21 June 2024: Original Paper
Long-Term Graft and Patient Survival After Re-Transplantation
Dana BielopolskiDOI: 10.12659/AOT.943903
Ann Transplant 2024; 29:e943903






Abstract
BACKGROUND: Kidney transplant recipients have higher life expectancy but may require subsequent transplantations, raising ethical concerns regarding organ allocation. We assessed the safety of multiple kidney transplants through long-term follow-up.
MATERIAL AND METHODS: A retrospective cohort study was conducted at a single center, categorizing patients based on the number of kidney transplantations received. The primary outcome was the composite of death-censored graft failure and overall mortality. The secondary outcome was death-censored graft failure.
RESULTS: Between 2000 and 2019, our center performed 2152 kidney transplantations. Patients were divided into 3 groups: A (1 transplant; n=1850), B (2 transplants; n=285), and C (3 or more transplants; n=75). Group C patients were younger, had fewer comorbidities, and received more aggressive induction therapy. The primary outcomes, including death-censored graft loss and overall mortality, showed similar rates across groups (A: 21.3%, B: 25.2%, C: 21.7%, p=0.068). However, the secondary outcome of death-censored graft failure alone was significantly lower in group A compared to the other groups. No significant difference was observed between groups B and C (8% vs 16% and 13%, respectively, p=0.001, p=0.845). Multivariate analysis identified having a living donor as the strongest predictor of patient and graft survival in all study groups.
CONCLUSIONS: Graft and patient survival rates were similar between first and multiple transplant recipients. Multiple transplant recipients had lower death-censored graft failure risk compared to first transplant recipients. However, the risk did not differ among second and subsequent transplant recipients. Younger patients, especially those with a living donor, should be considered for repeat kidney transplantation.
Keywords: Kidney Transplantation, Multiple Transplantations, Immunosuppression, Living Donor, Kidney Graft, Humans, Female, Male, Middle Aged, Retrospective Studies, Graft Survival, adult, Reoperation, Graft Rejection, Aged, Survival Rate
Introduction
Over the last few decades, kidney transplantation has shown steady improvements in success rates and patient survival. However, it is not uncommon for kidney transplant recipients to outlive their transplanted organs [1–3]. Many eligible candidates for kidney transplantation fall within the age range of 45–65 years and may require either dialysis or re-transplantation in the future [4,5]. According to the Eurotransplant kidney allocation system, the percentage of transplanted patients who return to dialysis due to a failing graft may be as high as 20% [6]. While repeat kidney transplantation has a lower graft survival rate than the first transplant, it remains a better treatment option for young candidates compared to lifelong dialysis [7,8]. Re-transplantation candidates constitute a significant proportion of the kidney transplant waiting list, with a consistent percentage of 15% [7,9]. Re-transplantation can, however, result in multiple complications, including high-dose immunosuppressive treatment for highly sensitized recipients and older recipients with multiple comorbidities after long-term chronic kidney disease (CKD) and immunosuppression therapy. Furthermore, due to the organ shortage, older recipients with failing grafts often receive grafts from extended-criteria donors [10,11]. Although earlier re-transplantation is usually considered the best option following graft failure, data on the efficacy of re-transplantation are lacking, as these patients are not included in the Renal Registry annual report. Therefore, we aimed to assess the long-term results of multiple kidney transplantations.
Material and Methods
STATISTICAL ANALYSIS:
Statistical analyses were performed using SPSS (version 25). Nominal variables are expressed as numbers (%). Comparison of proportions between groups was performed using the chi-squared test. Continuous variables are expressed as mean±SD where a
Multivariate logistic regression models for graft loss and death used the predictor variables as fixed effects. These included: age, sex, time on dialysis, ischemic heart disease, diabetes, PRA, living donor, donor age, delayed graft function (DGF), and hospitalizations. All effect estimates are presented as hazard ratios (HRs), along with the corresponding 95% confidence intervals (CI).
Results
OUTCOMES ACCORDING TO NUMBER OF TRANSPLANTS:
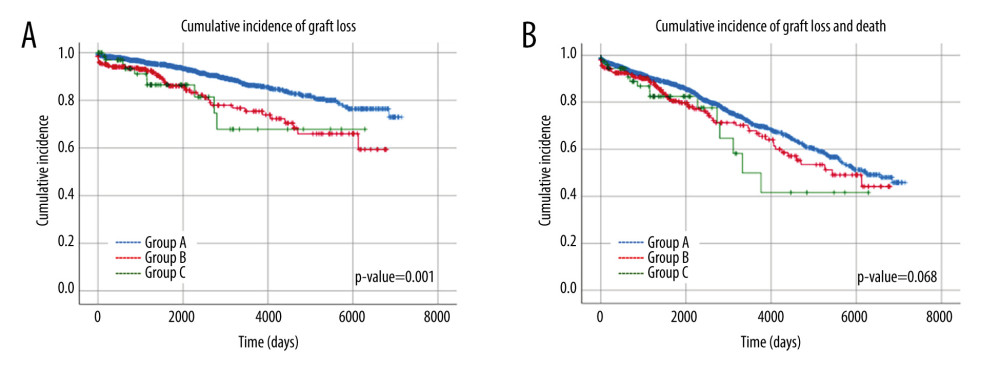
During the follow-up period, 465 cases of the composite outcome of death-censored graft failure and overall mortality were recorded. Among group A, there were 384 cases (21%), in group B there were 65 cases (25%), and there were 16 cases (22%) in group C. There was no significant difference between the risk of the composite outcome of death-censored graft failure and overall mortality between patients in groups A, B, and C (A vs B P=0.08, B vs C P=0.546, A vs C P=0.092) according to Kaplan-Meier analysis (Figure 1).
During the follow-up period, there were 211 cases of the secondary outcome of death-censored graft failure alone: 158 cases (8%) in group A, 43 cases (16%) in group B, and 10 cases (13%) in group C.
There was a significant difference between the risk of death-censored graft failure between group A vs groups B and C (
REGRESSION MODEL:
Based on the adjusted model, the composite outcome of death and graft loss was significantly associated with several factors, including IHD (HR=1.496, 95%CI 1.194–1.874), DM (HR=1.271, 95% CI 1.022–1.581), a living donor (HR=0.467, 95% CI 0.370–0.588), DGF (HR=1.483, 95% CI 1.177–1.867), and hospitalization after transplantation (HR=1.006, 95% CI1.002–1.009) (Table 3). Death-censored graft loss alone was increased in the presence of IHD (HR=1.574, 95% CI 1.086–2.281), an elderly donor (HR=1.018, 95% CI 1.008–1.028), and DGF (HR=1.812, 95% CI 1.296–2.535) and reduced with a living donor (HR=0.403, 95% CI 0.285–0.570). Furthermore, a living donor significantly reduced the risk of either graft loss alone or in combination with death (0.285–0.570 and 0.370–0.588, respectively) (Table 3).
Discussion
As the lifespan of kidney transplant patients increases, graft survival becomes a significant factor in their longevity and quality of life. However, repeated transplantation presents ethical challenges concerning organ allocation. In this study, we described a large kidney-transplanted patient cohort and compared their long-term outcomes according to transplantation numbers. Patients who received multiple transplants were younger with lower prevalence of DM, had fewer cardiovascular risk factors, and required an aggressive induction therapy due to increased allo-immunologic risk. The rates of the composite outcome of death-censored graft failure and overall mortality were similar across all groups. The rate of death-censored graft loss alone was lower in those with first transplantation compared to multiple transplantations, but the risk of death-censored graft failure alone was comparable between patients in groups B and C. The strongest predictor of patient and graft survival was having a living donor.
Despite its high risk, repeat transplantation is still preferable for young recipients with long life expectancy. Across patient groups, graft failure and overall mortality were similar, but the incidence death-censored graft failure was higher among repeated transplant recipients. These findings indicate that older patients receiving a first graft are more likely die from non-transplant-related causes, resulting in similar rates of graft loss and mortality [13]. Notably, the death-censored graft loss was not different between second and multiple transplantation recipients, suggesting that the risk does not increase with multiple transplantations. Since the strongest predictor of graft survival was having a living donor, our findings support allocating living donors to young recipients with fewer comorbidities who need re-transplantation.
Despite advancements in treatment protocols, such as the utilization of calcineurin inhibitors, human leukocyte antigens (HLA) matching, and antibody screening, HLA mismatch and episodes of acute rejection still have a negative impact on graft survival. Sensitization is expected to increase in recipients who have undergone multiple transplants [14], as seen in our cohort, where younger patients had increased allo-immunologic risk with repeated transplantations. Due to higher PRA levels, they required an aggressive induction with rATG compared with first-transplant recipients. When selecting the best donor option for a pediatric patient, we should carefully consider shortening dialysis time with deceased donors [8,15], as opposed to longer graft survival in patients who received a transplant from a living donor [16]. Dialysis time may be increased in the presence of multiple transplants. Regardless of preemptive transplantation cases, most patients with a failing graft will return to dialysis while waiting for a suitable donor. Young adults who received a first graft as children from a living donor are likely to be more sensitized, experience prolonged exposure to dialysis between transplants, and a reduced probability of having a living donor for a second transplant. Therefore, pediatric re-transplant candidates may benefit from living donation rather than deceased donation [16]. Children and young adults should be provided with well-matched, high-quality kidney allografts, as they may require multiple transplants throughout their lives [17].
Transplant centers allocate preferentially well-matched kidney to pediatric candidates, assuming a longer life expectancy, but even with the best kidney, young candidates will probably need a second transplant during their lifetimes. Despite the favorable HLA matches and careful graft selection for pediatric recipients, they still have a high cumulative 10-year incidence of graft loss (74.4%), perhaps due to nonadherence to treatment protocols [18,19].
Intriguingly, the impact of HLA matching on the prevalence of graft losses is more pronounced in first-transplant recipients than in those who receive re-transplants, but it is confounded by age. Generally, younger patients have a better HLA match than older ones. To shorten the waiting list and cold ischemia time, the Eurotransplant Senior Program allocates donors over age 65 to recipients who are also over 65, without considering HLA matching [20,21]. Previous studies have identified a subset of patients who underwent their first kidney transplantation at a young age, experienced graft loss, and subsequently received a transplant from expanded-criteria donors at a median age of 43 years [6,13,22]. Our results suggest that this approach puts them at a disadvantage, as their graft survival will improve when received from a living donor. Some studies have reported similar graft survival rates in third or subsequent deceased donor recipients compared to first-time recipients [23,24], but patients who undergo multiple transplants typically require longer dialysis time, and a higher degree of HLA sensitization is expected. This poor profile translates into higher rates of infections, rejection, and death as a result of multiple comorbidities [25,26]. A cohort of re-transplanted patients with similar characteristics to those in the present study described reduced death-censored graft survival with repeated transplantations but only for deceased donor transplants [27]. This complements our result emphasizing the importance of a living donor in repeated transplantations to improve graft survival. A large retrospective analysis from the EU registry has concluded that receiving more than 3 kidney transplantations is associated with increased mortality and graft loss compared to the first transplantation [6]. We believe this is due to an unfavorable patient profile in the re-transplantation group, characterized by a higher prevalence of comorbidities, prolonged immunosuppression, and dialysis adverse effects [6].
Diabetes is a well-documented risk factor for kidney failure, and new-onset diabetes mellitus after transplant (NODAT) occurs in approximately 30% of non-diabetic kidney transplant recipients many years after transplantation. Diabetes in patients with kidney transplantation constitutes a major comorbidity, and has a significant impact on the patient s and allograft outcomes [28]. It is interesting to note that in our cohort diabetes contributed to overall mortality but not to graft loss. This may be due to the relatively short follow-up time on one hand and the worsening of atherosclerosis on the other.
This study has certain limitations. First, it is based on data from a single center, which limits the generalizability of the findings. However, RMC is the primary transplantation center in Israel, conducting the majority of kidney transplants for both adult and pediatric patients. Therefore, the number of cases analyzed is comparable to previous multi-center studies. Second, being retrospective in nature, the study may have varying group sizes, and the patients with multiple transplants may have been distributed over an extended period. To counteract this, we included a maximum number of patients in each group to represent various treatment protocols and surgical techniques. In our examination of graft survival, adjusted for death censoring, based on donor type and transplantation count, we observed no discernible distinctions among cohorts A, B, and C (Supplementary Figure 1). This outcome may stem from the interplay of various factors influencing graft longevity in addition to donor type or the limited sample size in group C.
Our analysis also exhibits certain noteworthy strengths. The centralized healthcare system in Israel provides us with comprehensive data on donor and recipient characteristics and transplant outcomes.
Conclusions
Our study shows that patients who received multiple transplants have similar patient and graft survival as those who had received a second transplant, regardless of the number of transplantations. We believe that young re-transplant recipients should not be deprived of access to organs based on their age, and that decisions should be based on individual circumstances. Enabling live donation to young people needing re-transplantation is crucial to increase their life span and improve their quality of life by extending graft survival. Children and young adults have lower comorbidity rates and fewer therapeutic adverse effects [6], making them ideal candidates for re-transplantation.
Tables
Table 1. Demographic and clinical characteristics of patients.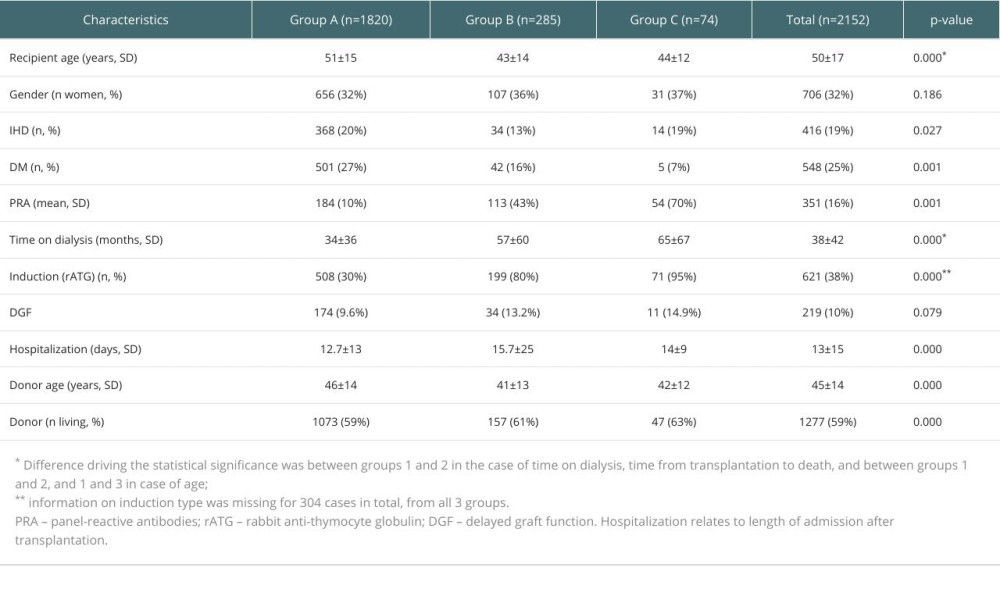 Table 2. Prevalence of primary kidney disease according to transplantation number.
Table 2. Prevalence of primary kidney disease according to transplantation number.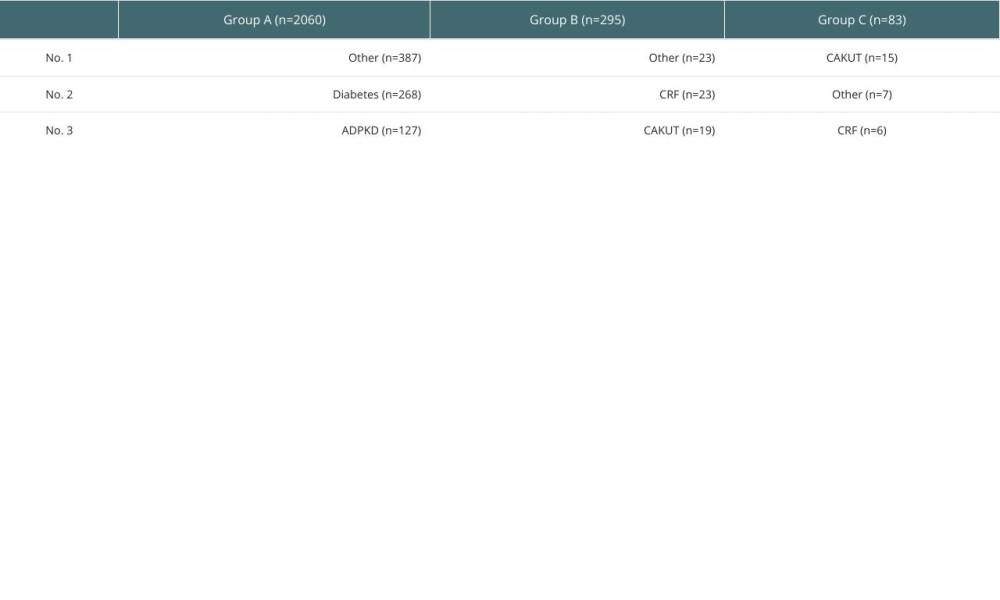 Table 3. Multiple regression for graft loss vs graft loss and death. Parameters include age, diabetes (DM), ischemic heart disease (IHD), panel-reactive antibody (PRA), living donor, donor age, delayed graft function (DGF), and hospitalization (HOSP).
Table 3. Multiple regression for graft loss vs graft loss and death. Parameters include age, diabetes (DM), ischemic heart disease (IHD), panel-reactive antibody (PRA), living donor, donor age, delayed graft function (DGF), and hospitalization (HOSP).
References
1. Hariharan S, Johnson CP, Bresnahan BA, Improved graft survival after renal transplantation in the United States, 1988 to 1996: N Engl J Med, 2000; 342; 605-12
2. Seron D, Moreso F, Arias M, Campistol JM, Estimation of renal allograft half-life: fact or fiction?: Nephrol Dial Transplant, 2011; 26; 3013-18
3. Meier-Kriesche H-U, Schold JD, Kaplan B, Long-term renal allograft survival: Have we made significant progress or is it time to rethink our analytic and therapeutic strategies?: Am J Transplant, 2004; 4; 1289-95
4. Matas AJ, Smith JM, Skeans MA, OPTN/SRTR 2013 Annual data report: Kidney: Am J Transplant, 2015; 15(Suppl 2); 1-34
5. : Annual Report 2014 - Eurotransplant [Internet] [cited 2022 Aug 18]; Available from: https://www.eurotransplant.org/annual-report/annual-report-2014/
6. Assfalg V, Selig K, Tolksdorf J, Repeated kidney re-transplantation-the Eurotransplant experience: A retrospective multicenter outcome analysis: Transpl Int, 2020; 33; 617-31
7. Magee JC, Barr ML, Basadonna GP, Repeat organ transplantation in the United States, 1996–2005: Am J Transplant, 2007; 7; 1424-33
8. Rao PS, Schaubel DE, Wei G, Fenton SSA, Evaluating the survival benefit of kidney retransplantation: Transplantation, 2006; 82; 669-74
9. Sharples E, Casula A, Byrne C, UK Renal Registry 19th Annual Report: Chapter 3 Demographic and biochemistry profile of kidney transplant recipients in the UK in 2015: National and centre-specific analyses: Nephron, 2017; 137(Suppl 1); 73-102
10. Gjertson DW, A multi-factor analysis of kidney regraft outcomes: Clin Transpl, 2002; 335-49
11. Assfalg V, Hüser N, Repeated kidney re-transplantation in times of organ shortage – a critical review: Curr Opin Organ Transplant, 2021; 26; 106-11
12. Arnol M, Naumovic R, Dimitrov EP, Immunosuppressive regimens following kidney transplantation in five European countries: The observational RECORD study: Transplantation Reports, 2020; 5; 100061
13. Redfield RR, Gupta M, Rodriguez E, Graft and patient survival outcomes of a third kidney transplant: Transplantation, 2015; 99; 416-2
14. Coupel S, Giral-Classe M, Karam G, Ten-year survival of second kidney transplants: Impact of immunologic factors and renal function at 12 months: Kidney Int, 2003; 64; 674-80
15. Ojo A, Wolfe RA, Agodoa LY, Prognosis after primary renal transplant failure and the beneficial effects of repeat transplantation: Multivariate analyses from the United States Renal Data System: Transplantation, 1998; 66; 1651-59
16. Phonphok K, Homkrailas P, Duong T, Time to second kidney transplantation in young adults after failed pediatric kidney transplant: Pediatr Transplant, 2020; 24; e13800
17. Ploos van Amstel S, Vogelzang JL, Long-term risk of cancer in survivors of pediatric ESRD: Clin J Am Soc Nephrol, 2015; 10; 2198-204
18. Van Arendonk KJ, James NT, Boyarsky BJ, Age at graft loss after pediatric kidney transplantation: exploring the high-risk age window: Clin J Am Soc Nephrol, 2013; 8; 1019-26
19. Dunn TB, Browne BJ, Gillingham KJ, Selective retransplant after graft loss to nonadherence: Success with a second chance: Am J Transplant, 2009; 9; 1337-46
20. Halleck F, Khadzhynov D, Liefeldt L, Immunologic outcome in elderly kidney transplant recipients: Is it time for HLA-DR matching?: Nephrol Dial Transplant, 2016; 31; 2143-49
21. Heidt S, Haasnoot GW, Witvliet MD, Allocation to highly sensitized patients based on acceptable mismatches results in low rejection rates comparable to nonsensitized patients: Am J Transplant, 2019; 19; 2926-33
22. Khalil AK, Slaven JE, Mujtaba MA, Re-transplants compared to primary kidney transplants recipients: A mate kidney paired analysis of the OPTN/UNOS database: Clin Transplant, 2016; 30; 566-78
23. Loupy A, Anglicheau D, Suberbielle C, Long-term outcome of third kidney transplants: Nephrol Dial Transplant, 2007; 22; 2693-700
24. Horovitz D, Caumartin Y, Warren J, Outcome of third renal allograft retransplants versus primary transplants from paired donors: Transplantation, 2009; 87; 1214-20
25. Schwarz A, Schäfer F, Framke T, Risk factors influencing the outcomes of kidney re-transplantation: Ann Transplant, 2021; 26; e928922
26. Matas AJ, Gillingham KJ, Payne WD, A third kidney transplant: Cost-effective treatment for end-stage renal disease?: Clin Transplant, 1996; 10; 516-20
27. Bellini MI, Courtney AE, McCaughan JA, Living donor kidney transplantation improves graft and recipient survival in patients with multiple kidney transplants: J Clin Med, 2020; 9(7); 2118
28. Peev V, Reiser J, Alachkar N, Diabetes mellitus in the transplanted kidney: Front Endocrinol (Lausanne), 2014; 5; 141
Tables
Table 1. Demographic and clinical characteristics of patients.Table 2. Prevalence of primary kidney disease according to transplantation number.Table 3. Multiple regression for graft loss vs graft loss and death. Parameters include age, diabetes (DM), ischemic heart disease (IHD), panel-reactive antibody (PRA), living donor, donor age, delayed graft function (DGF), and hospitalization (HOSP).Table 1. Demographic and clinical characteristics of patients.Table 2. Prevalence of primary kidney disease according to transplantation number.Table 3. Multiple regression for graft loss vs graft loss and death. Parameters include age, diabetes (DM), ischemic heart disease (IHD), panel-reactive antibody (PRA), living donor, donor age, delayed graft function (DGF), and hospitalization (HOSP). In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988