26 November 2024: Original Paper
Factors Influencing Stress Disorders in Intensive Care Unit (ICU) Patients After Liver Transplantation: A Cross-Sectional Study
Xiao-Qing Sun1ABCDEF, Ying Xu1ABCDEF, Xiu-Lian Wu1ABCDEF, Jing-Jing Zhi1ABCDEF, Yan-Mei Gu1ABCDEF*
DOI: 10.12659/AOT.944320
Ann Transplant 2024; 29:e944320






Abstract
BACKGROUND: Evidence on psychological factors associated with post-transplant post-traumatic stress disorder (PTSD) in liver transplantation (LT) patients is limited. Identifying the psychological factors associated with post-transplant PTSD would help to understand the symptoms of PTSD and take preventive measures. The aim of this study was to investigate factors influencing stress disorders in Intensive Care Unit (ICU) patients 1 year after LT.
MATERIAL AND METHODS: We assessed data from 184 LT patients at our hospital between January 2020 and December 2022. According to the PCL-C score, the patients were divided into the PTSD group (score ≤37) and the non-PTSD group (score >37). The demographic data, clinical data, the pain visual analogue scale (VAS), the anxiety and depression scale (HADS), and the psychological resilience scale (CD-RISC score) were compared between the 2 groups. Pearson correlation analysis was used to analyze the correlation between PCL-C and VAS, HADS, and CD-RISC, and logistic regression was used to analyze the factors influencing PTSD. SPSS 23.0 software was used for statistical analysis.
RESULTS: The average age of the 184 participants was 53.17 years (±3.47) and 66.85% of the subjects were male. The prevalence rate of post-transplant PTSD was 22.83% and the total score on the PCL-C scale was 32.47±7.81. Pearson correlation analysis showed that PCL-C score was positively correlated with VAS (r=0.312, P=0.012) and HADS (r=0.412, P<0.001), and negatively correlated with CD-RISC (r=-0.468, P<0.001). Logistic regression analysis showed that the symptom of post-transplant PTSD was significantly associated with higher VAS (OR=1.058, P=0.007) and HADS (OR=1.885, P<0.001) scores and lower CD-RISC (OR=2.213, P<0.001) score, which indicated that higher VAS and HAD scores were risk factors that contributed to PTSD and lower CD-RISC was a protective factor against PTSD.
CONCLUSIONS: We found that pain, anxiety, depression, and resilience were associated with symptoms of PTSD in LT patients in the ICU. Nursing staff should seek to relieve their patients’ pain and assure provision of targeted health education and personalized psychological counseling to reduce the risk of PTSD after LT.
Keywords: Liver Transplantation, Risk Factors, Perioperative Nursing, Humans, Male, Female, Stress Disorders, Post-Traumatic, Middle Aged, Cross-Sectional Studies, Intensive Care Units, adult, Postoperative Complications, Anxiety
Introduction
Liver transplantation (LT) is currently a common treatment for various end-stage liver diseases. Under the combined action of advanced transplantation technology, good organ preservation technology, and high-quality immunosuppressive agents, the survival rate, quality of life, and survival time of liver transplantation recipients have improved [1]. However, LT patients commonly experience emotional changes before and after surgery, causing physical and mental stress. For example, preoperative mood changes may produce emotional changes such as avoidance of liver transplantation and worries about postoperative life. In the postoperative period, LT patients need to be observed in the ICU, and the uncertain observation time can cause anxiety in patients. Subsequently, long-term use of immunosuppressive drugs can induce anxiety, depression, and other emotions not conducive to the recovery of patients’ physical health. The correct assessment of the impact of LT on the patient’s mental well-being is very important for optimizing treatment.
Post-traumatic stress disorder (PTSD) has received much attention in recent years. PTSD can be accompanied by pain, somatization, and mental and social dysfunction, with reported prevalence rates of 1% to 45% among post-transplant LT patients [2]. PTSD is caused by catastrophic, threatening, and sudden life events that can cause mental disorders that manifest much later [3]. The main characteristics are repeated re-perception of intrusive traumatic situations, avoidance responses, negative mood, and continuous high alertness. PTSD is not a single event, but a series of dynamic processes that can lead to traumatic experiences. However, transplantation is considered a “predetermined trauma,” in which PTSD can be caused by complications after transplantation, long Intensive Care Unit (ICU) stay time, the use of immunosuppressive agents, postoperative pain, and a series of extreme physical and mental factors [4].
Demographic and clinical factors are reported to be significantly associated with more severe post-transplant PTSD symptoms [2]. The type of primary liver disease [5–8] and severity of disease [9] have been reported to be pre-transplant risk factors, as well as duration of intensive care treatment [10], use of corticosteroids [11], and severe drug adverse effects [12]. Rothenhäusler et al reported that presence of depressive symptoms in LT recipients after transplantation was associated with greater risk of post-transplant PTSD [10]. Other studies reported that psychiatric symptoms in critically ill patients who underwent organ transplantation were effective predictors of PTSD [13,14]. LT recipients often reported positive psychological outcomes of optimism attitude, self-improvement, and tenacity, and they showed great resilience in overcoming various stresses after transplantation, but the relationship between resilience and PTSD is unclear [15–18].
To improve the overall efficacy of nursing, it is necessary to have a sufficient understanding of the patient’s post-transplant PTSD, to identify the factors influencing post-transplant PTSD, and to provide specific nursing measures. However, evidence about the psychological factors associated with post-transplant PTSD in LT patients is limited and not well explained. To further identify the psychological factors associated with post-transplant PTSD would help to understand the symptoms of PTSD and take preventive measures. We performed a questionnaire-based comprehensive psychosocial survey focusing on psychological themes of PTSD, pain, depression, anxiety, and resilience [19–22] to determine psychosocial factors associated with post-transplant PTSD. Therefore, clinical and socio-demographic data and 4 questionnaires were used to further understand the prevalence and symptoms of post-transplant PTSD in LT recipients and investigated their associated factors.
Material and Methods
CLINICAL MATERIAL:
A cross-sectional investigation was carried out using questionnaires. The chosen sampling method was purposive sampling. The medical records of 184 patients who underwent LT in the ICU of Capital Medical University Youan Hospital from January 2020 to December 2022 and were followed up after LT were collected. Inclusion criteria were: 1) first liver transplantation; 2) age ≥18 years old; 3) at least primary school education, able to communicate and normal intelligence and understanding, and could complete the questionnaires independently. Exclusion criteria were: 1) patients with severe stress events during treatment; 2) patients with immune system diseases (eg, systemic lupus erythematosus, rheumatoid arthritis, Sjogren’s syndrome, ulcerative colitis); 3) patients with mental and cognitive abnormalities; 4) patients with communication disorders; 5) patients with missing clinical data. Clinical data collection used a baseline data form including items such as gender, age, primary disease, education level, marital status, per capita monthly income, pain level, anxiety and depression, and resilience.
ASSESSMENT TOOLS:
PCL-C: The components of the scale are mainly PTSD-related diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders (USA), which are mainly used to assess the post-traumatic experience of the general population (relative to military personnel) in daily life (relative to war). The research subjects need to be scored based on the degree of the problem in the past month. The scale consisted of 17 small items, each item using 5-point Likert 5 scale, from “extremely severe” to “no” were given 5, 4, 3, 2, and 1 points, the total score was 17~85 points, the final score was proportional to the severity of PTSD symptoms. PCL-C has 3 main dimensions: avoidance response (7 items), continuous high alertness (5 items), and re-perception of intrusive traumatic situations (5 items). To improve the diagnostic sensitivity, many Chinese scholars believe that 38 points should be regarded as the demarcation standard [23]. In this study, 38 points was also regarded as the positive screening threshold. If the total score was less than 37 points, there was no significant symptom and no PTSD. If the total score was 38 to 85 points, it indicates that there are symptoms and PTSD is present. The Cronbach’s α coefficient of the Chinese version of PCL-C was 0.838 in this study.
The degree of pain was evaluated by VAS. The VAS represented the degree of pain from 0 points to 10 points (0 points without pain, 10 points with unbearable pain). Patients chose one of these 11 numbers to present their own level of pain. The higher the score, the worse the pain. Anxiety and depression were assessed using the HADS, in which a total of 14 items are equally divided into 2 subscales: anxiety (HADS-A) and depression (HADS-D). The subjects need to be scored based on how they currently feel and are rated on a 4-point Likert scale that ranged from 0 to 3. In this study, the ratings of 14 items are summarized to obtain a total score (0 to 42), the higher the score, the more serious the anxiety and depression. The Cronbach’s alpha was 0.76 for the HADS-A and 0.82 for the HADS-D.
Resilience was assessed by CD-RISC, including 3 dimensions: tenacity, self-improvement, and optimism. The scale includes 25 items: 0=“not at all”, 1=“rarely”, 2=“sometimes”, 3=“often”, and 4=“always”. The total score of CD-RISC is the sum of the scores of these 25 items, and the total score is positively correlated with resilience. The Cronbach’s alpha coefficient of the Chinese version of CD-RISC [23] was 0.92 in this study.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE:
This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of Beijing Youan Hospital (ethical batch number: LL-2023-052-K), and informed consent was obtained from all participants. All methods were carried out in accordance with relevant guidelines and regulations.
One year after LT, the research team used unified instructions to introduce the significance, purpose, questionnaire filling methods, and precautions of this study to the patients in detail. The questionnaires were, distributed, filled out by the patients, and recovered upon completion. Excel was used to establish a database, and the double entry method was used to import data into the database. A total of 184 questionnaires were distributed in this study, 184 were recovered, there were 184 valid questionnaires, and the effective recovery rate was 100.00%.
According to the PCL-C score, the patients were divided into PTSD group (score ≤37) and non-PTSD group (score >37). The demographic data, clinical data, VAS, HADS, and CD-RISC were compared between the 2 groups.
STATISTICAL METHODS:
SPSS23.0 software was used, and the measurement data were tested for normality. The normal distribution data were described by mean plus or minus standard deviation, and the independent sample
Results
GENERAL CHARACTERISTICS:
A total of 184 patients were followed up in this study, aged 36–69 (53.17±3.47) years, and the ratio of males to females (123/61) was 2.01: 1. There were 131 cases of hepatitis B virus infection and 53 cases of ischemic biliary disease. The total score of PCL-C scale was 32.47±7.81 (15~61). Among them, 42 patients had no less than 38 points, and the positive rate of PTSD was 22.83%. Among them, sustained high alertness was 26.40±6.81 points, avoidance response was 13.37±4.72 points, and intrusive trauma situation was 6.78±2.48 points.
DEMOGRAPHIC CHARACTERISTICS AND CLINICAL DATA:
The clinical data from the PTSD group and non-PTSD group were no significantly different. The proportion of patients with no spouse in the occurrence group was higher than that in the non-occurrence group (42.85% vs 19.72%, χ2=9.256, P=0.002), and the monthly family income was lower than that in the non-occurrence group (4712.71±63.18 vs 5691.87±59.85, t=6.733, P=0.007). The VAS (6.12±1.75 vs 4.92±2.43, t=4.378, P=0.016) and HADS (16.87±3.66 vs 12.33±2.75, t=9.675, P<0.001) scores of the occurrence group were higher than those of the non-occurrence group, and the CD-RISC score was lower than that of the non-occurrence group (67.18±4.91 vs 77.21±4.22, t=8.971, P<0.001) (Table 1).
CORRELATION BETWEEN PCL-C AND VAS, HADS, CD-RISC:
Pearson correlation analysis showed that PCL-C score was positively correlated with VAS (r=0.312,
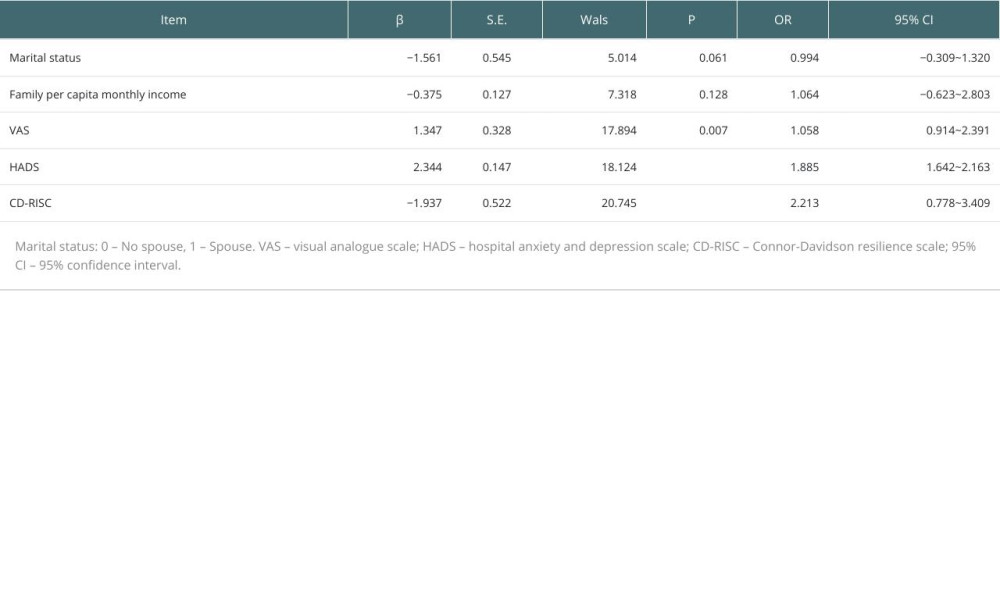
LOGISTICS REGRESSION ANALYSIS:
The logistic regression equation was fitted with the occurrence of PTSD as the dependent variable (0: no occurrence, 1: occurrence) and the statistically significant influencing factors (marital status, family monthly income per capita, VAS, HADS, CD-RISC) in the univariate analysis as independent variables. The results showed that higher VAS (OR=1.058, P=0.007) and HADS (OR=1.885, P<0.001) scores were risk factors for PTSD. Higher CD-RISC (OR=2.213, P<0.001) score was a protective factor for PTSD (Table 2).
Discussion
LT recipients are at increased risk of post-transplant PTSD. However, evidence about the factors associated with post-transplant PTSD in LT patients is limited and not well explained. Therefore, we conducted a detailed survey investigating influencing factors for post-transplant PTSD in recipients, which may help in prevention and treatment strategies for PTSD.
In this study, the incidence of post-transplant PTSD in ICU patients undergoing LT was 22.83%, which is consistent with the reported prevalence of 1–45% in a previous systematic review [2], indicating that PTSD is common in LT recipients. Baranyi et al found that liver transplantation patients have greater risk of post-transplantation PTSD (30.2%) compared to heart or lung transplantation patients (6.5% and 9.5%, respectively), indicating LT recipients may experience great mental pressure [24].
We also found that the prevalence of PTSD in LT recipients without a spouse was significantly higher than in those with a spouse (42.85% vs 19.72%,
After univariate analysis of PTSD in patients undergoing LT, logistic regression analysis was performed. After excluding confounding factors, the results showed that higher VAS (OR=1.058,
Anxiety and depression are the most frequently experienced negative emotions in organ transplant patients and are more common in LT patients [15–18]. Patients with anxiety and depression are prone to cognitive bias. In the face of external stimuli, they often respond with a pessimistic and evasive mentality, which can cause changes in the central nervous system. When negative emotions persist, PTSD-related symptoms increase [28,29]. One study found that higher anxiety at admission for hematopoietic stem cell transplantation and changes in anxiety during hospitalization were associated with worse PTSD symptoms at 6 months [30].
Logistic regression analysis in the present study found that a higher CD-RISC score (OR=2.213, P<0.001) was a protective factor for PTSD. Psychological resilience level is one of the factors causing PTSD in patients. Patients with higher levels of psychological flexibility were less likely to develop PTSD. Psychological flexibility has been shown to be related to personal emotions and experiences [31–33]. The patients with lower CD-RISC scores and lower level of resilience usually negatively respond to traumatic stressful events and most of them face the disease with a negative and avoidance attitude. The uncertainty of disease progression can aggravate the psychological burden. The repeated onset of the disease aggravates the harm to patients, and also greatly affects the enthusiasm and confidence of patients in treatment, resulting in the loss of hope for recovery and aggravation of psychological trauma. Therefore, improving psychological resilience may be another good strategy to prevent or treat post-transplant PTSD.
After experiencing serious traumatic events, patients need to be encouraged to have a positive attitude towards life and to achieve good mental health. A variety of psychological governance, nursing intervention, have been reported in the intervention of PSTD, using crisis intervention techniques and principles, focusing on providing support, and guiding patients to vent and express their emotions related to traumatic events. Therefore, in the early stage after liver transplantation, it is necessary to construct and adjust the physical and mental care plan and for transplant patients. Patients need to be guided to overcome personality defects and use disease rehabilitation channels. They require substantial social support to create a harmonious, pleasant, and loving rehabilitation environment with targeted and humanized care, enhancing treatment and life confidence, establishing correct social cognition, improving interpersonal relationships, and returning to society with a positive attitude.
There are some limitations in our study. Firstly, this was a cross-sectional study and no causal relationship between risk factors and PTSD symptoms can be established. Prospective studies are needed to validate the conclusions of this study in the future. Secondly, few clinical factors were investigated in this study. Studies have found that clinical charateristics such as in-ICU exposure to high doses of benzodiazepines and corticosteroid exposure [2,6,11] were significantly associated with PTSD. Based on these results, future studies of potential risk factors for PTSD in LT recipients should examine more clinical factors. Thirdly, there were many more males than females in this study, with ratio of males to females of 2.01: 1, and the patients were not assessed for long-term PTSD, which may have led to bias and limits the generalizability of our results.
Conclusions
Higher VAS and HADS scores and lower CD-RISC scores are the factors influencing PTSD after LT in ICU patients. Nursing staff should relieve patients’ pain and provide targeted health education and personalized psychological counseling to reduce the risk of PTSD after LT.

References
1. Zhang YY, Yuan ZR, Cai YN, Application of comfortable nursing in patients after liver transplantation: J Qilu Nurs, 2019; 25(24); 43-45
2. Davydow DS, Lease ED, Reyes JD, Post-traumatic stress disorder in organ transplant recipients: A systematic review: Gen Hosp Psychiatry, 2015; 37(5); 387-98
3. Compean E, Hamner M, Post-traumatic stress disorder with secondary psychotic features (PTSD-SP): Diagnostic and treatment challenges: Prog Neuropsychopharmacol Biol Psychiatry, 2019; 88; 265-75
4. Zhang YJ, Zhao RP, Ren JH, Acute stress disorder of malignancy inpatients informed with diagnosis: Mod Nurs, 2018; 24(20); 2434-36
5. Rogal SS, Dew MA, Fontes P, DiMartini AF, Early treatment of depressive symptoms and long-term survival after liver transplantation: Am J Transplant, 2013; 13(4); 928-35
6. Corruble E, Barry C, Varescon I, Depressive symptoms predict long-term mortality after liver transplantation: J Psychosom Res, 2011; 71(1); 32-37
7. Ruppert K, Kuo S, DiMartini A, Balan V, In a 12-year study, sustainability of quality of life benefits after liver transplantation varies with pretransplantation diagnosis: Gastroenterology, 2010; 139(5); 1619-1629e16294
8. Tombazzi CR, Waters B, Shokouh-Amiri MH, Neuropsychiatric complications after liver transplantation: Role of immunosuppression and hepatitis C: Dig Dis Sci, 2006; 51(6); 1079-81
9. Jin SG, Yan LN, Xiang B, Post-traumatic stress disorder after liver transplantation: Hepatobiliary Pancreat Dis Int, 2012; 11(1); 28-33
10. Rothenhäusler HB, Ehrentraut S, Kapfhammer HP, Psychiatric and psychosocial outcome of orthotopic liver transplantation: Psychother Psychosom, 2002; 71(5); 285-97
11. Zaydfudim V, Feurer ID, Landman MP, Reduction in corticosteroids is associated with better health-related quality of life after liver transplantation: J Am Coll Surg, 2012; 214(2); 164-73
12. Nickel R, Wunsch A, Egle UT, The relevance of anxiety, depression, and coping in patients after liver transplantation: Liver Transpl, 2002; 8(1); 63-71
13. Davydow DS, Gifford JM, Desai SV, Post-traumatic stress disorder in general intensive care unit survivors: A systematic review: Gen Hosp Psychiatry, 2008; 30(5); 421-34
14. Davydow DS, Zatzick D, Hough CL, Katon WJ, A longitudinal investigation of post-traumatic stress and depressive symptoms over the course of the year following medical-surgical intensive care unit admission: Gen Hosp Psychiatry, 2013; 35(3); 226-32
15. Rosenberger EM, Dew MA, Crone C, DiMartini AF, Psychiatric disorders as risk factors for adverse medical outcomes after solid organ transplantation: Curr Opin Organ Transplant, 2012; 17(2); 188-92
16. Jindal RM, Neff RT, Abbott KC, Association between depression and nonadherence in recipients of kidney transplants: Analysis of the United States renal data system: Transplant Proc, 2009; 41(9); 3662-66
17. Novak M, Molnar MZ, Szeifert L, Depressive symptoms and mortality in patients after kidney transplantation: A prospective prevalent cohort study: Psychosom Med, 2010; 72(6); 527-34
18. DiMartini A, Dew MA, Chaiffetz D, Early trajectories of depressive symptoms after liver transplantation for alcoholic liver disease predicts long-term survival: Am J Transplant, 2011; 11(6); 1287-95
19. Mureșanu IA, Grad DA, Mureșanu DF, Evaluation of post-traumatic stress disorder (PTSD) and related comorbidities in clinical studies: J Med Life, 2022; 15(4); 436-42
20. Beekman E, Verhagen A, Clinimetrics: Hospital anxiety and depression scale: J Physiother, 2018; 64(3); 198
21. Chiarotto A, Maxwell LJ, Ostelo RW, Measurement properties of Visual Analogue Scale, Numeric Rating Scale, and Pain Severity Subscale of the brief pain inventory in patients with low back pain: A systematic review: J Pain, 2019; 20(3); 245-63
22. Connor KM, Davidson JR, Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC): Depress Anxiety, 2003; 18(2); 76-82
23. Yu X, Zhang J, Yu XN, Factor analysis and psychometric evaluation of the Connor-Davidson resilience scale (CD-RISC) with Chinese people: Soc Behav Pers, 2007; 35(1); 19-30
24. Baranyi A, Krauseneck T, Rothenhäusler HB, Post-traumatic stress symptoms after solid-organ transplantation: Preoperative risk factors and the impact on health-related quality of life and life satisfaction: Health Qual Life Outcomes, 2013; 11; 111
25. Yang YS, Zhang M, Yao AM, The effect of traumatic pain on the incidence of early post-traumatic stress disorder: Chin J Emerg Med, 2020; 29(5); 665-69
26. Esser P, Kuba K, Scherwath A, Post-traumatic stress disorder symptomatology in the course of allogeneic HSCT: A prospective study: J Cancer Surviv, 2017; 11(2); 203-10
27. Kuiper H, van Leeuwen CCM, Kopsky DJ, Post-traumatic stress disorder symptoms and pain intensity in persons with spinal cord injury: Spinal Cord, 2021; 59(3); 328-35
28. Westby CL, Erlandsen AR, Nilsen SA, Depression, anxiety, PTSD, and OCD after stillbirth: A systematic review: BMC Pregnancy Childbirth, 2021; 21(1); 782
29. Maalouf FT, Haidar R, Mansour F, Anxiety, depression and PTSD in children and adolescents following the Beirut port explosion: J Affect Disord, 2022; 302; 58-65
30. Fenech AL, Van Benschoten O, Jagielo AD, Post-traumatic stress symptoms in hematopoietic stem cell transplant recipients: Transplant Cell Ther, 2021; 27(4); 341e1-341.e6
31. Song S, Yang X, Yang H, Psychological resilience as a protective factor for depression and anxiety among the public during the outbreak of COVID-19: Front Psychol, 2021; 11; 618509
32. Ran L, Wang W, Ai M, Psychological resilience, depression, anxiety, and somatization symptoms in response to COVID-19: A study of the general population in China at the peak of its epidemic: Soc Sci Med, 2020; 262; 113261
33. Zhou K, Li J, Li X, Effects of cyclic adjustment training delivered via a mobile device on psychological resilience, depression, and anxiety in Chinese post-surgical breast cancer patients: Breast Cancer Res Treat, 2019; 178(1); 95-103
In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988