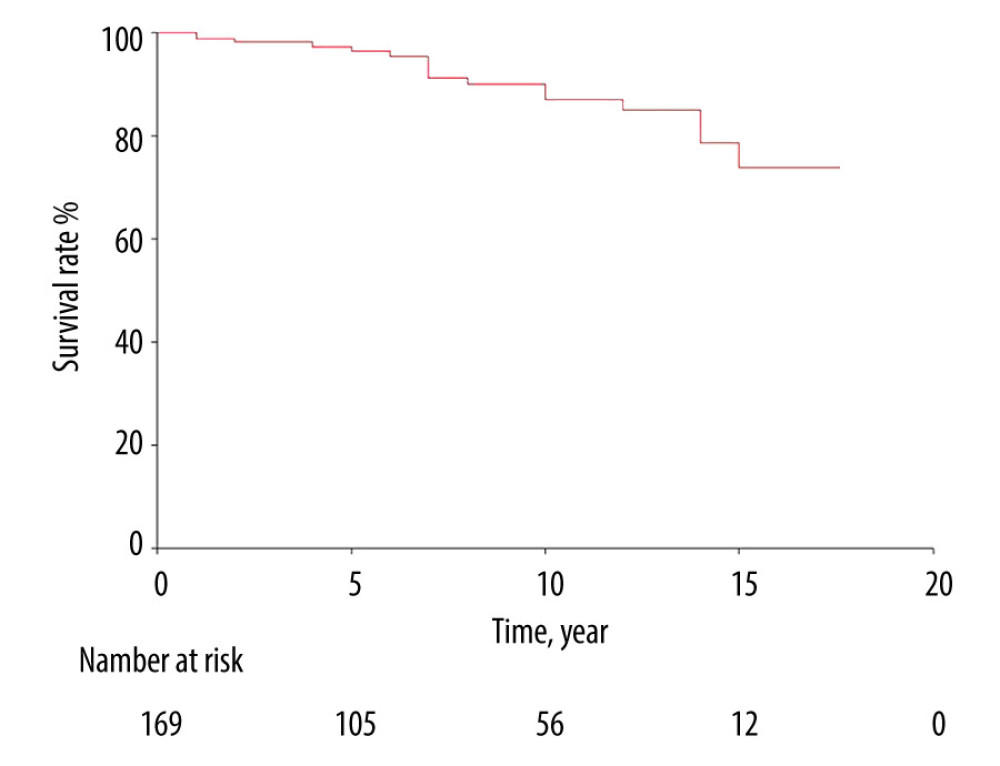 Figure 5. Patients’ survival in living donor kidney transplantation. The number at risk defines the number of patients in follow-up at each time point.
Figure 5. Patients’ survival in living donor kidney transplantation. The number at risk defines the number of patients in follow-up at each time point. 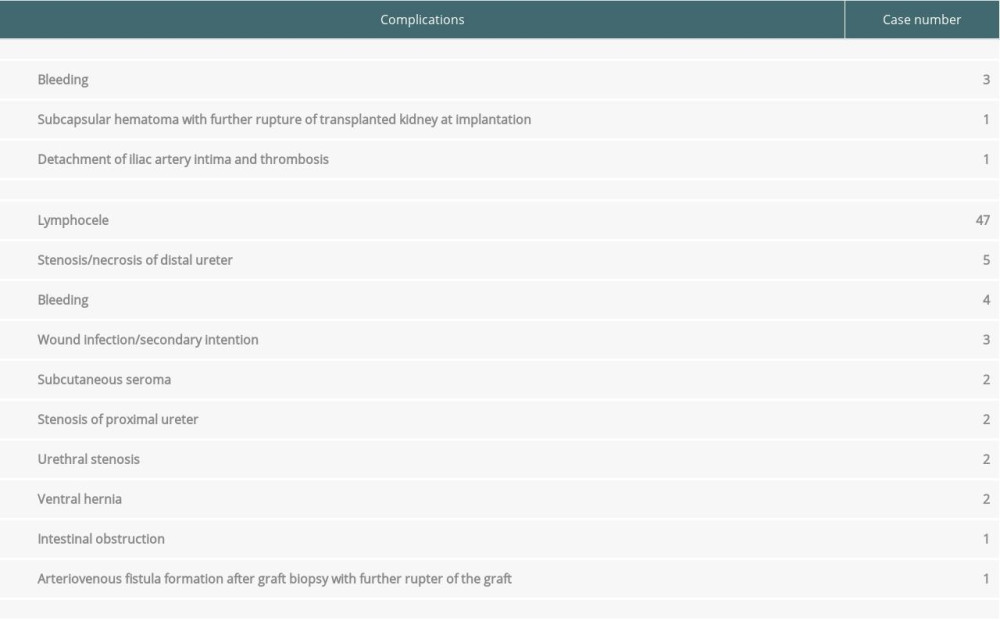
References
1. Jha V, Garcia-Garcia G, Iseki K, Chronic kidney disease: Global dimension and perspectives: Lancet, 2013; 382; 260-72
2. Abecassis M, Bartlett ST, Collins AJ, Kidney transplantation as primary therapy for end-stage renal disease: A National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQITM) conference: Clin J Am Soc Nephrol, 2008; 3; 471-80
3. Ready AR, Nath J, Milford DV, Establishing sustainable kidney transplantation programs in developing world countries: A 10-year experience: Kidney Int, 2016; 90; 916-20
4. Rizvi SAH, Naqvi SAA, Hussain Z, Renal transplantation in developing countries: Kidney Int, 2003; 6(Suppl 83); S96-100
5. Sarkissian A, Armenia: A history of first kidney transplantation – a European overview, 2019; 165-69, Budapest Semmelweis Publishers
6. Eknoyan G, Acute renal failure in the Armenian earthquake: Ren Fail, 1992; 14; 241-44
7. Abramowicz D, Cochat P, Claas FHJ, European Renal Best Practice Guideline on kidney donor and recipient evaluation and perioperative care: Nephrol Dial Transplant, 2015; 30; 1790-97
8. Lich RJ, Howerton LW, Davis LA, Recurrent urosepsis in children: J Urol, 1961; 86; 554-58
9. Simon DM, Levin S, Infectious complications of solid organ transplantations: Infect Dis Clin of North Am, 2001; 15; 521-49
10. Lempinen M, Stenman J, Kyllönen I, Salmela K, Surgical complications following 1670 consecutive adult renal transplantations: A single center study: Scand J Surgery, 2015; 104; 254-59
Figures
Figure 1. The number of living donor kidney transplantations per year (n=172).Figure 2. Increase in the number of patients awaiting transplantation as highlighted by trends in the number of transplants vs the number on HD.Figure 3. Etiology of end-stage renal disease among kidney transplant patients in Armenia. GN – glomerulonephritis; FMF – familial mediterranean fever; CAKUT/VUR – congenital anomalies of the kidney and urinary tract/vesicoureteral reflux; ADPKD – autosomal dominant polycystic kidney disease; Systemic – dsystemic disease; HN – hypertensive nephropathy; CAN – chronic allograft nephropathy; BBS – Bardet-Biedl syndrome; AlpSynd – Alport syndrome.Figure 4. Graft survival in living donor kidney transplantation. The number at risk defines the number of patients in follow-up at each time point.Figure 5. Patients’ survival in living donor kidney transplantation. The number at risk defines the number of patients in follow-up at each time point. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,843
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,003
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,082
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,052
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988