20 August 2024: Original Paper
One-Year Mortality After Lung Transplantation: Experience of a Single French Center Between 2012 and 2021
Thi Cam Tu Hoang1ABCDEF, Lien Han2CDE, Sandrine Hirschi1ADEF, Tristan Degot1ADEF, Justine Leroux1ADEF, Pierre-Emmanuel FalcozDOI: 10.12659/AOT.944420
Ann Transplant 2024; 29:e944420






Abstract
BACKGROUND: Lung transplantation (LTx) is a life-extending therapy for specific patients with terminal lung diseases. This study aimed to evaluate the associations and causes of 1-year mortality after lung transplantation at Strasbourg University Hospital, France, between 2012 and 2021.
MATERIAL AND METHODS: We carried out a retrospective analysis on 425 patients who underwent LTx at Strasbourg University Hospital between January 1, 2012, and December 31, 2021. Pre-transplant, perioperative, and postoperative data were collected from the electronic medical records.
RESULTS: Among all patients, 94.6% had a LTx, 4.0% a heart-lung transplantation, and 1.4% underwent pancreatic islet-lung transplantation. The median age at transplantation was 57 years, with 55.3% male patients. The main native lung disease leading to LTx was chronic obstructive pulmonary disease in 51.1% of patients; 16.2% needed super-urgent LTx. The 1-year mortality rate was 11.5%. Most deaths were either caused by multi-organ failure or septic shock. In our multivariate analysis, we identified 3 risk factors significantly related to 1-year mortality after LTx: body mass index (BMI) between 25 and 30 kg/m² vs BMI between 18.5 and 25 kg/m² (P=0.032), postoperative extracorporeal membrane oxygenation support (P=0.034), and intensive care unit length of stay after transplantation (P<0.001). Two other factors were associated with a significantly lower 1-year mortality risk: longer hospital stay after LTx (P=0.024) and tacrolimus prescription (P=0.004).
CONCLUSIONS: Our study reported a 1-year mortality rate of 11.5% after LTx. Although LTx candidates are carefully selected, additional data are required to improve understanding of the risk factors for post-LTx mortality.
Keywords: Lung, Mortality, transplant recipients, Humans, Lung Transplantation, Male, Female, Middle Aged, France, Retrospective Studies, adult, Risk Factors, Aged, Lung Diseases, Postoperative Complications
Introduction
Lung transplantation (LTx) has been established as an effective and life-extending therapy for specific patients with terminal lung diseases, such as idiopathic pulmonary fibrosis, chronic obstructive pulmonary disease, alpha-1 antitrypsin deficiency, cystic fibrosis, and pulmonary arterial hypertension [1].
In France, the first heart-lung transplantation was performed in 1982, while the first LTx was performed in 1987. According to the French biomedicine agency data, there are 11 lung transplant centers performing approximatively 400 LTx per year in France [2].
Survival after LTx has improved due to better surgical and anesthetic techniques, bridging to LTx with extracorporeal membrane oxygenation (ECMO), perioperative management, treatment of infection, and optimization of immunosuppressive regimens. According to the registry of the International Society for Heart and Lung Transplantation (ISHLT) published in 2016, the median survival is 5.8 years after LTx for the overall underlying disease [3,4]. Various factors can affect graft longevity, and the median survival after LTx can increase, provided the patients survive the first year. According to the ISHLT registry, the worldwide 1-year mortality rate was 20.0% between 1990 and 2014 [3]. In France, the 1-year survival was 83% between 2017 and 2021 [2]. Some of the factors leading to 1-year mortality are also involved in the occurrence of chronic lung allograft dysfunction, the main limitation for long-term survival after LTx [3]. A better understanding of the risk factors involved in early post-LTx mortality remains an important challenge.
Numerous studies have investigated risk factors associated with 1-year post-LTx mortality worldwide. Factors such as advanced age, female-to-male transplantation, the need for ECMO, and the need for renal replacement therapy have been considered to affect 1-year mortality [5–7].
Therefore, in this study, we aimed to evaluate the associations and causes of 1-year mortality after LTx at Strasbourg University Hospital, France, between 2012 and 2021. The primary endpoint was all-cause 1-year mortality after LTx. The secondary endpoint was to determine pre-transplant, perioperative, and postoperative patient characteristics associated with all-cause 1-year mortality after LTx.
Material and Methods
ETHICS:
This study was approved by the Institutional Review Board of the French Learned Society for Respiratory Medicine (CEPRO 2024-011). It was conducted in accordance with the 2013 Declaration of Helsinki. Individual consent was obtained from the patients to write this study.
STUDY POPULATION:
All patients who underwent a LTx, heart-lung transplantation, or pancreatic islet-lung transplantation at the Strasbourg University Hospital between January 1, 2012, and December 31, 2021, were enrolled in the study. Recipients were followed retrospectively from the date of transplantation to 1 year after transplantation and were divided into 2 groups based on overall 1-year survival: survivors and non-survivors.
DATA COLLECTION AND DEFINITION:
Patient data were collected from the electronic medical records from Strasbourg University Hospital. The data included demographic characteristics, indication for lung transplant, nature of the transplantation (lung, heart-lung, or pancreatic islet-lung transplantation), time on waiting list before transplantation, type of transplantation, super-urgent transplantation, medical condition at the time of LTx, comorbidities, smoking status, blood type, cytomegalovirus (CMV) mismatch, laboratory test results, ischemia time, use of extracorporeal circulation or ECMO, tracheotomy, length of stay at the Intensive Care Unit (ICU) and at the hospital, immunosuppression, post-transplant complications, death at 1 year, and cause of death.
The transplant type was either unilateral or bilateral. Super-urgent transplantations were performed according to the national protocol defined by the French biomedicine agency (Agence de la biomédecine). Patients with life-threatening conditions who met the criteria for a LTx for interstitial lung disease, cystic fibrosis, or pulmonary hypertension were registered on the list for 8 days, and renewed once if necessary, after validation by a national French LTx expert [8]. Medical condition at the time of transplantation was defined as non-hospitalized, hospitalized but not in ICU, or hospitalized in ICU. Smoking status was defined as either “ever smoker” or “never smoker” (having smoked less than 100 cigarettes in a lifetime). Geographical location corresponded to the number of kilometers between the patient’s house and Strasbourg University Hospital. CMV mismatch was defined as donor positive and recipient negative for CMV serology (D+/R−). Glomerular filtration rate (GFR) was estimated from the last preoperative blood test performed prior to LTx. Forced vital capacity (FVC) and forced expiratory volume in the first second (FEV1) were collected on the listing document or from the last pulmonary function test performed before LTx. FVC and FEV1 were represented as percentages of the predicted values. Mean pulmonary artery pressure (mPAP) was measured with right heart catheterization performed before transplantation. Lung allograft ischemic time was defined as the interval from the aortic cross-clamp during the harvesting until reperfusion of the graft in the recipient. For bilateral LTx, we collected the longer ischemic time for both lungs, expressed in minutes. The induction immunosuppression administered consisted of basiliximab, Thymoglobulin, or none. Maintenance immunosuppression referred to the immunosuppressive agents administered either at the end of the first year after transplantation or at the time of death. Donor-specific anti-HLA antibodies were evaluated during the first year following the transplantation. The best post-LTx FEV1 value was the highest FEV1 measurement in the first year after transplantation, expressed in liters (L) and as a percentage of the predicted lung function. Early postoperative complications were defined as complications occurring between transplantation and discharge. Primary graft dysfunction (PGD) grade 3, defined by an acute lung injury occurring within the first 72 h after LTx and pulmonary edema associated with severe hypoxemia (PaO2/FiO2<200), without others identifiable causes, was assessed.
DATA ANALYSIS:
All data are represented as continuous or categorical variables. Continuous data are described by medians and the interquartile ranges (IQRs) between the 75th and 25th percentiles. Categorical variables are described by numbers and percentages. Univariate analysis of each factor was performed using logistic regression models. Factors with a
Results
BASELINE CHARACTERISTICS:
The median age at transplantation was 57 years, and 55.3% (n=235) were male patients. The median body mass index (BMI) was 22 kg/m2. The median waiting time from listing to transplantation was 3 months, with most patients waiting between 1 and 6 months. Overall, 94.6% (n=402) of patients received a LTx, 4.0% (n=17) a heart-lung transplantation, and 1.4% (n=6) a pancreatic islet-lung transplantation. The main indication for LTx was chronic obstructive pulmonary or alpha-1 antitrypsin deficiency, accounting for 51.1% (n=217) of patients. The other indications were interstitial lung disease (19.8%, n=84), cystic fibrosis (12.7%, n=54), pulmonary arterial hypertension (5.4%, n=23), re-transplantation (3.1%, n=13), and other rare indications (8.0%, n=34). A single LTx was performed in only 15 patients (3.5%), and 16.2% (n=69) underwent a super-urgent LTx. All characteristics of the patients are summarized in Table 1.
UNIVARIATE ANALYSIS:
Overall, 11.5% (n=49) of patients died within the first year after their LTx. The proportion of patients with a BMI between 25 and 30 kg/m2 was significantly different from that of patients with a BMI between 18.5 and 25 kg/m2 between the non-survivors and survivors (OR 2.40, 95% CI [1.15–5.03], P=0.019). Overall, 26.5% of patients had a coronary artery disease in the non-survivor group vs 15.2% in the survivor group (OR 2.02, 95% CI [0.98–3.96], Pv0.047). The median GFR in the non-survivor group was 90 mL/min (IQR 78–90) vs 90 (IQR 90–104) in the survivor group (OR 0.98, 95% CI [0.96–1.00], P=0.017). The median ischemic time was longer in the non-survivor group, at 409 min vs 375 min in the survivor group (OR 1.003, 95% CI [1.001–1.01], P=0.04). Moreover, 54.3% of the patients in the non-survivor group needed intraoperative extracorporeal circulation, compared with only 23% patients in the survivor group (OR 3.99, 95% CI [2.13–7.55], P<0.001). On the other hand, 16.7% patients required postoperative ECMO support in the non-survivor group vs 2.1% patients in the survivor group (OR 9.20, 95% CI [3.22–26.32], P<0.001). The median invasive ventilation time after transplantation was 3 days (IQR 1–10) in the non-survivor group, compared with 1 day (IQR 1–2) in the survivor group (OR 1.18, 95% CI [1.09–1.27], P<0.001). Furthermore, 33.3% of patients required post-transplant tracheotomy in the non-survivor group vs only 14.6% in the survivor group (OR 2.92, 95% CI [1.47–5.61], P=0.002). The median length of post-transplant ICU stay was 14 days (IQR 6–45) in the non-survivor group vs 7 days (IQR 5–12) in the survivor group (OR 1.05, 95% CI [1.03–1.06], P<0.001). The median length of hospital stay after transplant was 44 days (IQR 15–80) in the non-survivor group vs 36 days (IQR 33–44) in the survivor group (OR 1.01, 95% CI [1.00–1.02], P=0.016). The proportion of patients who did not receive induction immunosuppression was significantly different from that of patients who received induction immunosuppression with basiliximab between the non-survivor and survivor groups (OR 6.92, 95% CI [1.73–24.45], P=0.003). Tacrolimus was less prescribed for maintenance immunosuppression in the non-survivor group at time of death than in the survivor group at the end of the first year after LTx, at 70.6% vs 94.4%, respectively (OR 0.19, 95% CI [0.09–0.43], P<0.001). The median best FEV1 value during the first year after transplantation was significantly different between 2 groups, 2.6 L (IQR 2.1–3.1) in the survivor group vs 1.5 L (IQR 1.2–2.0) in the non-survivor group (OR 0.11, 95% CI [0.04–0.27], P<0.001), 94% [IQR 77–111] in the survivor group vs 54 [40–85] in the non-survivor group (OR 0.94, 95% CI [0.91–0.96], P<0.001) when considering the predicted values. Overall, 70.6% patients in the non-survivor group had their best FEV1 value <80% of their theoretical value during the first year after transplantation vs 27.0% patients in the survivor group (OR 6.50, 95% CI [2.35–20.9], P<0.001). There were significantly more early post-surgery complications in the non-survivor group than the survivor group: acute kidney injury requiring renal replacement therapy (61.7% vs 8.8%, OR 16.8, 95% CI [8.50–33.91], P<0.001), cardiac arrest (40.4% vs 5.3%, OR 12.08, 95% CI [5.79–25.4], P<0.001), hemothorax (27.7% vs 9.8%, OR 3.50, 95% CI [1.66–7.11], P<0.001), grade 3 PGD (71.0% vs 45.6%, OR 2.92, 95% CI [1.33–6.91], P=0.009), stroke (12.5% vs 4.3%, OR 3.21, 95% CI [1.10–8.30], P=0.021), and ICU readmission (31.2% vs 10.4%, OR 3.93, 95% CI [1.92–7.78], P<0.001) (Table 2).
In the univariate analysis, there were no differences between the survivor and non-survivor groups regarding age at transplantation, sex, waiting time from listing to transplantation, organ transplanted, indication for LTx, including re-transplantation, type of transplantation, super-urgent transplantation, medical condition at transplantation, preoperative invasive ventilation support, preoperative ECMO support, comorbidities (such as systemic hypertension, heart failure, cerebrovascular disease, gastroesophageal reflux or esophageal dysfunction or gastric ulcer, liver disease, and psychiatric disorder), smoking status, geographic location, CMV mismatch (D+/R−), pre-LTx FVC and FEV1 values, mPAP, use of Thymoglobulin as induction immunosuppression compared with basiliximab, post-transplant donor-specific anti-HLA antibodies, early infection after transplant, treated acute cellular rejection, antibody mediated rejection, and airway stenosis requiring a prosthesis within the first year after LTx (Table 2).
FACTORS ASSOCIATED WITH 1-YEAR POST-TRANSPLANTATION MORTALITY: MULTIVARIATE ANALYSIS:
The multivariate analysis included significant variables from the univariate analysis and eliminated variables with more than 5% of missing data (ischemic time, invasive ventilation time after transplantation, induction immunosuppression, best value of FEV1 within the first year after transplant, and grade 3 PGD). Multivariate analysis was performed in 410 patients with complete data for covariates.
The results revealed 3 prognostic factors associated with 1-year post-LTx mortality: BMI between 25 and 30 kg/m2 vs BMI between 18.5 and 25 kg/m2 (OR 2.50, 95% CI [1.08–5.85], P=0.032), postoperative ECMO support (OR 3.84, 95% CI [1.06–13.4], P=0.034), and ICU stay after transplantation (OR 1.07, 95% CI [1.04–1.11, P<0.001). Two variables exhibited a decreased risk: hospitalization length of stay after LTx (OR 0.98, 95% CI [0.97–1.00], P=0.024) and tacrolimus use (OR 0.24, 95% CI [0.09–0.66], P=0.004) (Table 3).
CAUSE OF DEATH:
The cause of death was not identified for 9 patients. The most common causes were multi-organ failure (37.5%, n=15) and septic shock (25%, n=10). Other causes of death were cardiac arrest (12.5%, n=5), stroke (7.5%, n=3), hemoptysis (5%, n=2), brain death (5%, n=2), digestive ischemia (2.5%, n=1), hemorrhage shock (2.5%, n=1), and transplant rejection (2.5%, n=1).
SURVIVAL CURVES:
Using the Kaplan-Meier method, we assessed the overall survival and also the 1-year survival after LTx depending on different parameters (Figure 1).
No significant difference was observed when considering the age of the patients (<60 vs 60–65 vs >65 years;
Discussion
Our study included 425 patients who underwent LTx, heart-lung transplantation, or pancreatic islet-lung transplantation over a 10-year period, from 2012 to 2021, at Strasbourg University Hospital. The 1-year mortality rate was 11.5%. A BMI between 25 and 30 kg/m2, postoperative ECMO support, and length of ICU stay after transplantation were identified as risk factors associated with 1-year mortality after LTx.
The 1-year mortality rate at our hospital was better than previous data from the literature. Roux et al [9] reported a 1-year mortality after LTx of 14% at the Foch Hospital in France between 2011 and 2014, while Sabashnikov et al [5] reported 15.6% in the United Kingdom. In the United States, the rate varied between 8% and 15% from 2013 to 2018, depending on the hospital [10]. Higher rates of 1-year mortality were described in Korea (35.3%) and Brazil (32.3%) [6,11]. According to the ISHLT registry, the worldwide 1-year mortality rate was 20.0% between 1990 and 2014 [3]. In France, the 1-year survival was 83% between 2017 and 2021 [2].
The use of ECMO support after LTx has already been identified as a risk factor associated with 1-year post-transplant mortality in a few studies [5,12]. This may be explained by an increased risk of inflammatory responses, coagulation abnormalities, or end-organ dysfunction, related to the use of ECMO. Recently, Foroutan et al [7] conducted a systematic review using meta-analytic methods to assess predictors of 1-year mortality following LTx in adults. This meta-analysis included 72 studies and 55 variables and revealed a single predictor, which was the early postoperative need for ECMO therapy.
Several studies have observed that prolonged ICU or hospital stays constituted risk factors, as they were also associated with higher mortality and poor short- and long-term outcomes after LTx [13–16]. Surprisingly, in our study, a prolonged hospital stay after LTx was associated with a decreased 1-year mortality. Our hypothesis is that patients who were hospitalized longer after LTx may have benefited from better care than in a rehabilitation center or at home. This may also be explained by the limited size of our cohort and because we assessed only the 1-year post-LTx mortality, and not beyond. The difference observed between our univariate and multivariate analyses may be explained by the wide distribution of hospitalization length of stay after LTx observed between the groups.
Many studies have found an association between being underweight or obese and poor outcomes after LTx [17,18]. Fernandez et al reported that BMI was an independent predictor of 1-year mortality. Indeed, a BMI of 26 kg/m2 was associated with the lowest probability of death, whereas BMIs ≤24 kg/m2 and ≥28 kg/m2 were associated with increased mortality [19]. Obesity might contribute to increased surgical complexity, impaired wound healing, or heightened susceptibility to infections, which could ultimately impact post-transplant outcomes. In our study, by using multivariate analysis, we observed a positive association between a BMI between 25 and 30 kg/m2 and 1-year mortality. However, there was no significant difference for patients with underweight (BMI <18.5 kg/m2) or obesity (BMI>30 kg/m2). This result may be explained by a better and stricter selection of patients with underweight or obesity during the process leading to their registration on the LTx waiting list. Thus, these patients had less comorbidities than the other LTx candidates.
Similarly, in our study, older age was not a significant marker for 1-year mortality after LTx. In the same way, this might be explained by better selection and shorter waiting times from listing to transplantation for older recipients. Even though the 1-year survival was not different by age, we observed a trend toward a better survival for patients under 60 years old, using the Kaplan-Meier method.
Immunosuppression maintenance treatments are prescribed to reduce the risk of acute and chronic rejection. Tacrolimus is one of the main immunosuppression maintenance treatments, and patients not receiving tacrolimus at the time of death or at the end of the first year presented a significantly higher risk of 1-year mortality after LTx in our study. One explanation may be that tacrolimus is considered a more efficient immunosuppressive agent than cyclosporine and everolimus, although to date, no trial has shown a statistically significant difference regarding the risk of developing an acute rejection or regarding the survival between patients treated with tacrolimus or cyclosporine [20,21]. Considering the increased risk of acute rejection within the first year after LTx and its effect on patient morbidity and mortality, this may explain why patients without tacrolimus exhibited a higher rate of 1-year mortality [22,23]. In our center, tacrolimus is used for all patients undergoing LTx. However, for some of them, tacrolimus was sometimes stopped, mostly because of adverse effects, such as encephalopathy or renal toxicity. We can hypothesize that patients for whom tacrolimus was suspended may have developed more comorbidities and may have had a higher frailty than patients under tacrolimus, which may have led to a higher mortality by the end of the first year after LTx. Regarding immunosuppression regimens, protection against post-LTx complications, such acute rejection, no significant protective effect of one drug compared with others was observed in several previous studies. However, tacrolimus plus mycophenolate mofetil is the most commonly used regimen after LTx [23]. Our findings may encourage LTx centers to keep optimizing immunosuppressive drug dosing, especially tacrolimus, and monitoring for adverse effects. Further studies are needed to explore alternative immunosuppressive strategies for patients who cannot tolerate tacrolimus, without increasing the risk of post-LTx complications.
One-year mortality was not different regarding the native lung disease and transplant type. Most patients underwent double lung transplantation, and single lung transplantation was usually for older patients with interstitial lung disease. One-year survival seemed to be better for double vs single lung transplantation, using the Kaplan-Meier method, but it was not significant. We did not find any statistical differences regarding 1-year mortality between patients who were hospitalized compared with those who were at home just before LTx. Patients who required preoperative invasive ventilation and preoperative ECMO support were associated with life-threatening risks and usually had super-urgent procedure for LTx. However, our study did not show any difference in 1-year mortality for these variables. Cardiovascular disease and diabetes mellitus influenced LTx outcomes in several previous studies; however, we did not observe the same results [24,25]. Similarly, CMV mismatch (D+/R−) or pretransplant laboratory values (GFR, FVC, FEV1, and mPAP), identified as risk factors in previous articles, were not established as significant risk factors in our study. Ischemic time and prolonged mechanical ventilation after LTx had an impact on short- and long-term survival. Unfortunately, we could not include these variables in multivariate analysis due to missing data: 8.7% and 17.4%, respectively [26–28]. None of the postoperative complications assessed in our study were associated with 1-year mortality after LTx.
Our cohort is the second largest cohort in France in which 1-year mortality after LTx was studied, after the Foch Hospital cohort. We reported recent results from patients who underwent LTx in our center between 2012 and 2021. Other strengths of our study are that patients underwent the same criteria selection for LTx, and the surgical techniques, as well as perioperative management and immunosuppression regimens, did not vary much during the study period.
However, the current results should be interpreted considering some limitations. First, this study is a retrospective analysis from a single hospital. We can imagine that some variations between LTx centers for surgical techniques, post-transplant management protocols, or regarding LTx patient populations might affect the observed risk factors in our own study. Second, several variables were not considered for this work, such as donor characteristics and pre-transplant anti-HLA antibodies, due to lack of data. Of note, these variables might also have an affect 1-year mortality post-LTx. Third, because of missing data, we could not include ischemic time, invasive ventilation time after transplantation, and best value of FEV1 <80% within the first year after transplantation, and grade 3 PGD in our multivariate analysis.
Conclusions
Our study reported recent results of 1-year mortality after LTx in a French medium-sized LTx center. We observed a 1-year mortality rate of 11.5%, which was lower than previous data from the literature. A BMI between 25 and 30 kg/m2, prolonged ICU stay, and need for postoperative ECMO support were identified as risk factors in our study. Although candidates for LTx are carefully selected, additional data are strongly required from prospective and multicenter studies to improve our knowledge and understanding of post-LTx morbidity and mortality risk factors, especially during the first year after LTx.

Tables
Table 1. Characteristics of lung transplant patients followed up at Strasbourg University Hospital between 2012 and 2021.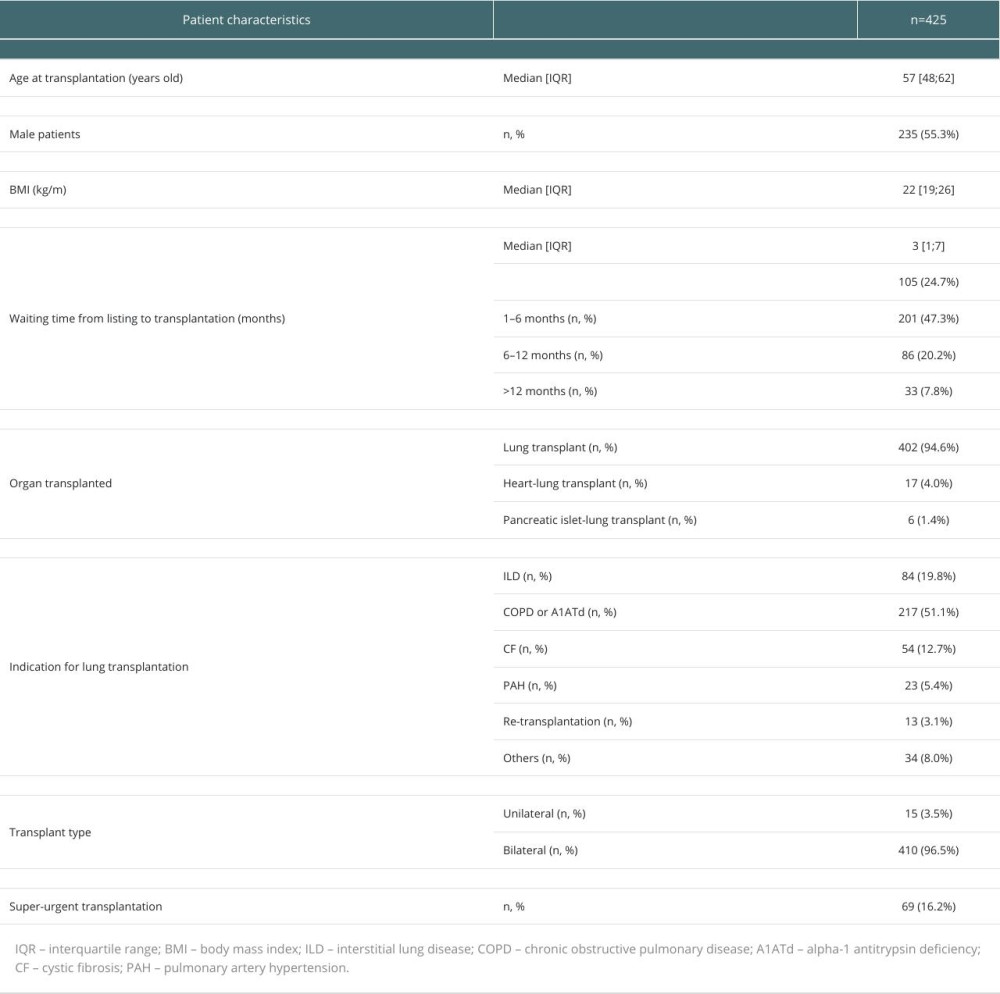 Table 2. Characteristics of patients who survived and those who died during the first year after lung transplantation between 2012 and 2021.
Table 2. Characteristics of patients who survived and those who died during the first year after lung transplantation between 2012 and 2021.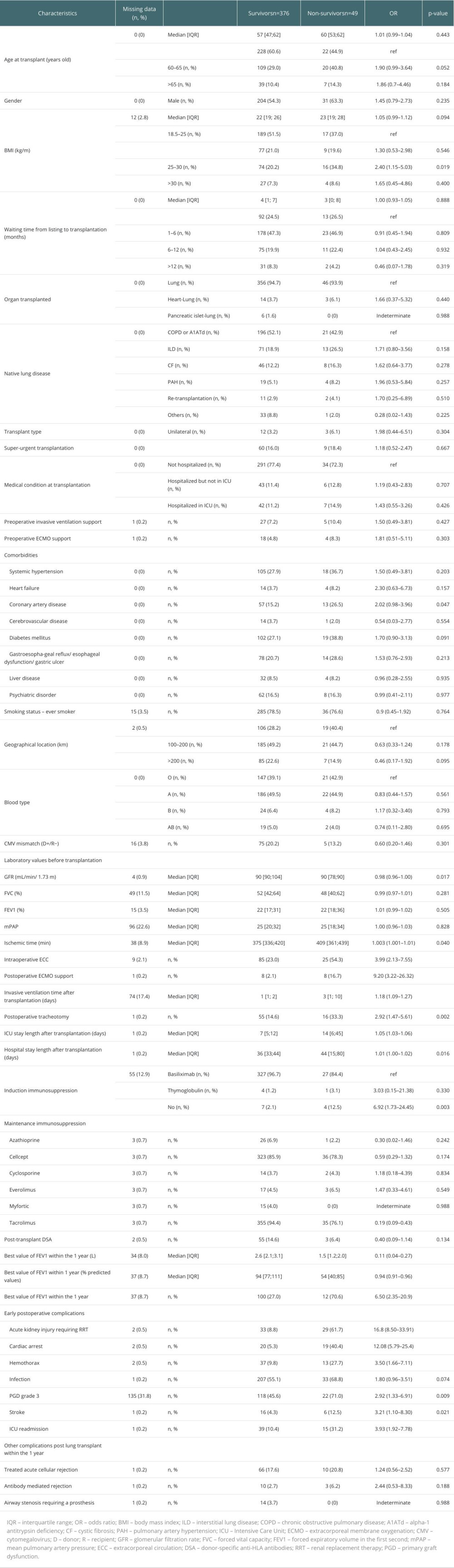 Table 3. Multivariate analysis.
Table 3. Multivariate analysis.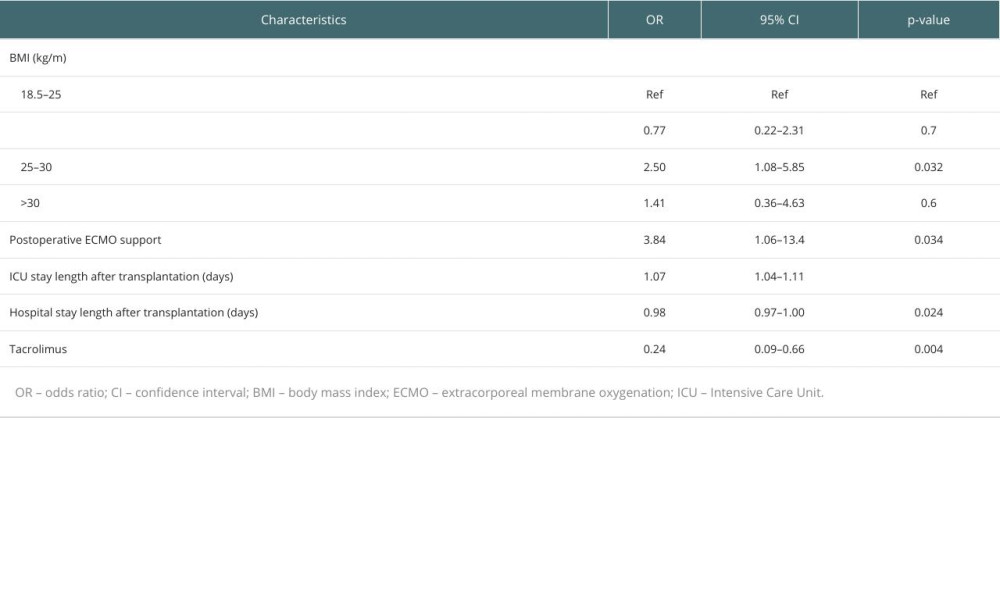
References
1. Leard LE, Holm AM, Valapour M, Consensus document for the selection of lung transplant candidates: An update from the International Society for Heart and Lung Transplantation: J Heart Lung Transplant, 2021; 40(11); 1349-79
2. : Agence de la biomédecine Available from: [in French]https://rams.agence-biomedecine.fr/greffe-cardio-pulmonaire-et-pulmonaire-0
3. Yusen RD, Edwards LB, Dipchand AI, The Registry of the International Society for Heart and Lung Transplantation: Thirty-third adult lung and heart–lung transplant report – 2016; Focus theme: Primary diagnostic indications for transplant: J Heart Lung Transplant, 2016; 35(10); 1170-84
4. Thabut G, Mal H, Outcomes after lung transplantation: J Thorac Dis, 2017; 9(8); 2684-91
5. Sabashnikov A, Weymann A, Mohite PN, Risk factors predictive of one-year mortality after lung transplantation: Eur J Cardiothorac Surg, 2014; 46(6); e82-88
6. Lee SH, Park MS, Song JH, Perioperative factors associated with 1-year mortality after lung transplantation: A single-center experience in Korea: J Thorac Dis, 2017; 9(10); 4006-16
7. Foroutan F, Malik A, Clark KE, Predictors of 1-year mortality after adult lung transplantation: Systematic review and meta-analyses: J Heart Lung Transplant, 2022; 41(7); 937-51
8. Agence de la biomédecine: Procedures d’application des Regles de Repartition Et d’attribution des Greffons Preleves Sur Personne Decedee Published online 2013. Available from: [in French]https://www.agence-biomedecine.fr/IMG/pdf/regles_repartition_organes_decembre2013.pdf
9. Roux A, Sage E, Cerf CEvolution and progress of lung transplantation: An analysis of a cohort of 600 lung transplant patients at the Hospital Foch: Rev Mal Respir, 2019; 36(2); 142-54 [in French]
10. Wakeam E, Thumma JR, Bonner SN, One-year mortality is not a reliable indicator of lung transplant center performance: Ann Thorac Surg, 2022; 114(1); 225-32
11. Machuca TN, Schio SM, Camargo SM, Prognostic factors in lung transplantation: the Santa Casa de Porto Alegre experience: Transplantation, 2011; 91(11); 1297-303
12. Boffini M, Simonato E, Ricci D, Extracorporeal membrane oxygenation after lung transplantation: Risk factors and outcomes analysis: Ann Cardiothorac Surg, 2019; 8(1); 54-61
13. Ong LP, Tristan Z, Prahbu M, Prolonged Intensive Care Unit stay after bilateral lung transplantation – late mortality & functional outcome?: J Heart Lung Transplant, 2014; 33(4); S294
14. Tanaka S, Geneve C, Tebano G, Morbidity and mortality related to pneumonia and TRACHEOBRONCHITIS in ICU after lung transplantation: BMC Pulm Med, 2018; 18(1); 43
15. Tran-Dinh A, Guiot M, Tanaka S, Bacteraemia is associated with increased ICU mortality in the postoperative course of lung transplantation: Antibiotics (Basel), 2022; 11(10); 1405
16. Banga A, Mohanka M, Mullins J, Hospital length of stay after lung transplantation: Independent predictors and association with early and late survival: J Heart Lung Transplant, 2017; 36(3); 289-96
17. Upala S, Panichsillapakit T, Wijarnpreecha K, Underweight and obesity increase the risk of mortality after lung transplantation: A systematic review and meta-analysis: Transpl Int, 2016; 29(3); 285-96
18. Allen JG, Arnaoutakis GJ, Weiss ES, The impact of recipient body mass index on survival after lung transplantation: J Heart Lung Transplant, 2010; 29(9); 1026-33
19. Fernandez R, Safaeinili N, Kurihara C, Association of body mass index with lung transplantation survival in the United States following implementation of the lung allocation score: J Thorac Cardiovasc Surg, 2018; 155(4); 1871-79e3
20. Zuckermann A, Reichenspurner H, Birsan T, Cyclosporine A versus tacrolimus in combination with mycophenolate mofetil and steroids as primary immunosuppression after lung transplantation: One-year results of a 2-center prospective randomized trial: J Thorac Cardiovasc Surg, 2003; 125(4); 891-900
21. Treede H, Glanville AR, Klepetko WEuropean and Australian Investigators in Lung Transplantation, Tacrolimus and cyclosporine have differential effects on the risk of development of bronchiolitis obliterans syndrome: Results of a prospective, randomized international trial in lung transplantation: J Heart Lung Transplant, 2012; 31(8); 797-804
22. Krustrup D, Iversen M, Martinussen T, Andersen CB, Time elapsed after transplantation influences the relationship between the number of regulatory T cells in lung allograft biopsies and subsequent acute rejection episodes: Transpl Immunol, 2014; 31(1); 42-27
23. Renaud-Picard B, Koutsokera A, Cabanero M, Martinu T, Acute rejection in the modern lung transplant era: Semin Respir Crit Care Med, 2021; 42(3); 411-27
24. Plantier L, Skhiri N, Biondi G, Impact of previous cardiovascular disease on the outcome of lung transplantation: J Heart Lung Transplant, 2010; 29(11); 1270-76
25. Hackman KL, Bailey MJ, Snell GI, Bach LA, Diabetes is a major risk factor for mortality after lung transplantation: Am J Transplant, 2014; 14(2); 438-45
26. Ghaidan H, Fakhro M, Lindstedt S, Impact of allograft ischemic time on long-term survival in lung transplantation: A Swedish monocentric study: Scand Cardiovasc J, 2020; 54(5); 322-29
27. Novick RJ, Bennett LE, Meyer DM, Hosenpud JD, Influence of graft ischemic time and donor age on survival after lung transplantation: J Heart Lung Transplant, 1999; 18(5); 425-31
28. Atchade E, Boughaba A, Dinh AT, Prolonged mechanical ventilation after lung transplantation: Risks factors and consequences on recipient outcome: Front Med (Lausanne), 2023; 10; 1160621
Tables
Table 1. Characteristics of lung transplant patients followed up at Strasbourg University Hospital between 2012 and 2021.Table 2. Characteristics of patients who survived and those who died during the first year after lung transplantation between 2012 and 2021.Table 3. Multivariate analysis.Table 1. Characteristics of lung transplant patients followed up at Strasbourg University Hospital between 2012 and 2021.Table 2. Characteristics of patients who survived and those who died during the first year after lung transplantation between 2012 and 2021.Table 3. Multivariate analysis. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988