14 May 2024: Original Paper
Association Between FEV Decline Rate and Mortality in Long-Term Follow-Up of a 21-Patient Pilot Clinical Trial of Inhaled Liposomal Cyclosporine Plus Standard-of-Care Versus Standard-of-Care Alone for Bronchiolitis Obliterans Syndrome After Lung Transplantation
Aldo Iacono1ABDEF*, Marniker WijesinhaDOI: 10.12659/AOT.942823
Ann Transplant 2024; 29:e942823






Abstract
BACKGROUND: The association between forced expiratory volume in 1 second (FEV1) trajectory and mortality in bronchiolitis obliterans syndrome (BOS) is not well defined. Using long-term data from a prior clinical trial of inhaled liposomal cyclosporine A (L-CsA-I) for lung transplant patients with BOS, this study examined the association between longitudinal FEV₁ change and mortality.
MATERIAL AND METHODS: We analyzed long-term data from a clinical trial which randomized 21 patients with BOS (³20% decrease in FEV1 from personal maximum) to receive L-CsA-I plus standard-of-care (n=11) or standard-of-care (SOC) alone (n=10) for 24 weeks. A joint statistical model, combining a linear mixed model for FEV₁ change and Cox regression for mortality, was utilized to examine the overall association between FEV₁ trajectory and mortality during follow-up.
RESULTS: The 21 trial participants (10 single, 11 double lung recipients) had a mean FEV₁ of 1.7±0.6 Liters at randomization. Median follow-up post-randomization was 35 months. In joint model analysis, 1 percent FEV₁ decline predicted 1.076-fold increased mortality risk (95% confidence interval: -0.998 to 1.160, p=0.058). FEV₁ decline was reduced by 2.6% per year in L-CsA-I patients compared to SOC (p=0.210), and overall survival at 1/3/5 years was 91%/64%/27% vs 90%/20%/0% for L-CsA-I versus SOC, respectively (p=0.164).
CONCLUSIONS: In BOS patients, greater longitudinal FEV₁ decline predicts increased mortality. Trends towards prolonged stabilization of FEV₁ and improved survival were observed with L-CsA-I receipt. Further analyses will aid in evaluating the utility of FEV₁ change as a survival predictor, having implications in BOS management and future trial design.
Keywords: Lung Transplantation, Bronchiolitis Obliterans, Respiratory Function Tests, adult, Female, Humans, Male, Middle Aged, Administration, Inhalation, bronchiolitis obliterans syndrome, Cyclosporine, Follow-Up Studies, Forced Expiratory Volume, Immunosuppressive Agents, Liposomes, Pilot Projects, standard of care, Treatment Outcome
Introduction
Since the modern era of lung transplantation over 30 years ago, chronic lung allograft dysfunction manifesting as bronchiolitis obliterans syndrome (BOS) remains the single leading cause of long-term morbidity and mortality [1]. There are minimally effective approved therapeutic options to date to treat and prevent BOS after lung transplantation [1–3]. Approximately half of patients at risk develop BOS within 5 years following their lung transplant, and median survival after BOS onset is just 3–4 years [4]. A diagnosis of BOS and grade is made pursuant to a decline of ≥20% from the patient’s personal best measurement of forced expiratory volume in one second (FEV1), that is present for at least 3 weeks. A BOS grade of 1, 2, or 3 is assigned corresponding to an FEV1 decline of 20–34%, 35–49%, or ≥50%, respectively [4]. BOS, an obstructive phenotype of chronic lung allograft dysfunction, is a complex condition partly triggered by a pathogenetic alloresponse leading to epithelial injury causing bronchiolar fibro-obliteration and permanent FEV1 decline and eventually culminating in respiratory failure and death [4,5]. Unfortunately, no definitive treatment for BOS has substantially altered outcomes. The natural course of FEV1 after BOS demonstrates an increased decline within the first 6 months after the diagnosis. Female gender, single lung recipients and baseline interstitial lung disease patients appear to demonstrate increased FEV1 deterioration [6]. The degree of FEV1 impairment as a static percent of a best (maximum) post-transplant value and higher BOS grade correlate with increased mortality [7]. Absolute FEV1 has been identified as a predictor of mortality among lung transplant patients with BOS, as has short-term FEV1 change among hematopoietic stem cell transplantation patients with BOS; however, the relationship between long-term FEV1 trajectory (measured longitudinally for multiple years after BOS onset) and mortality has never been clearly examined in lung transplant patients with BOS [8].
A prior hypothesis of ours was that direct deposition of cyclosporine into inflamed airways of BOS using inhaled liposomal cyclosporine (L-CsA-I) may prevent progression of BOS and preserve pulmonary function. A prior open-label, single-center, pilot, randomized trial using L-CsA-I for BOS demonstrated improvement of overall survival, BOS progression-free survival, and lung function in patients randomized to L-CsA-I plus standard-of-care versus standard-of-care (SOC) alone [9]. In the current study that consists of secondary analyses of data from the aforementioned clinical trial, we hypothesized the following: 1) Rate of lung function decline after BOS will affect survival time; 2) A longstanding beneficial effect may occur following L-CsA-I exposure (although duration of treatment with L-CsA-I was merely 24 weeks).
The current study being reported analyzed lung function measurements from the aforementioned trial participants with BOS, which were collected for a median of 35 months (up to 7.5 years) from randomization. This study was designed to examine the evidence of a potential correlation between longitudinal FEV1 decline and patient survival time. The possible implications of this correlation include assisting in optimization of medical management, and supporting the use of FEV1 as a key surrogate endpoint in clinical trials of BOS since mortality is often not observed due to practical constraints such as limited follow-up durations and enrollment of less severely ill patients. Thus, the current study aimed to determine the association between longitudinal FEV1 change (percent change of FEV1 from randomization) and mortality using long-term follow-up data from a clinical trial which included 21 lung transplant patients (10 single lung and 11 double lung) with BOS.
Material and Methods
STUDY COHORT:
This is a nested study that consists of secondary analyses of extended data from an open-label pilot randomized clinical trial conducted at the University of Maryland School of Medicine. The study was approved by the University of Maryland’s Institutional Review Board (ClinicalTrials.gov NCT01650545). Written informed consent was provided by all participants in the L-CsA-I study prior to randomization. Patients ≥18 years of age were clinically diagnosed with BOS up to 4 weeks before study entry and were receiving tacrolimus-based immunosuppression. All patients met criteria for BOS grades 1 or 2 [10].
STUDY DESIGN:
The product under study was a drug–device combination: L-CsA-I and eFlow nebulizer system (PARI Pharma, Graefelfing, Germany). Both study groups received standard-of-care immunosuppression (SOC) while the L-CsA-I arm also received L-CsA-I twice a day for 24 weeks during the intervention period, and this was followed by a subsequent 24-week observation period during which SOC alone was continued in both groups [9]. Primary endpoints of the initial L-CsA-I study included 1) a composite endpoint of BOS progression-free survival, defined as time from randomization to ≥20% decline in FEV1, re-transplantation or death and 2) progression of BOS grade, defined by grade change from randomization. Details of the study procedures including randomization and allocation, statistical methods and analyses can be found in the initial study report [9]. The presently reported post-hoc long-term follow-up study included all patients enrolled in the initial randomized clinical study and involved collection of the standard clinical lung function tests used for clinical management at University of Maryland as well as survival time, death and cause of death for all cases. Follow-up for lung function and death was until April 11, 2019, having analyzed up to 25 serial pulmonary function tests (PFTs) per patient. The flow diagram summarizing the clinical trial design is shown in Figure 1.
INVESTIGATIONAL MEDICINAL PRODUCT AND TREATMENT REGIMENS:
L-CsA-I was provided in vials of 5 milligrams (mg)/1.25 milliliters (mL) and 10 mg/2.5 mL via an investigational eFlow nebulizer system (PARI Pharma, Graefelfing, Germany). Standard-of-care oral immunosuppression (SOC) included tacrolimus, mycophenolate mofetil and prednisone. Immunosuppression was adjusted according to University of Maryland standard protocols. Augmented immunosuppression consisting of corticosteroids or antithymocyte globulin was given for treatment of histological or clinical rejection.
TRIAL DESIGN AND OBJECTIVE:
The objective of the initial randomized open-label clinical study was to evaluate safety and efficacy of L-CsA-I for BOS grade 1 and 2. A clinical diagnosis of BOS was made based on a >20% decrease in FEV1 from the patient’s maximum post-transplant value. Patients had to be diagnosed within the prior 4 weeks to be enrolled in the study. Randomization was stratified according to single and double transplant status. Randomization characteristics, study design, power and statistical analyses are described in detail in the initial publication [9]. The Phase IIb study ended enrollments in 2015 and follow-up was for 12 months thereafter including PFTs until that date. Subsequently, lung function data and survival status have been collected for all patients until April 2019. Lung function was obtained according to University of Maryland protocol clinical follow-up schedule for lung transplant patients using American Thoracic Society (ATS) standards. Cause of death and BOS grade progression were also evaluated as data was extrapolated from clinic records.
ENDPOINTS:
The main objective of this study is to determine whether longitudinal changes of FEV1 would predict mortality risk. Other outcomes include: 1) FEV1 changes between L-CsA-I and SOC patients beyond the initial trial interval formally reported, 2) Progression to subsequent BOS grade; 3) Survival duration and cause of death.
LUNG FUNCTION MONITORING AND DATA COLLECTION:
All PFTs were performed within the clinical pulmonary function laboratories at the University of Maryland according to ATS standards [11]. PFT data were collected as part of the L-CsA-I trial or abstracted from the medical record after the trial had been completed. Follow-up includes demographics PFT data documented at approximately quarterly intervals depending on clinical status. Prebronchodilator FEV1 was expressed as absolute and percent predicted values [12]. FEV1 measurements for each subject were presented as spaghetti plots to provide a summary of individual patient lung function timepoints. FEV1 values per patient are expressed as both absolute milliliter change/month and percent predicted. These data were evaluated as initiation values at best post-transplant at randomization for each subject and at subsequent intervals to study termination in April 2019. Follow-up documentation includes the date and cause of a patient’s death or the date of each patient’s last visit if alive at study completion.
STATISTICAL ANALYSIS:
Patient characteristics are reported as means with standard deviations or percentages for categorical variables. To test the hypothesis that change in FEV1 was associated with mortality, a joint model consisting of a combination of a linear mixed model (LMM) for FEV1 trajectory and Cox regression analyses for mortality was used. This joint model represents the potential role of FEV1 as a mediator in the effect of treatment (L-CsA-I vs SOC) on mortality, while also accounting for the independent treatment effect of L-CsA-I vs SOC on mortality irrespective of FEV1, thereby enabling a more efficient and accurate assessment of the relationship between FEV1 and mortality [13]. For the LMM, FEV1 expressed as% of the personal best value observed between transplantation and randomization in the initial clinical trial was used as the dependent variable. All measurements of FEV1 taken between randomization and study termination were included in the analyses for predicting mortality risk. Single versus bilateral transplantation, BOS stage at inclusion, absolute FEV1 at baseline, age, sex, and linear time-by-treatment interaction (SOC or SOC+L-CsA-I) were included as covariates. Time to progression to a higher BOS grade, as well as overall survival, were assessed by Cox regression analyses. Joint modeling was performed using a function joint model of the R package JM version 1.4 8 [14]. All other statistical analyses were performed with IBM SPSS version 24 software.
Results
PATIENT CHARACTERISTICS:
21 patients with BOS grades 1 or 2 were enrolled in the clinical trial that is the data source for this study. Patients were randomized as follows: 11 to receive L-CsA-I plus SOC, and 10 to receive SOC alone. Patients in both groups had similar baseline characteristics (Table 1) and time from transplantation to BOS onset (L-CsA-I group vs SOC group respectively, 1391±859 days versus 1061±796; p=0.41). All 21 patients had PFT and mortality data during study follow-up available, and if expired, cause of death was reported.
:
All PFT data during the entire observation period, from randomization in the clinical trial until death or last contact for each patient were included in analyses, with a median observation period of 35 months (L-CsA-I 49 months, SOC 34 months). Number of PFTs ranged between one (this patient was excluded as no follow-up for trajectory was available) and 26 per patient. Sixteen patients (76.2% of 21) contributed more than 10 serial PFT assessments.
Mean±Standard Deviation (SD) FEV1 at randomization was 1.66±0.56 l for L-CsA-I vs 1.78±0.60 l for SOC alone (p=0.65), and subsequently 1.49±0.64 vs 1.51±0.60 L after one year (p=0.36), and 1.75±0.98 vs 1.15±0.49 L after 2 years’ follow-up (p=0.28) respectively (last observation carried forward). By the end of the third year, there were only 2 patients with FEV1 assessments remaining in the SOC group (compared to 7 in the L-CsA-I group) so averaging data is not meaningful.
The individual patients’ FEV1 trajectories, expressed relative to their personal post-transplant maximum FEV1, are shown in Figure 2, stratified by treatment group (L-CsA-I or SOC) and transplant type (single or double). These trajectories indicate a great diversity of idiosyncratic trends over the course of time, with many subjects showing a gradual deterioration of FEV1, and others exhibiting a rapid decline, while still others showed stabilization or even improvement during the study. For the overall analysis population, FEV1% of the individual maximum value decreased at a rate of 2.9% per year (LMM, factor ‘time’: p=0.007) over the entire observation period. Only a linear association between change in FEV1 and time could be investigated, as analyses with higher-order polynomials did not converge due to the small sample size and follow-up attrition.
:
Baseline FEV1 was positively associated with FEV1 during follow-up, with each 1 mL less of FEV1 at baseline being associated with an average of 0.013% lower FEV1 during follow-up (p<0.001). Moreover, compared to BOS grade 1 at baseline, a grade of 2 predicted a 9% lower FEV1% of the personal best value during follow-up (p=0.007). Males showed an average of 9.4% lower FEV1% of the personal best compared to females (p=0.018). A time-by-treatment interaction was found, according to which the FEV1% of personal best decline in the patients treated with L-CsA-I was delayed by 2.6% per year compared to SOC, even though the effect did not reach formal statistical significance (p=0.210). Patient age and type of transplant did not significantly alter the rate of decline of FEV1.
:
Assessing the longitudinal impact of change of FEV1 trajectory and survival, according to a joint model based on LMM and Cox regression analysis, demonstrated a marginally significant association between% change in FEV1 from maximum and survival (p=0.058) (Figure 3). According to the model, a 1% decline in FEV1 from the personal best is associated with a 1.076-fold increase in mortality risk (95% confidence interval: 0.998 to 1.160). Accordingly, when the difference between any 2 individuals in FEV1% of maximum is 10%, the predicted mortality risk of the individual with the lower value for FEV1% of maximum is increased by 1.07610=2.080, corresponding to a predicted increase by 108%.
PROGRESSION OF BOS STAGES AND PATIENT SURVIVAL:
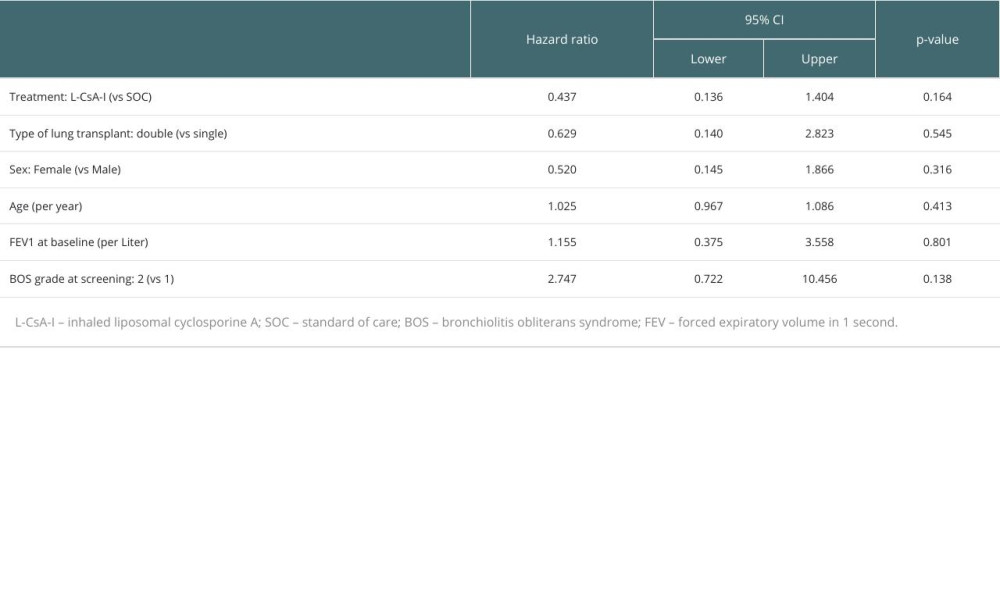
Of the 21 patients in the trial, 9 (42.9%) progressed to a higher BOS grade during follow-up. Subjects with a higher FEV1 (p=0.052), single lung transplant (p=0.061), and female sex (p=0.072) tended to be more likely to progress to a higher BOS grade. Cox regression analysis of overall survival (Table 2) showed that a lower BOS grade at screening (p=0.138) and treatment with L-CsA-I (p=0.164) were the most important predictors of improved long-term survival in the study population, though not reaching statistical significance. Among the 21 randomized subjects, 3 of 11 in the L-CsA-I group (27.3%) but none in the SOC group were alive at the end of the follow-up. Overall survival rates at 1/3/5 years were 91%/64%/27% in the L-CsA-I group versus 90%/20%/0% in the SOC group. Chronic rejection was the cause of death in almost all deceased patients, except for one patient in the L-CsA-I group who died from a malignant skin tumor, and one patient in the SOC group who died from bacterial septicemia. For the surviving patients in the L-CsA-I group, the last follow-up was 71.7–88.8 months after baseline.
Discussion
The principal finding of this study was the association between greater rate of decline in FEV1 and increased risk of death in patients with BOS after lung transplantation. Each 1% decline in FEV1 was predicted to increase the risk of death by 7.6%. Although statistical significance by conventional standards was narrowly missed for this association (p=0.055), due to the limited sample size (the study was not powered for achieving significance in this post-hoc analysis), the effect size is notable, and this finding may form the basis for future larger scale analyses exploring this important relationship. We elaborate upon the previously known relationship between lower absolute FEV1 and increased mortality [15], but here demonstrate a correlation between progressive FEV1 decline rate and mortality, with the most marked longitudinal decreases in FEV1 being associated with the highest risk of survival reduction.
A second point is that a time-by-treatment interaction was observed, showing a more profound FEV1 decline with standard immunosuppression as compared to L-CsA-I plus standard immunosuppression (even though the effect was statistically non-significant). This highlights a potential benefit of L-CsA-I even after L-CsA-I was discontinued following the treatment duration of 6 months only, and gives further credence to the initial trial results. A recently completed phase III international randomized trial using L-CsA-I for BOS modeled off of this Phase II study will further elucidate the aforementioned subject (NCT03657342; NCT03656926). Furthermore, a study using L-CsA-I for BOS prophylaxis (as opposed to treatment of BOS as in the current study) similarly demonstrates a correlation between FEV1 longitudinal deterioration and mortality in lung transplant recipients receiving L-CsA-I soon after transplantation for rejection prevention [16].
Those patients with a reduced baseline FEV1 or higher BOS grade at randomization, and female gender, were more likely to experience a rapid decline in FEV1 values compared to the remaining patients. Approximately 90 percent of our study recipients ultimately expired from a final chronic rejection diagnosis indicating homogeneity of the population and precision of the baseline populations’ BOS diagnosis. The results of our study appear consistent with prior findings that absolute FEV1 is associated with mortality in lung transplant patients with BOS, and FEV1 change is associated with mortality in hematopoietic stem cell transplant patients with BOS [8].
BOS as a chronic lung allograft dysfunction phenotype is characterized by a complex immunological process of bronchiolar inflammation and a fibroproliferative response resulting in bronchiolar injury and sustained FEV1 decline. The diagnosis of BOS is based on FEV1 reduction from best post-transplant baseline values and absence of a concomitant restrictive ventilatory defect [17]. Absolute FEV1 reductions have been identified as a definitive prognostic marker in BOS after lung transplant. Differences in rates of loss of lung function have been linked to post-transplant time of BOS diagnosis, BOS grade, sex, pretransplant underlying disease and type of transplant [17,18]. However, longitudinal FEV1 change has not been specifically examined as predictor of mortality in lung transplant patients with BOS, although a consistent increase in the risk of death has been associated with the absolute FEV1 decrease based on BOS grade [18,19].
In the initial phase of the reported trial, L-CsA-I plus standard-of-care or standard-of-care alone was administered for a total duration of 6 months after study randomization, and all patients received standard-of-care exclusively afterwards for an additional 6 months (12 months total trial duration) [9]. The latter study showed improved graft survival and FEV1 preservation, results consistent with other trials using aerosol cyclosporine in lung transplant recipients for rejection prevention and treatment [20,21]. In the present extended follow-up analysis of this trial, these clinical trial participants were followed for an average duration of 35 months to examine the relationship between their longitudinal FEV1 changes and survival times. A trend towards improvement of lung function and outcomes was again noted in association with L-CsA-I despite prolonged time elapsed since the discontinuation of the drug.
Since there are no laboratory markers to date that can accurately predict a prognosis for BOS progression and the course is typically variable, new methodologies to prognosticate are required to enhance clinical acumen. Longitudinal evolution of FEV1 has potential implications for patient care and clinical trial design. It would be beneficial to be able to predict mortality based on a defined trajectory of FEV1 after BOS onset rather than an absolute irrevocable decline (grade 3) limiting treatment options at that explicit point when irreversible lung disease progression and airway obliteration has already occurred. An early marker of BOS progression would facilitate patient management in real time clinical practice and in trial design as a surrogate marker of an evolving severe outcome.
This study, which is comprised of secondary analyses of data from a Phase IIb clinical trial, has several limitations. As a pilot trial the small sample size leads to the study being statistically underpowered and possibly limited in generalizability, although trends in FEV1 and survival show promise to justify completion of a current international Phase III trial using L-CsA-I for BOS. The observed trend of long -term functional and survival improvement in our current analysis will need to be corroborated by future larger scale trials using L-CsA-I. In addition, the analyses in this study fail to account for the possibility that clinical parameters related to or correlated with FEV1 may confound, modify, mediate, or otherwise affect the true association between FEV1 decline rate and mortality, Furthermore, although the joint model approach used appears to be the most appropriate for examining the association between FEV1 trajectory and mortality in this case, it assumes that the structure of the FEV1 trajectories (i.e. linear function of time) is generally common to both treatment arms, which may not be an entirely justifiable assumption. A strength of the study is that the FEV1 measurements for each patient were generally collected on a frequent and consistent basis due to being part of a clinical trial. Additionally, due to the rapid enrollment of patients in the clinical trial soon after diagnosis of BOS, along with the long-term follow-up which typically continued for the remainder of the patient’s lifetime, the full length of illness with BOS (from diagnosis until death) was captured in this study for the vast majority of patients enabling an accurate and comprehensive ascertainment of the relationship between FEV1 decline and mortality in this population.
Conclusions
Our long-term analysis of this Phase II study using L-CsA-I found that the longitudinal change of FEV1 predicts mortality in patients randomized with BOS. Additionally, advantageous long-term trends for L-CsA-I randomized BOS cases versus SOC were observed by stability of FEV1 and survival time. These results will be further elucidated by the forthcoming interpretation of data from the recently completed randomized – controlled -Phase III international study using L-CsA-I for chronic lung allograft dysfunction. Ideally longitudinal changes of FEV1 may be used to prognosticate outcomes of BOS and specifically tailor therapeutic immunosuppressive algorithms.
Figures
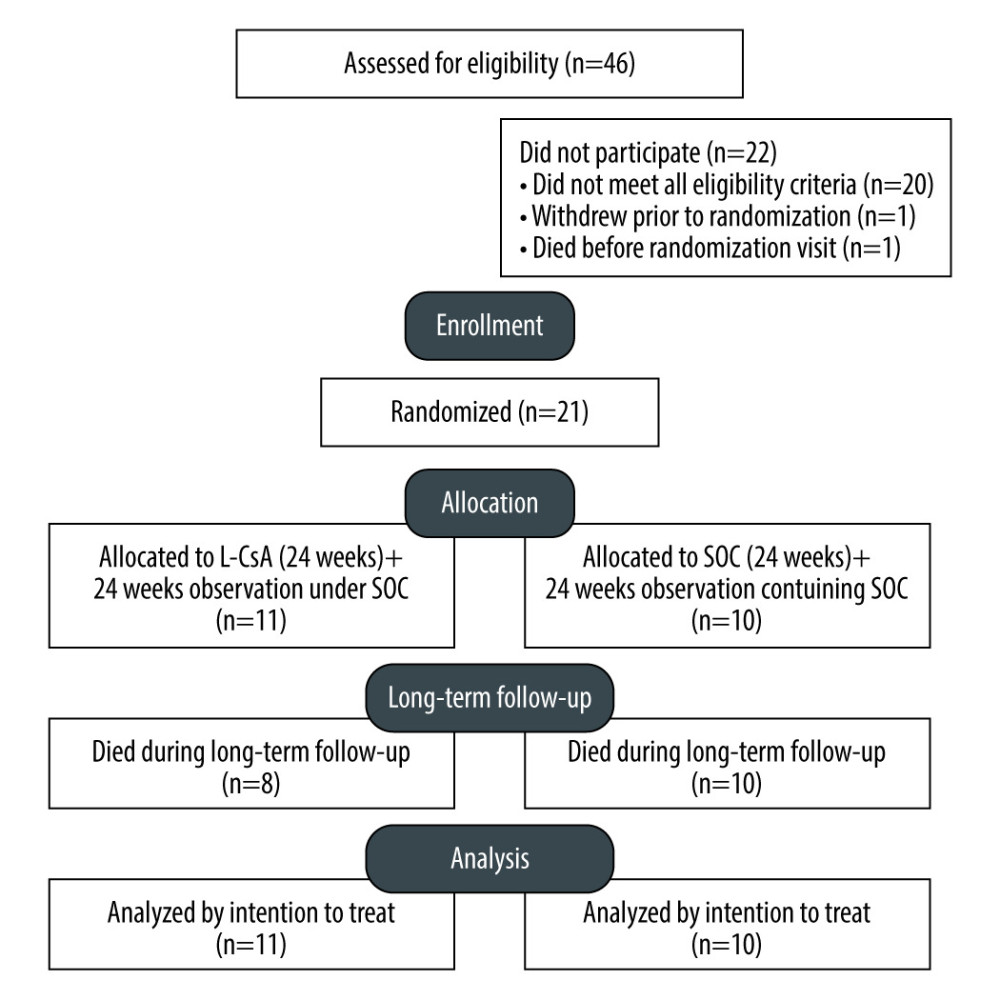 Figure 1. Flow diagram depicting study design.
Figure 1. Flow diagram depicting study design. 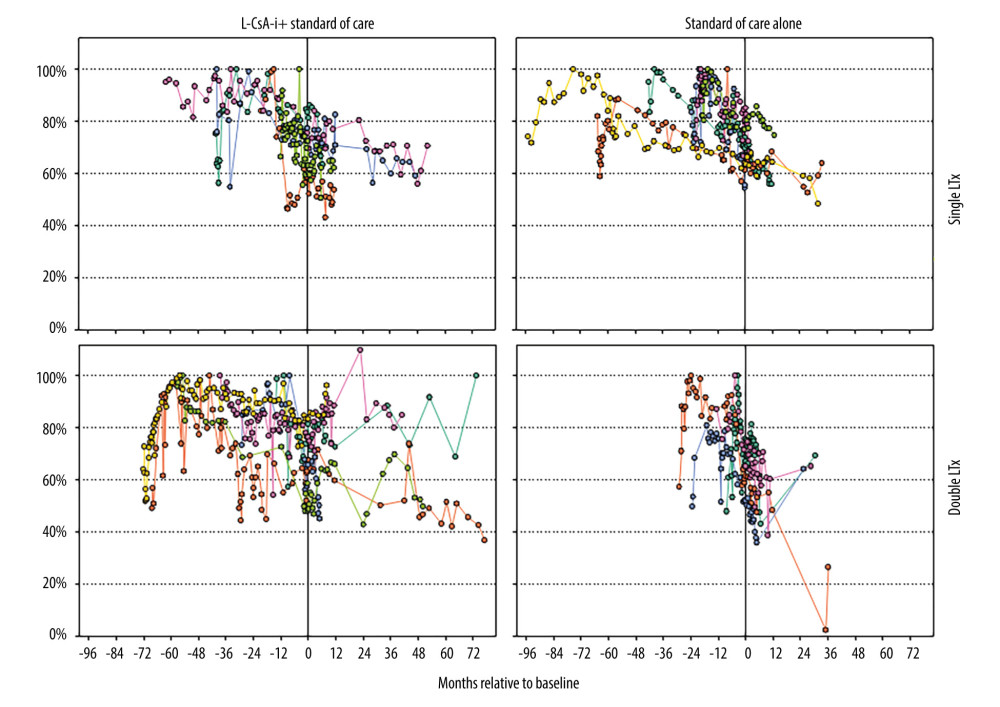 Figure 2. Trajectories of forced expiratory volume in 1 second (FEV1) for individual subjects, from transplantation to end of follow-up. FEV1 trajectories are plotted in terms of% of personal maximum FEV1 between lung transplantation and randomization.
Figure 2. Trajectories of forced expiratory volume in 1 second (FEV1) for individual subjects, from transplantation to end of follow-up. FEV1 trajectories are plotted in terms of% of personal maximum FEV1 between lung transplantation and randomization. 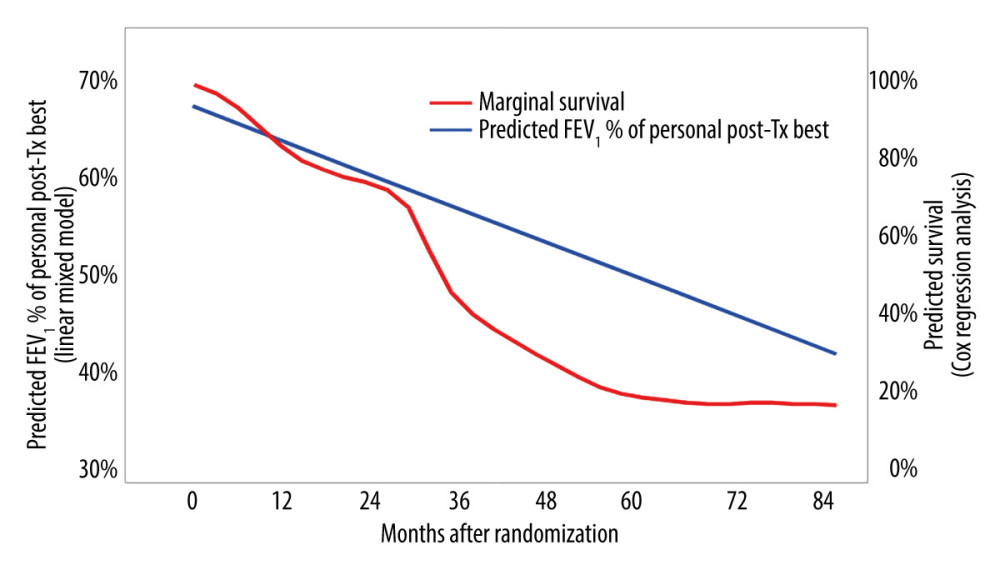 Figure 3. Association between FEV1% of personal post-transplant maximum and mortality risk – joint model analysis.
Figure 3. Association between FEV1% of personal post-transplant maximum and mortality risk – joint model analysis. 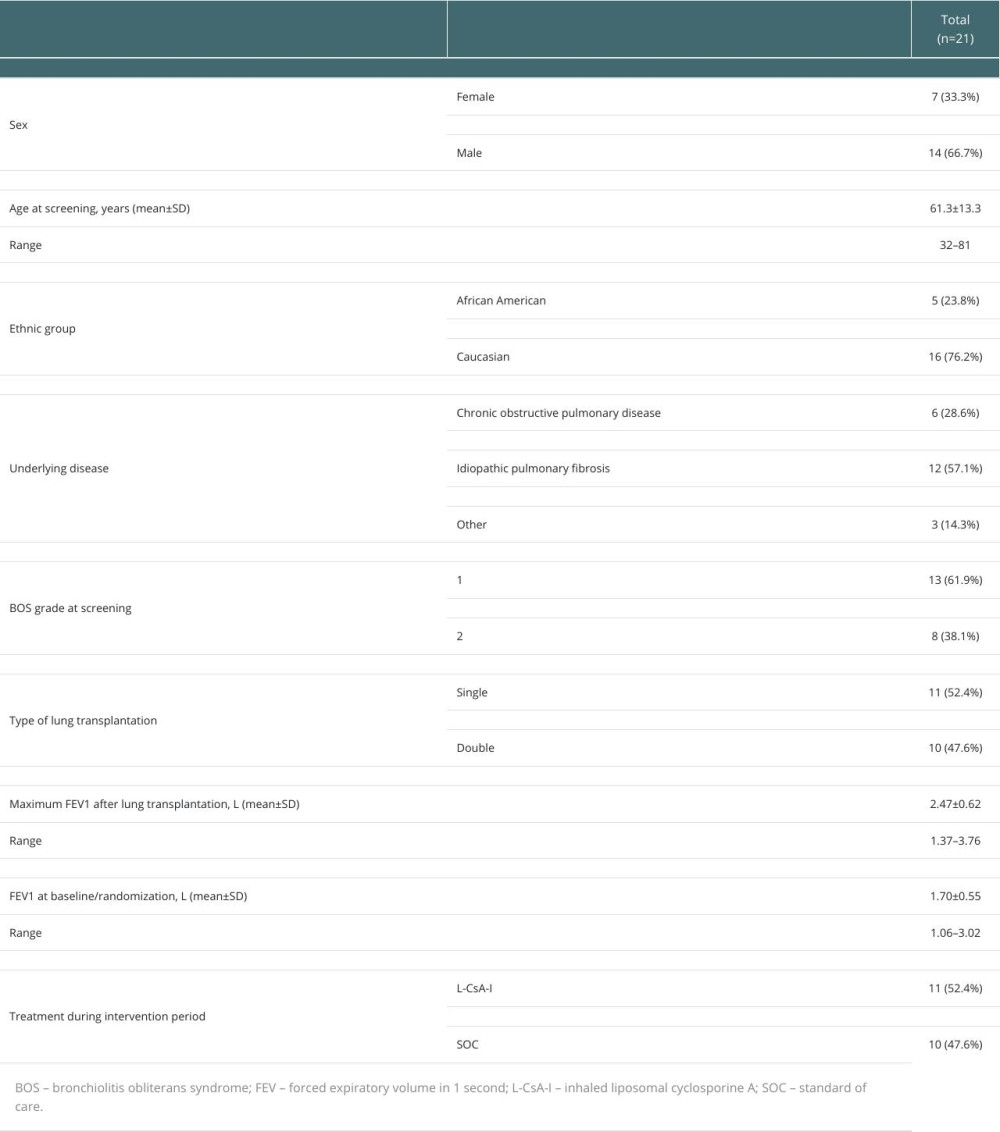
References
1. Kulkarni HS, Cherikh WS, Chambers DC, Bronchiolitis obliterans syndrome-free survival after lung transplantation: An International Society for Heart and Lung Transplantation Thoracic Transplant Registry analysis: J Heart Lung Transplant, 2019; 38; 5-16
2. Kneidinger N, Milger K, Janitza S, Lung volumes predict survival in patients with chronic lung allograft dysfunction: Eur Respir J, 2017; 49(4); 1601315
3. Krishna R, Anjum F, Oliver TI, Bronchiolitis obliterans. [Updated 2023 Aug 14]: StatPearls [Internet], 2024, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK441865
4. Meyer K, Raghu G, Verleden G, An international ISHLT/ATS/ERS clinical practice guideline: Diagnosis and management of bronchiolitis obliterans syndrome: Eur Respir J, 2014; 44; 1479-503
5. Duncan SR, Leonard C, Theodore J, Oligoclonal CD4+ T cell expansions in lung transplant recipients with obliterative bronchiolitis: Am J Respir Crit Care Med, 2002; 165; 1439-44
6. Burton C, Carlsen J, Mortensen J, Long-term survival after lung transplantation depends on development and severity of bronchiolitis obliterans syndrome: J Heart Lung Transplant, 2007; 26(7); 681-86
7. Copeland C, Snyder , Zaas D, Survival after bronchiolitis obliterans syndrome among bilateral lung transplant recipients: Am J Respir Crit Care Med, 2010; 182; 784-89
8. Kemp R, Pustulka I, Boerner G: Respir Med, 2021; 188; 106608
9. Iacono A, Wijesinha M, Rajagopal K, A randomised single-centre trial of inhaled liposomal cyclosporine for bronchiolitis obliterans syndrome post-lung transplantation: ERJ Open Res, 2019; 5; 00167-2019
10. Estenne M, Maurer JR, Boehler A, Bronchiolitis obliterans syndrome 2001: An update of the diagnostic criteria: J Heart Lung Transplant, 2002; 21; 297-310
11. Brusasco V, Crapo R, Viegi GATS/ERS task force, Standardization of lung function testing: Eur Respir J, 2005; 26; 153-61
12. American Thoracic Society, Standardization of spirometry, 1994 update: Am J Respir Crit Care Med, 1995; 152; 1107-36
13. Ibrahim JG, Chu H, Chen LM, Basic concepts and methods for joint models of longitudinal and survival data: J Clin Oncol, 2010; 28(16); 2796-801
14. Rizopoulos D, JM: An R package for the joint modelling of longitudinal and time-to-event data: Journal of Statistical Software, 2010; 35(9); 1-33
15. Todd JL, Neely ML, Finlen Copeland CA, Prognostic significance of early pulmonary function changes after onset of chronic lung allograft dysfunction: J Heart Lung Transplant, 2019; 38; 184-93
16. Kneidinger N, Ghiani A, Milger K, Impact of lung function decline on mortality in lung transplant recipients: Long-term results from the L-CsA-i study for the prevention of bronchiolitis obliterans syndrome: Front Med (Lausanne), 2022; 9; 897581
17. Verleden AR, Glanville ED, Chronic lung allograft dysfunction: Definition, diagnostic criteria, and approaches to treatment – A consensus report from the Pulmonary Council of the ISHLT, J: Heart Lung Transplant, 2019; 38(5); 493-503
18. Lama VN, Murray S, Lonigro RJ, Course of FEV1 after onset of bronchiolitis obliterans syndrome in lung transplant recipients: Am J Respir Crit Care Med, 2007; 175; 1192-98
19. Burton CM, Iversen M, Mortensen J: J Heart Lung Transplant, 2007; 26(11); 1127-34
20. Iacono AT, Corcoran TE, Griffith BP, Aerosol cyclosporine therapy in lung transplant recipients with bronchiolitis obliterans: Eur Respir J, 2004; 23(3); 384-90
21. Iacono AT, Johnson BA, Grgurich WF, A randomized trial of inhaled cyclosporine in lung-transplant recipients: N Engl J Med, 2006; 354(2); 141-50
Figures
Figure 1. Flow diagram depicting study design.Figure 2. Trajectories of forced expiratory volume in 1 second (FEV1) for individual subjects, from transplantation to end of follow-up. FEV1 trajectories are plotted in terms of% of personal maximum FEV1 between lung transplantation and randomization.Figure 3. Association between FEV1% of personal post-transplant maximum and mortality risk – joint model analysis. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988