06 May 2025: Original Paper
Splenic Artery Ligation: Effects on Portal Flow and Hypersplenism in Living Donor Liver Transplantation
Sinan Efe Yazici DOI: 10.12659/AOT.947760
Ann Transplant 2025; 30:e947760






Abstract
BACKGROUND: Living donor liver transplantation (LDLT) has been shown to be safe in the curative treatment of liver cirrhosis. Portal flow modulation techniques, such as splenic artery ligation (SAL), have been used to avoid complications like small-for-size syndrome (SFSS). However, the effects of SAL on portal flow, splenic function, and hematologic outcomes remain underexplored.
MATERIAL AND METHODS: This retrospective study analyzed 60 LDLT recipients treated at a single center from January 2023 to December 2024. Thirty patients underwent SAL (SAL+) while 30 did not undergo SAL (SAL-). Data on demographic and clinical characteristics, portal flow dynamics, spleen volume, hematologic parameters, and postoperative complications were collected and analyzed using IBM SPSS 20.0. Statistical significance was set at P<0.05.
RESULTS: SAL significantly reduced portal flow from 3148±989 mL/min to 1949±830 mL/min (P<0.001), optimizing the portal flow/graft weight ratio. SAL also decreased splenic volume by 21% and alleviated thrombocytopenia, with postoperative platelet counts increasing 3.8-fold compared to preoperative levels (P<0.001). There were fewer complications in the SAL+ group, with significant reductions in biliary complications and improved graft function. No severe ischemic splenic changes or thromboembolic events were observed in the SAL+ group.
CONCLUSIONS: SAL is an effective strategy for portal flow modulation in LDLT, significantly reducing portal flow to optimal levels and improving hematologic outcomes. By preserving splenic function and minimizing complications, SAL is a safe and beneficial approach to managing SFSS and improving graft performance in LDLT patients.
Keywords: Liver Transplantation, Living Donors, Portal System, Spleen, Splenic Artery, Thrombocytopenia, Humans, Female, Male, Retrospective Studies, Middle Aged, hypersplenism, Ligation, adult, Postoperative Complications
Introduction
Living donor liver transplantation (LDLT) has been shown to be safe in the curative treatment of liver cirrhosis and has many advantages over cadaveric liver transplantation [1]. The development of living donor liver transplantation in transplant surgery has led to a revival of interest in hepatic hemodynamics. Portal hypertension can persist after liver transplantation, especially in partial liver transplant recipients. A successful LDLT operation depends on adequate volume of the transplanted liver graft and an appropriate balance of portal vein inflow and hepatic vein outflow [2].
When the liver graft is too small to meet the metabolic needs of the recipient, the recipient may have small-for-size syndrome (SFSS). SFSS is clinically manifested by impaired coagulation, cholestasis, and ascites, resulting in septic complications and lower graft survival [3,4]. The basic pathophysiology of this syndrome is that the graft receives portal overflow, resulting in sinusoidal congestion and hemorrhage [5]. As a secondary effect of portal overflow, arterial vasoconstriction leads to ischemic damage. Portal flow modulation improves graft function by increasing arterial flow [6].
SFSS typically occurs when the graft volume is less than 0.8% of the graft-recipient weight ratio (GRWR) [7]. For these grafts, an optimal portal vein flow (PVF) of 250 mL/min/100 g is recommended [8]. Several methods have been attempted to avoid SFSS. These include splenic artery ligation (SAL), splenectomy, and the diversion of portal venous blood through mesocaval, portocaval, or inferior mesenteric shunts [9,10].
In chronic liver diseases, splenomegaly and hypersplenism may develop following the onset of portal hypertension [11]. Thrombocytopenia is a common hematological disorder in patients with chronic liver disease, with the severity of liver disease being the most significant factor. The pathophysiology of thrombocytopenia in chronic liver disease has been shown to be associated with the hypersplenism hypothesis, in which portal hypertension leads to accumulation and sequestration of all blood cellular elements, particularly platelets, in the enlarged and congested spleen.
The aim of this study was to investigate both the effects of portal flow modulation and the recovery process of hematological disorders such as hypersplenism and thrombocytopenia in patients undergoing splenic artery ligation following liver transplantation. These findings may provide an important clinical guideline for the management of hematological complications after liver transplantation and contribute to a better understanding of the postoperative effects of surgical interventions.
Material and Methods
ETHICAL CONSIDERATIONS:
The study was approved by the institutional ethics committee, and informed consent was obtained from all participants. The study followed the principles outlined in the Declaration of Helsinki.
PARTICIPANTS:
A total of 60 liver transplant recipients were included in the study −30 patients underwent splenic artery ligation and 30 patients in the control group did not undergo splenic artery ligation.
DEMOGRAPHIC AND CLINICAL DATA:
The demographic and clinical characteristics of the patients, including sex, age, and etiology of liver cirrhosis, were evaluated. Additionally, the Model for End-Stage Liver Disease sodium (MELD-Na) score and Child-Pugh score were used to determine the severity of liver disease. Intraoperative variables, including intraoperative bleeding volume, need for blood transfusion, and graft weight measured at surgery, were recorded. The GRWR was calculated to evaluate the adequacy of the graft weight relative to the recipient. In the first 30 days complications were monitored and recorded to assess the outcomes of the procedure. Intraoperative findings were recorded, including intraoperative bleeding measured in milliliters (mL). The need for blood transfusion was also documented, with the number of units transfused being recorded for each patient.
LABORATORY DATA:
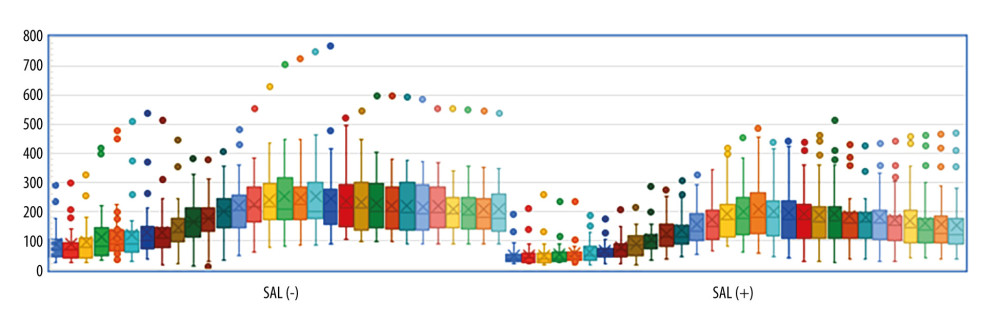
Patients’ platelet values immediately before surgery as well as their platelet levels during the first month after surgery were recorded. In addition, amylase values were recorded on the first postoperative day as part of routine monitoring. Platelet and amylase values were obtained from the hospital’s electronic health record system. Platelet values are reported in ×109/L and amylase values are reported in U/L.
CROSS-SECTIONAL IMAGING:
All recipients underwent preoperative contrast-enhanced computed tomography (CT) to visualize the portal system. In the arterial phase of the CT, the presence of splenic artery aneurysms was specifically evaluated. The spleen volumes were calculated using Myrian® 2.7.1 software, an advanced imaging application designed for organ segmentation. The volumetric analysis was performed using the venous phase of the contrast-enhanced CT scans, which offers optimal visualization of the splenic parenchyma for accurate measurements.
Postoperatively, a follow-up CT scan was performed at 1 month as part of the routine follow-up protocol. During this scan, the healthy spleen and the ischemic area were measured to assess the effects of the surgical procedure and any potential complications related to splenic perfusion.
ULTRASOUND IMAGING:
Intraoperatively, portal flow was assessed using Doppler ultrasonography. Portal flow measurements were taken before and after ligation of the splenic artery to evaluate the effects of the procedure on portal circulation. The changes in portal flow were compared, and the results were analyzed to determine how the ligation influenced portal dynamics. The ratio of portal flow to liver graft weight was calculated and analyzed.
DECISION TO PERFORM SPLENIC ARTERY LIGATION AND SURGICAL TECHNIQUE:
The ligation decision was made according to the presence of aneurysm in the splenic artery, and the portal flow-to-graft weight ratio.
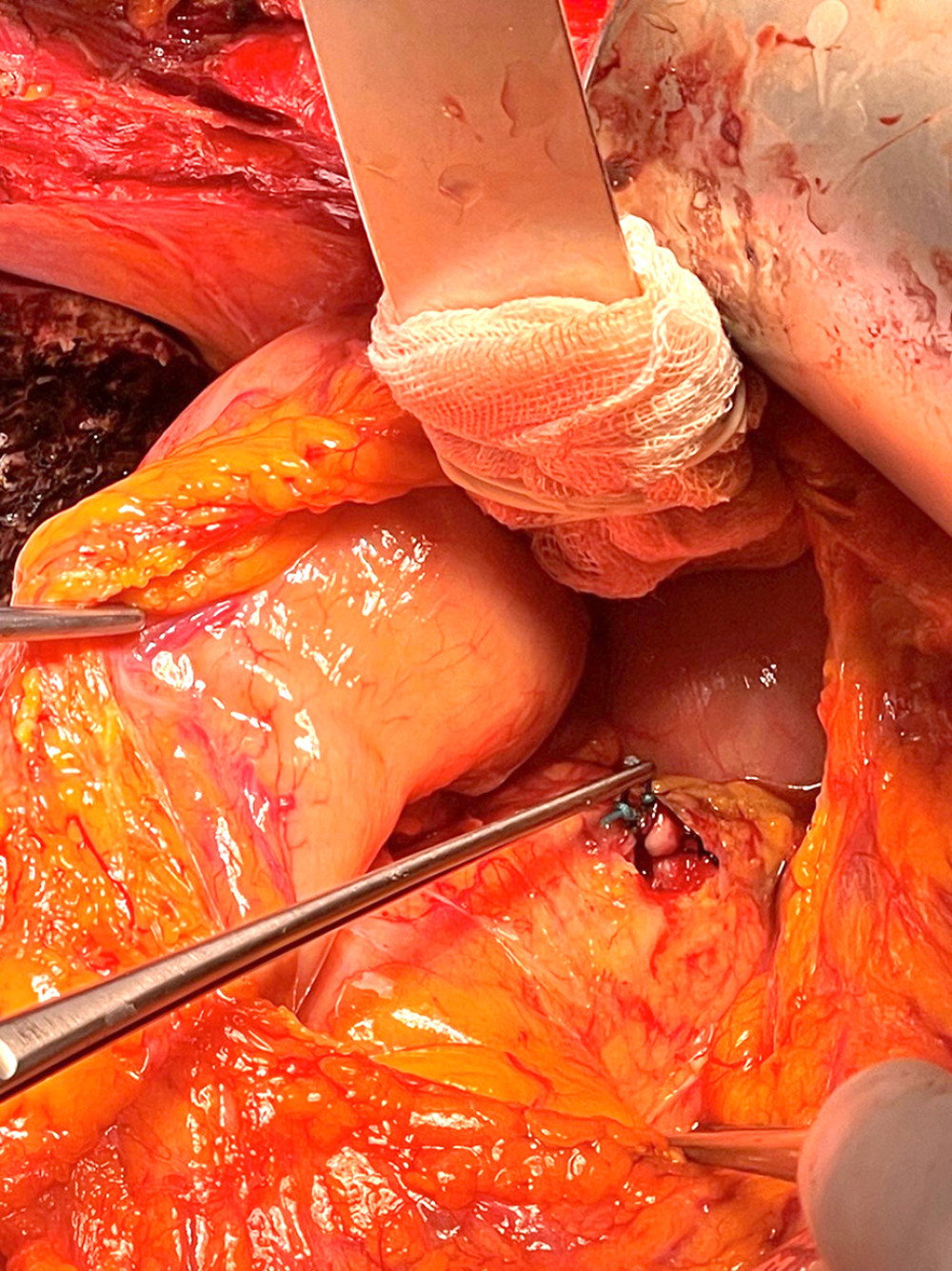
The gastrocolic ligament was opened. The splenic artery was dissected over the pancreas. Depending on the density of collaterals in the region, the splenic artery was ligated with thick, non-absorbable material from 2 separate points from the safe dissection area (Figure 1).
COMPLICATIONS:
Complications were categorized into 4 groups: bleeding, portal vein thrombosis (PVT), biliary complications, and “none.” Bleeding complications included significant hemorrhage requiring re-exploration or further surgical intervention. PVT was defined as any occlusion or thrombus formation in the portal vein detected during or after the transplant procedure. Biliary complications encompassed issues such as bile leaks, strictures, or obstruction that required surgical, endoscopic, or percutaneous intervention. Patients who did not experience any of these complications were categorized as “none”.
STATISTICAL ANALYSES:
The data were analyzed using IBM SPSS 20.0 software. Descriptive statistics are presented as frequencies (n, %) for categorical variables, and as mean±standard deviation or median (Q1–Q3) for continuous variables. The normality assumption was tested using the Kolmogorov-Smirnov test. In cases where the assumptions for parametric tests were not met, the differences between independent groups were analyzed using the Mann-Whitney U test. When parametric test assumptions were satisfied, differences between means were analyzed using the independent-samples
Results
A total of 60 patients were included in the study −30 in the splenic artery ligation (SAL +) group and 30 in the no splenic artery ligation group (SAL −). The sex distribution in the entire cohort was 20 females (33.3%) and 40 males (66.7%). The median age of the patients was 56 years (IQR: 43–62), and no significant age difference was observed between the groups (
The MELD-Na scores of the total patient cohort ranged from 9 to 20, with a median of 14 (IQR: 10–20), indicating moderate liver disease severity. In terms of Child-Pugh classification, 30% of patients were classified as Child-Pugh A, 53.3% as Child-Pugh B, and 16.7% as Child-Pugh C. There was no significant difference in either the MELD-Na or Child-Pugh scores between the SAL (+) and SAL (−) groups (
GRWR was comparable between the groups, with a mean value of 1.08±0.19 in the SAL (+) group and 1.13±0.24 in the SAL (−) group (
Biochemical and radiological data are summarized in Table 3. Preoperative platelet counts were significantly lower in the SAL (+) group compared to the SAL (−) group (
Preoperative spleen volumes were significantly larger in the SAL (+) group than in the SAL (−) group (
In the SAL (+) group, more patients experienced no complications compared to the SAL (−) group. Biliary complications were more frequent in the SAL (−) group, while bleeding complication requiring re-exploration and portal vein thrombosis occurred only in the SAL (+) group. Data on complications are summarized in Table 4.
Portal flow decreased significantly following splenic artery ligation, from 3147.7±989.1 mL/min before ligation to 1949.2±829.8 mL/min after ligation (
Discussion
In living donor liver transplantation, it is thought that excessive portal flow following perfusion leads to sinusoidal congestion and hemorrhage, forming the fundamental mechanism of small-for-size graft syndrome (SFSS) [5]. There are numerous studies suggesting that the damage caused by portal overflow to the liver can be mitigated through portal modulation, potentially improving graft functions [12]. In our study, the reason for focusing on portal flow rather than portal pressure in portal flow modulation is that portal pressure is influenced by central venous pressure [13].
Portal venous flow below 250 mL/min/100 g is associated with poor graft outcomes [8,14]. In our study, a PVF of 100–250 ml/min/100 g was considered optimal. SAL was performed in patients with PVF above this level. We analyzed the effect of splenic artery ligation on the PVF/graft weight ratio in liver transplant recipients. In particular, the mean portal flow rate was approximately 4 times the graft weight before splenic artery ligation and decreased to less than 2.5 times after splenic artery ligation, showing that portal flow rate was reduced to optimal limits to avoid the adverse effects of portal overflow on the liver graft.
It has been reported in the literature that there can be a decrease in portal venous flow after splenic artery ligation [15], and Su et al showed that splenic artery ligation decreased portal blood flow by 14.3% [16].
In our study, a 37% decrease in portal venous flow was observed in patients who underwent splenic artery ligation after the procedure. The 37% reduction in our study is slightly higher than the values in previous studies. This difference may be due to differences in patient selection, surgical technique, measurement methods, timing, patient population characteristics, or clinical protocols. In conclusion, our study suggests that SAL can help preserve the short- and possibly long-term functional integrity of the graft by significantly reducing excess portal flow in living donor liver transplants.
Many methods can be used in portal modulation, including splenectomy [17], splenic artery embolization [18], splenic artery ligation [19], porto-systemic shunts [20], and somatostatin [21].
The exclusion of patients on somatostatin aimed to eliminate potential confounding factors for the effect of splenic artery ligation in our study.
When considering options to reduce portal vein blood flow, there is substantial evidence showing splenic artery ligation is preferable to splenectomy [22]. Samimi et al demonstrated significantly higher patient mortality in liver transplant recipients undergoing concomitant splenectomy, mainly as a result of early and late septic complications [23]. Ito et al reported that splenectomy was associated with longer operative time, greater blood loss, and a higher risk of venous thrombosis and infection [24]. Splenectomy weakens the defense against encapsulated bacteria and increases the risk of serious and life-threatening infections, especially in immunocompromised patients [25].
In our study, there was no significant difference in blood loss and transfusion needs between the groups with and without splenic artery ligation. There was no significant difference in the incidence of venous thrombosis. Serious bacterial infections were not observed. This situation is especially critical for patients receiving immunosuppressive therapy after liver transplantation. Our results suggest that splenic artery ligation provides significant advantages in clinical management by preserving splenic integrity and function in the liver transplant patients. It has been reported in the literature that thromboembolic complications can occur due to excessive platelet increase, which is frequently seen after splenectomy, and that this situation may require antithrombotic treatment and should be followed closely [16].
In our study, although there was a significant difference between the postoperative peak platelet values of the patients with and without SAL in favor of the SAL group, the postoperative 1-month platelet values remained within normal limits and thromboembolic complications due to excessive platelet increase were not significantly detected, thus reducing the need for long-term anticoagulant use. This result suggests that splenic artery ligation is also advantageous in terms of preserving the long-term hematologic balance of the patients.
Although splenic artery embolization is an effective method to reduce portal flow of small grafts after liver transplantation [18], ischemic complications of splenic artery embolization, such as splenic infarction, have also been reported in the literature [26]. In our series, only a small splenic area (5.51%) was ischemic in 18 patients with SAL and there was no significant splenic infarction. This shows that the spleen can be protected from ischemic changes by providing adequate perfusion through additional vascular sources such as short gastric, gastroepiploic, and omental vessels, and that ischemic complications after embolization can be minimized. Splenomegaly causes sequestration of blood products in the splenic sinusoids and the literature suggests an association between splenomegaly and resultant cytopenias [27].
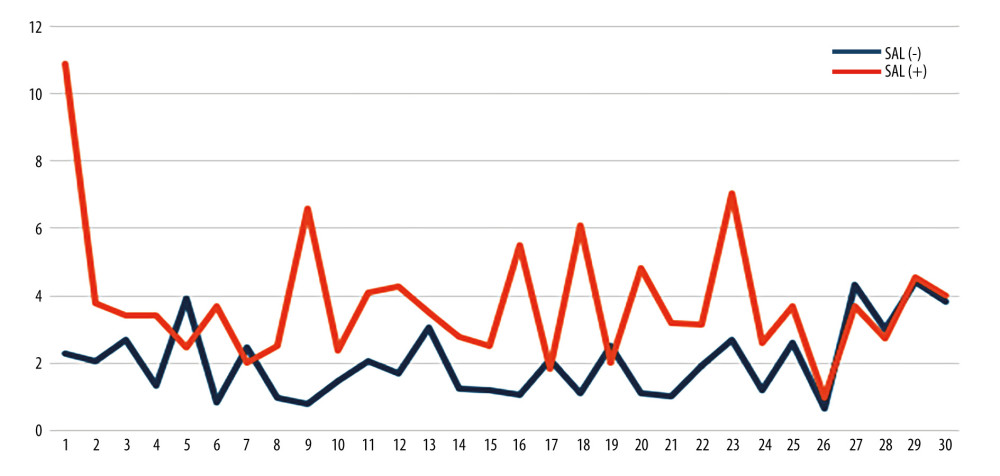
The present study show that SAL significantly improves splenic volume and platelet values in living donor liver transplant patients. First, the percentage change in splenic volume in the group that underwent SAL showed a significantly more pronounced decrease than in the group that did not undergo SAL. This finding suggests that SAL alleviates splenic sequestration due to hypersplenism by significantly reducing splenic volume. Secondly, the positive effect of SAL on platelet values was also clearly demonstrated. The ratio of postoperative peak platelet values to preoperative values was significantly higher in patients who underwent SAL compared to the group without SAL. This increase indicates that hematologic complications related to hypersplenism such as thrombocytopenia can be effectively controlled by SAL. This improvement may be explained by decreased sequestration due to decreased splenic volume and increased circulating effective platelet count.
Taken together, these 2 statistical findings suggest that SAL modulates portal hemodynamics and normalizes hematologic balance by improving signs of hypersplenism to a clinically relevant extent. Compared to alternative methods such as splenectomy and splenic artery embolization, splenic artery ligation is an approach that minimizes the risk of ischemia, maintains immunological protection, supports hematologic balance in the long term, and reduces potential complications.
This study has several limitations. First, this is a retrospective study with a small sample size at a single center. Second, the effect of low portal venous outflow was not analyzed. Third, patients with shunts were not included. Future larger, multicenter, prospective studies may more comprehensively confirm these multifaceted benefits of splenic artery ligation.
Conclusions
SAL in LDLT significantly reduces the risk of damage to the graft from portal overflow. SAL also was shown to significantly reduce splenic volume, alleviate sequestration due to splenomegaly, and improve thrombocytopenia, with significant improvements in platelet count. SAL as an effective method that not only optimizes portal flow but also promotes hematologic balance, improving graft function and patient outcomes.

References
1. Roubil JG, Martins PN, Babak M, Resolution of severe graft steatosis before living-donor liver transplant after 86 pounds of weight loss: Exp Clin Transplant, 2022; 20(9); 874-77
2. Kelly DM, Miller C, Understanding the splenic contribution to portal flow: The role of splenic artery ligation as inflow modification in living donor liver transplantation: Liver Transpl, 2006; 12(8); 1186-88
3. Dahm F, Georgiev P, Clavien PA, Small-for-size syndrome after partial liver transplantation: Definition, mechanisms of disease and clinical implications: Am J Transplant, 2005; 5(11); 2605-10
4. Kiuchi T, Kasahara M, Uryuhara K, Impact of graft size mismatching on graft prognosis in liver transplantation from living donors: Transplantation, 1999; 67(2); 321-27
5. Etesami K, Genyk Y, The increasingly limited basis for portal venous pressure modulation in living donor liver transplantation: Liver Transpl, 2018; 24(11); 1506-7
6. Yoshizumi T, Mori M, Portal flow modulation in living donor liver transplantation: Review with a focus on splenectomy: Surg Today, 2020; 50(1); 21-29 [Erratum in: Surg Today. 2020;50(4):423]
7. Masuda Y, Yoshizawa K, Ohno Y, Small-for-size syndrome in liver transplantation: Definition, pathophysiology and management: Hepatobiliary Pancreat Dis Int, 2020; 19(4); 334-41
8. Troisi R, de Hemptinne B, Clinical relevance of adapting portal vein flow in living donor liver transplantation in adult patients: Liver Transpl, 2003; 9(9); S36-41
9. Troisi R, Cammu G, Militerno G, Modulation of portal graft inflow: A necessity in adult living-donor liver transplantation?: Ann Surg, 2003; 237(3); 429-36
10. Ku Y, Fukumoto T, Nishida T, Evidence that portal vein decompression improves survival of canine quarter orthotopic liver transplantation: Transplantation, 1995; 59(10); 1388-92
11. Li L, Duan M, Chen W, The spleen in liver cirrhosis: revisiting an old enemy with novel targets: J Transl Med, 2017; 15(1); 111
12. Emond JC, Goodrich NP, Pomposelli JJ, Hepatic hemodynamics and portal flow modulation: The A2ALL experience: Transplantation, 2017; 101(10); 2375-84
13. Sainz-Barriga M, Scudeller L, Costa MG, Lack of a correlation between portal vein flow and pressure: Toward a shared interpretation of hemodynamic stress governing inflow modulation in liver transplantation: Liver Transpl, 2011; 17(7); 836-48
14. Yamada T, Tanaka K, Uryuhara K, Selective hemi-portocaval shunt based on portal vein pressure for small-for-size graft in adult living donor liver transplantation: Am J Transplant, 2008; 8(4); 847-53
15. Su CM, Chou TC, Yang TH, Lin YJ, Graft inflow modulation in living-donor liver transplantation: Hepatic hemodynamic changes in splenic artery ligation and splenectomy: Ann Transplant, 2022; 27; e936609
16. Ikegami T, Balci D, Jung DH, Living donor liver transplantation in small-for-size setting: Int J Surg, 2020; 82S; 134-37
17. Taha AMI, Temerik AR, Eweis MK, Splenic artery ligation versus splenectomy for portal inflow modulation in adult living donor liver transplant: Effects on early graft function, a prospective study: Exp Clin Transplant, 2024; 22(10); 794-99
18. Gruttadauria S, Mandala’ L, Miraglia R, Successful treatment of small-for-size syndrome in adult-to-adult living-related liver transplantation: single center series: Clin Transplant, 2007; 21(6); 761-66
19. Troisi R, Hoste E, Van Langenhove P, Modulation of liver graft hemodynamics by partial ablation of the splenic circuit: A way to increase hepatic artery flow?: Transplant Proc, 2001; 33(1–2); 1445-46
20. Troisi R, Ricciardi S, Smeets P, Effects of hemi-portocaval shunts for inflow modulation on the outcome of small-for-size grafts in living donor liver transplantation: Am J Transplant, 2005; 5(6); 1397-404
21. Hessheimer AJ, Escobar B, Muñoz J, Somatostatin therapy protects porcine livers in small-for-size liver transplantation: Am J Transplant, 2014; 14(8); 1806-16
22. Shimada M, Ijichi H, Yonemura Y, The impact of splenectomy or splenic artery ligation on the outcome of a living donor adult liver transplantation using a left lobe graft: Hepatogastroenterology, 2004; 51(57); 625-29
23. Samimi F, Irish WD, Eghtesad B, Role of splenectomy in human liver transplantation under modern-day immunosuppression: Dig Dis Sci, 1998; 43(9); 1931-37
24. Ito K, Akamatsu N, Ichida A, Splenectomy is not indicated in living donor liver transplantation: Liver Transpl, 2016; 22(11); 1526-35
25. Lynch AM, Kapila R, Overwhelming postsplenectomy infection: Infect Dis Clin North Am, 1996; 10(4); 693-707
26. Chao CP, Nguyen JH, Paz-Fumagalli R, Splenic embolization in liver transplant recipients: Early outcomes: Transplant Proc, 2007; 39(10); 3194-98
27. Tan CH, Hall JA, Hammonds K, Dodlapati J, Relationship between splenomegaly and transfusion requirements in patients with cirrhosis: Proc (Bayl Univ Med Cent), 2020; 34(1); 44-48
Figures
Tables
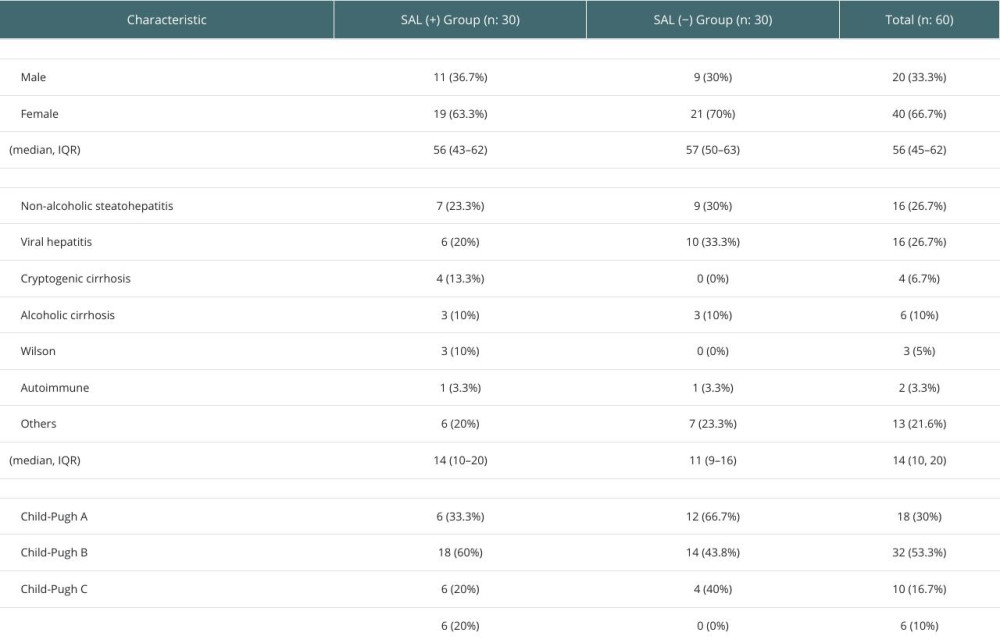 Table 1. Demographic and clinical sata.
Table 1. Demographic and clinical sata. Table 2. Intraoperative data.
Table 2. Intraoperative data. Table 3. Biochemical and radiological data.
Table 3. Biochemical and radiological data. Table 4. Complications.
Table 4. Complications. Table 5. Pre- and post-splenic artery ligation data.Table 1. Demographic and clinical sata.Table 2. Intraoperative data.Table 3. Biochemical and radiological data.Table 4. Complications.Table 5. Pre- and post-splenic artery ligation data.
Table 5. Pre- and post-splenic artery ligation data.Table 1. Demographic and clinical sata.Table 2. Intraoperative data.Table 3. Biochemical and radiological data.Table 4. Complications.Table 5. Pre- and post-splenic artery ligation data. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988