20 October 2020: Review Paper
Clinical Relevance of Kidney Biopsy in Patients Qualified for Liver Transplantation and After This Procedure in the Model for End-stage Liver Disease (MELD) Era: Where Are We Today?
Monika Wieliczko1ABCDEF, Urszula Ołdakowska-Jedynak1BCEF, Jolanta Małyszko1ABCDEFG*DOI: 10.12659/AOT.925891
Ann Transplant 2020; 25:e925891






Abstract
ABSTRACT: Chronic kidney disease (CKD) has been recognized as an increasingly common complication of liver transplantation (OLTx). Post-transplant renal dysfunction contributes to long-term morbidity and mortality following OLTx and is a very important issue in the management of liver transplant recipients. Its etiology is multifactorial and can be determined by kidney biopsy, which is too rarely done in this patient group. In the clinical context of patients with liver cirrhosis, accurate and reliable evaluation of the renal injury is crucial. We performed a review of kidney biopsies in patients with symptoms of CKD (proteinuria/hematuria/elevated creatinine) before and after liver transplantation in the published literature. Kidney biopsies were performed either before or after liver transplantation using percutaneous technique. There are few reports on transjugular kidney biopsy. Biopsy results prevented unnecessary modification of immunosuppressive therapy or selection of candidates for liver transplantation. In our opinion, kidney biopsy is a clinically relevant diagnostic approach to recognize kidney disease before and after liver transplantation, it also helps with the management of kidney disease in this population, and it is safe. Kidney biopsy should be offered more often in liver transplant patients to ensure appropriate therapy in concomitant CKD in this population. Our decisions today will impact clinical outcomes in the future.
Keywords: Biopsy, Liver Transplantation, Renal Insufficiency, Chronic, End stage liver disease, Kidney, Severity of Illness Index
Background
Chronic kidney disease (CKD) is the most common kidney problem in the general population, and, in advanced stages, patients need dialysis treatment. CKD is also a huge problem in special patient groups, such as patients with end-stage liver disease (ESLD).
The number of patients with concomitant renal dysfunction qualified for liver transplantation (OLTx) and after this procedure has recently further increased due to the implementation of MELD (Model for End-stage Liver Disease) score-based allograft allocation. About 30–80% of patients develop CKD, with a cumulative risk of ESRD (End-Stage Renal Disease) requiring renal replacement therapy consisting of either maintenance dialysis or renal transplantation [1,2]. Although chronic kidney disease (CKD) is a common problem in these patients, kidney biopsy is rarely performed because of its invasive nature and potential complications, and therapeutic decisions are made solely on the basis of biochemical tests. There is no criterion standard diagnostic assessment used in most transplant centers, and data on histological changes and complications in patients with CKD in ESLD patients are scarce. The prevalence of CKD in patients qualified to OLTx and after this procedure has not been precisely defined, but it is known to affect the long-term results of liver transplant recipients. Several large studies have shown that pretransplant CKD in patients with a stage higher than 1 (especially with elevated creatinine), presence of hepatorenal syndrome before transplantation, or requirement of renal replacement therapy early after transplantation have an increased risk of post-transplant ESRD [3–6]. Chronic renal dysfunction has also been shown to have a significant association with cardiovascular events in clinical analyses [7]. These findings confirm retrospective evidence that the risk of major cardiac events increases with deteriorating renal function in liver recipients. At present, the decision is made on a case-by-case basis and there is no guideline regarding the role of renal biopsy in the setting of kidney injury in liver transplant patients [8].
We conducted a literature review of kidney biopsy performed in patients before and after liver transplantation, including percutaneous and transjugular procedures. We performed a search in Medline, PubMed, and Embase using the keywords: kidney biopsy, kidney impairment, kidney failure, CKD, liver transplantation, ESLD, and liver cirrhosis. We limited our search to adult patients and publications in English and Polish between 1995 and 2020. We found 2306 articles, but only 23 articles were analyzed due to lack of information about histological changes in kidneys, lack of full clinical data, and availability of abstracts only.
Pretransplant Kidney Biopsy and OLTx
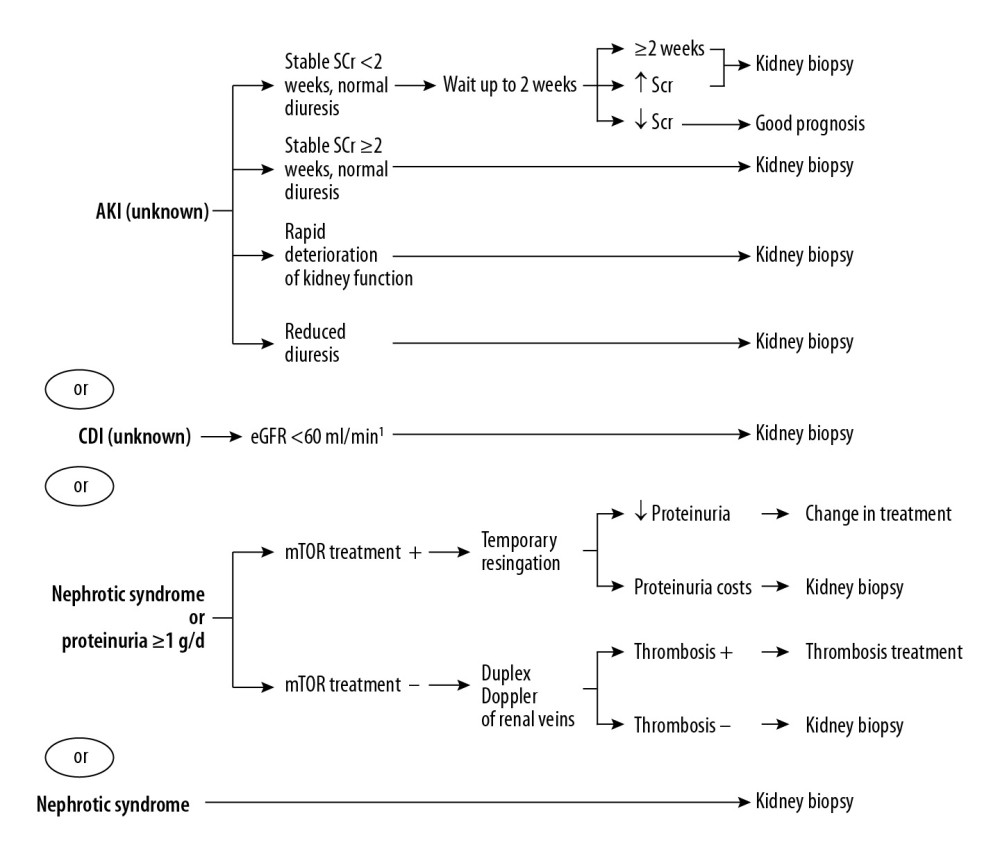
Assessment of kidney function before liver transplantation is important because the presence of impaired kidney function before transplantation, particularly the presence of hepatorenal syndrome, is a significant predictor of post-transplant CKD or even requirement for renal replacement therapy [9,10]. Approximately 25% of patients qualified for OLTx have some renal function damage. Cirrhotic patients have specific disturbances that affect the serum creatinine value; therefore, this endogenous marker remains an imperfect parameter of renal function in this clinical setting [11]. In patients with glomerulonephritis, it is particularly important in regard to treatment and outcome, especially when there is co-existing hepatitis B and/or C [12]. Published studies have not established the correlation between kidney disease progression after transplantation and renal histological damage, kidney function, or clinical picture [12–14]. The role of pretransplant kidney biopsy in liver transplant candidates has not been established. Kidney biopsy findings are not included in the 2016 OPTN/UNOS criteria for selection of patients for simultaneous liver-kidney transplantation [15,16], although only kidney biopsy can differentiate the type and severity of kidney injury and provide information about reversibility or irreversibility of renal damage (excluding obvious cases like cystic disease or atrophy). A pre-liver transplant kidney biopsy can help make the decision and establish the cause of kidney disease. In addition, kidney biopsy can be helpful to determine chronicity, treatability, and likelihood of future progression or reversibility. A few published studies on pretransplant kidney biopsy and evaluation for potential simultaneous liver-kidney transplantation suggest performing dual transplantation in a case of glomerulosclerosis exceeding 40% and interstitial fibrosis exceeding 30% [5,6,17], but these studies are limited by the small number of biopsies performed. However, a study reported avoidance of dual transplantation in 70% of patients on the basis of biopsy [6]. In these patients, the extent of glomerulosclerosis was a predictor of eGFR reduction over the first 12 months after liver transplantation [6]. Wadei et al. [18] reported that 22% of liver transplant recipients with pretransplant kidney biopsies showing reversible histology were evaluated for kidney transplantation by 12 months after liver transplant [18]. Therefore, more studies are needed to determine whether pretransplant kidney biopsies can predict long-term kidney outcomes after liver transplantation. A summary of studies on pretransplant kidney biopsy with clinical relevance is presented in Table 1.
Post-Transplant Kidney Biopsy and OLTx
The etiology of CKD after liver transplantation may be multifactorial. The disease may result from treatment (e.g., early renal dysfunction after LT has been associated with the use of the calcineurin inhibitors [CNI] approved to prevent liver graft rejection in all immunosuppression regimens), with complications after transplantation (e.g., post-transplant diabetes or hypertension), may appear
Conclusions
Kidney biopsy is very useful in diagnosing kidney damage and assessing prognosis in liver transplant recipients. The procedure is safe, but is rarely performed. The data on pre- and post-transplant kidney biopsy are very scarce. Kidney damage occurring in approximately 25% of patients qualified for OLTx is often irreversible, and predicting renal recovery after OLTx, without knowledge of histological changes in the kidneys, is imperfect and challenging. In some studies, the incidence of kidney biopsies was about 1–2% [32]. It would be helpful to know if a patient has a chance to improve kidney function after OLTx or should be qualified for simultaneous transplantation (SLKT). On the other hand, immunosuppressive treatment after OLTx with a CNI reduction can improve kidney function, but studies show that CNI toxicity accounts for only a small percentage of complications. Performing a kidney biopsy in such a situation may reduce unnecessary discontinuation of immunosuppression. We suggest that kidney biopsy in patients qualified for OLTx and after transplantation should be done more often, as it can help in the treatment and prognosis of CKD in this vulnerable population.
References
1. Ojo AO, Held PhJ, Port FK, Chronic renal failure after transplantation of a nonrenal organ: N Engl J Med, 2003; 349; 931-40
2. Gonwa TA, Mai ML, Melton LB, End-stage renal disease (ESRD) after orthotopic liver transplantation (OLTX) using calcineurin-based immunotherapy: Risk of development and treatment: Transplantation, 2001; 72; 1934-39
3. Malyszko J, Durlik M, Przybylowski P, Kidney dysfunction after non-renal solid organ transplantation: Ann Transplant, 2009; 14; 71-79
4. Gonwa TA, McBride MA, Anderson K, Continued influence of preoperative renal function on outcome of orthotropic liver transplant (OLTX) in the US: Where will MELD lead us?: Am J Transplant, 2006; 6; 2651-59
5. Davis CI, Feng S, Sung R, Simultaneous liver-kidney transplantation: evaluation to decision making: Am K Transplant, 2007; 7; 1702-9
6. Pichler RH, Husky J, Kowalewska J, Kidney biopsies may help predict renal function after liver transplantation: Transplantation, 2016; 100; 2122-28
7. Saliba F, Fischer L, de Simone P, Association between renal dysfunction and major adverse cardiac events after liver transplantation: evidence from an international randomized trial of everolimus-based immunosuppression [published correction appears in Ann Transplant, 2019; 24: 174]: Ann Transplant, 2018; 23; 751-57
8. Duvoux C, Pageaux GP, Immunosuppression in liver transplant recipients with renal impairment: J Hepatol, 2011; 54(5); 1041-54
9. Srinivas TR, Stephany BR, Budev M, An emerging population: kidney transplant candidates who are placed on the waiting list after liver, heart, and lung transplantation: Clin J Am Soc Nephrol, 2010; 5; 1881-86
10. O’Riordan A, Wong V, McCormick PA, Chronic kidney disease post-liver transplantation: Nephrol Dial Transplant, 2006; 21; 2630
11. Sherman DS, Fish DN, Teitelbaum I, Assessing renal function in cirrhotic patients problems and pitfalls: Am J Kidney Dis, 2003; 41; 269-78
12. McGuire BM, Julian BA, Bynon JS, Brief communication: Glomerulonephritis in patients with hepatitis C cirrhosis undergoing liver transplantation: Ann Intern Med, 2006; 144; 735-41
13. Labban B, Arora N, Restaino S, The role of kidney biopsy in heart transplant candidates with kidney disease: Transplantation, 2010; 89; 887-93
14. Wadei HM, Geiger XJ, Cortese C, Kidney allocation to liver transplant candidates with renal failure of undetermined etiology: Role of percutaneous renal biopsy: Am J Transplant, 2008; 8; 2618-26
15. Pham PT, Pham PC, Rastogi A, Wilkinson AH, Review article: Current management of renal dysfunction in the cirrhotic patient: Aliment Pharmacol Ther, 2005; 21; 949-61
16. Formica RN, Aeder M, Boyle G, Simultaneous liver-kidney allocation policy: A proposal to optimize appropriate utilization of scarce resources: Am J Transplant, 2016; 16; 758-66
17. Davis CL, Feng S, Sung R, Simultaneous liver-kidney transplantation: Evaluation to decision making: Am J Transplant, 2007; 7; 1702-9
18. Wadei HM, Heckman MG, Rawal B, Renal outcome of liver transplant recipients who had pretransplant kidney biopsy: Transplantation, 2014; 98; 1323-30
19. Ziolkowski J, Paczek L, Senatorski G, Renal function after liver transplantation: Calcineurin inhibitor nephrotoxicity: Transpl Proc, 2003; 35; 2307-9
20. Axelsen RA, Crawford DH, Endre ZH, Renal glomerular lesions in unselected patients with cirrhosis undergoing orthotopic liver transplantation: Pathology, 1995; 27; 237-46
21. Whittier WL, Korbet S, Timing of complications in percutaneous renal biopsy: J Am Soc Nephrol, 2004; 15; 142-47
22. Jouet P, Meyrier A, Mai F, Transjugular renal biopsy in the treatment of patients with cirrhosis and renal abnormalities: Hepatology, 1996; 24; 1143-47
23. Sam R, Leehey DJ, Picken MM, Transjugular renal biopsy in patients with liver disease: Am J Kidney Dis, 2001; 37; 1144-51
24. Allen AM, Kim WR, Therneau TM, Chronic kidney disease and associated mortality after liver transplantation – a time-dependent analysis using measured glomerular filtration rate: J Hepatol, 2014; 61; 286-92
25. Moreno MJ, Cuervas-Mons V, Rubio E, Chronic renal dysfunction after liver transplantation in adult patients: Prevalence, risk factors, and impact on mortality: Transplant Proc, 2003; 35; 1907-8
26. Fujinaga K, Usui M, Yamamoto N, Hypertension and hepatitis C virus infection are strong risk factors for developing late renal dysfunction after liver living donor liver transplantation: Significance of renal biopsy: Transplant Proc, 2014; 46; 804-10
27. Lee JH, Cho YH, Ryu SJ, Clinical usefulness of kidney biopsy in liver transplant recipients with renal impairment: Kidney Res Clin Pract, 2013; 32; 153-57
28. Pillebout E, Nochy D, Hill G, Renal histopathological lesions after orthotropic liver transplantation (OLT): Am J Transpl, 2005; 5; 1120-29
29. Wieliczko M, Ołdakowska-Jedynak U, Andrian T, Małyszko J, Kidney biopsy in patients after liver transplantation: An underutilized, but clinically important procedure: Int Urol Nephrol, 2020; 52; 1191-92
30. Abbott KC, Musi FM, Chung EM, Transjugular renal biopsy in high-risk patients: An American case series: BMC Nephrol, 2002; 3; 5
31. Welker MW, Weiler N, Bechstein WO, Key role of renal biopsy in management of progressive chronic kidney disease in liver graft recipients: J Nephrol, 2019; 32; 129-37
32. Tsapenko M, El-Zoghby ZM, Sethi S, Renal histological lesions and outcome in liver transplant recipients: Clin Transplant, 2012; 26; E48-54
33. Neau-Cransac M, Morel D, Bernard P-H, Renal failure after liver transplantation. Outcome after calcineurin inhibitor withdrawal: Clin Transplant, 2002; 16; 368-73
34. Kim J-Y, Akalin E, Dikman S, The variable pathology of kidney disease after liver transplantation: Transplantation, 2010; 89; 215-21
35. Kamar N, Maaroufi C, Guilbeau-Frugier C, Do kidney histology lesions predict long-term kidney function after liver transplantation?: Clin Transplant, 2012; 26; 927-34
36. Kubal Ch, Cockwell P, Gunson B, Chronic kidney disease after nonrenal solid organ transplantation: A histological assessment and utility of chronic allograft damage index scoring: Transplantation, 2012; 93; 406-11
37. Chan GSW, Lam MF, Kwan L, Clinicopathological study of renal biopsies after liver transplantation: Hong Kong Med J, 2013; 19; 27-32
38. Calmus Y, Conti F, Cluzel Ph, Prospective assessment of renal histopathological lesions in patients with end-stage liver disease; Effects on long-term renal function after liver transplantation: J Hepatol, 2012; 57; 572-76
39. Lee JP, Heo NJ, Joo KW, Risk factors for consequent kidney impairment and differential impact of liver transplantation on renal function: Nephrol Dial Transplant, 2010; 25; 2772-85
40. Schwarz A, Haller H, Schmitt R, Biopsy-diagnosed renal disease in patient after transplantation of other organs and tissue: Amer J Transplant, 2010; 10; 2017-25
41. Singh N, Ahmadzadeh S, Shokouh-Amiri H, Kidney outcomes in patients with liver cirrhosis and chronic kidney disease receiving liver transplant alone: Clin Transplant, 2017; 31; ctr13008
42. Hiesse C, Samuel D, Bensadoun H, Combined liver and kidney transplantation in patients with chronic nephritis associated with end-stage liver disease: Nephrol Dial Transplant, 1995; 10(Supp 6); 129-33
43. Wadei HM, Abader P, Alsaad AA, Arterial blood pressure at liver transplant evaluation predict renal histology in candidates with renal dysfunction: Liver Transplantation, 2019; 25; 1756-67
Tables
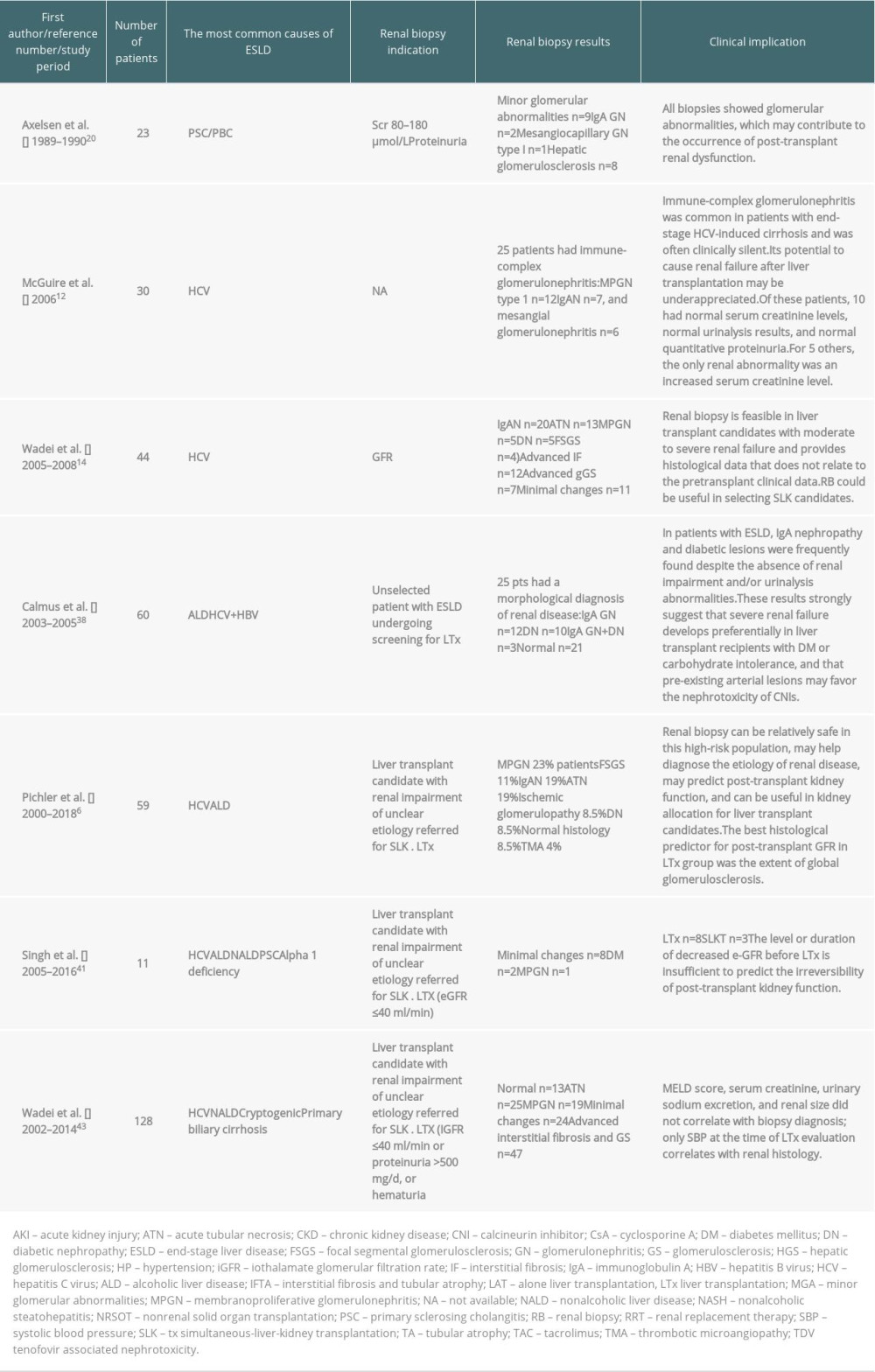 Table 1. Kidney biopsy before liver transplantation.
Table 1. Kidney biopsy before liver transplantation.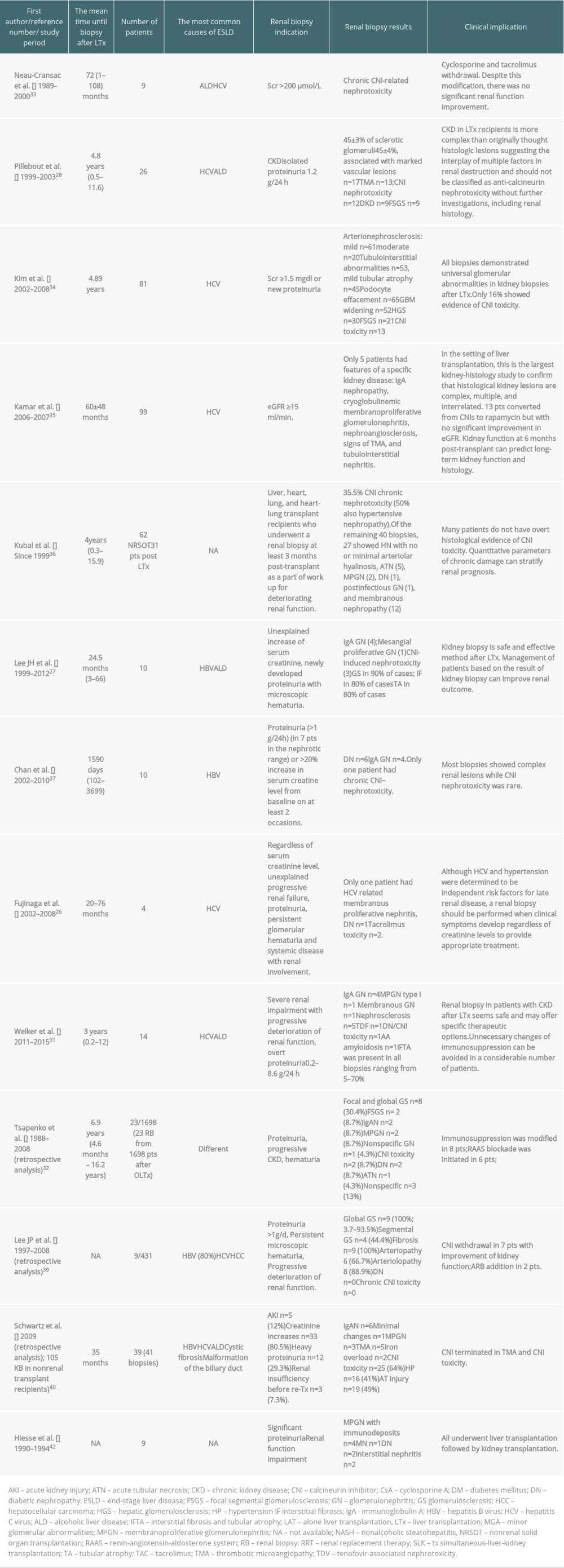 Table 2. Kidney biopsy after liver transplantation.
Table 2. Kidney biopsy after liver transplantation.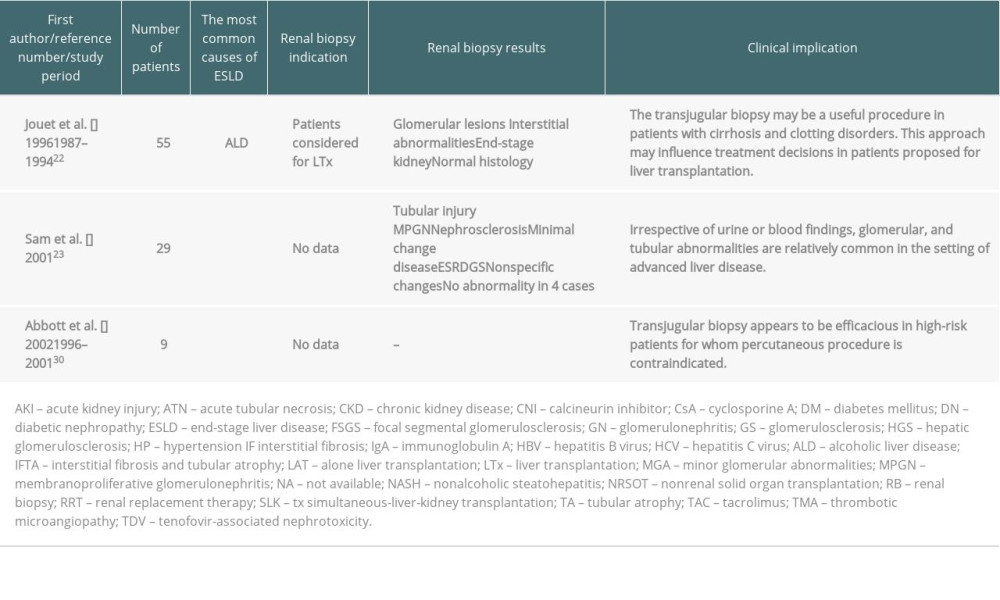 Table 3. Transjugular kidney biopsy in liver transplant recipients.Table 1. Kidney biopsy before liver transplantation.Table 2. Kidney biopsy after liver transplantation.Table 3. Transjugular kidney biopsy in liver transplant recipients.
Table 3. Transjugular kidney biopsy in liver transplant recipients.Table 1. Kidney biopsy before liver transplantation.Table 2. Kidney biopsy after liver transplantation.Table 3. Transjugular kidney biopsy in liver transplant recipients. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988