06 April 2021: Original Paper
Intensified Endoscopic Evaluation for Biliary Complications After Orthotopic Liver Transplantation
Tim R. Glowka1ABCDEF*, Caroline Karlstetter1BCF, Tobias J. Weismüller2BCD, Tim O. Vilz1CD, Christian P. Strassburg2CD, Jörg C. Kalff1CD, Steffen Manekeller1ACDEFDOI: 10.12659/AOT.928907
Ann Transplant 2021; 26:e928907






Abstract
BACKGROUND: Biliary complications are common causes of morbidity and mortality after liver transplantation.
MATERIAL AND METHODS: From 2013 to 2018, 102 whole-organ liver transplantations were conducted in our department. Patients were closely monitored for biliary complication development. In all suspected cases, patients underwent either endoscopic retrograde cholangiopancreatography or percutaneous transhepatic cholangial drainage. Patients’ demographic characteristics, preexisting conditions, and perioperative characteristics, as well as morbidity and mortality, were analyzed. Risk factors for 1-year survival were calculated.
RESULTS: Of the 102 patients, 43 (42%) experienced biliary complications. In comparison with patients without biliary complications, patients with biliary complications exhibited the following risk factors: underlying liver disease (viral hepatitis; P=0.009), blood group A (P=0.005), and previous abdominal surgery (P=0.037). Neither perioperative characteristics, especially duration of cold ischemia (P=0.86), nor postoperative course differed between patients with and without biliary complications. Risk factors for mortality within 1 year were cirrhosis caused by entities other than viral hepatitis (P=0.017), cardiac comorbidities (P=0.019), re-transplantation (P=0.032), and reduced organ weight (P=0.002). Biliary complications, postoperative hemorrhage, primary nonfunction, and repeated surgery worsened outcome; moreover, serum bilirubin trough in the first 30 days after transplantation might be prognostic for mortality (P=0.043).
CONCLUSIONS: Biliary complications adversely affect outcome after liver transplantation. Neither frequency nor outcome of biliary complications was improved by intensified endoscopic evaluation. Patients on the waiting list for liver transplants should also be closely monitored for cardiac comorbidities.
Keywords: Anastomotic Leak, Biliary Fistula, Biliary Tract, endoscopy, Liver Cirrhosis, Liver Transplantation, Biliary Tract Diseases, Cholangiopancreatography, Endoscopic Retrograde, Drainage, Female, Humans, Liver Diseases, Male, Middle Aged, Postoperative Complications, Retrospective Studies
Background
Liver transplantation (LTx) is the main therapy for end-stage liver disease. The 1-year survival rate is excellent (~90%), according to European and United States registries [1,2]. Biliary complications (BCs) commonly cause morbidity, graft loss, and even mortality in transplant recipients [3]. Early in the history of LTx, morbidity and mortality rates (34–50% and 24–30%, respectively) from BCs were high [4,5]. Although those rates have decreased over the last decades, 10–30% of BCs still result in morbidity [6–8]. In recent years, a renewed rise in BCs has been noted, possibly as a result of the increased use of marginal organs [3,9]. The discovery and media coverage of compliance violations in several transplantation centers has significantly reduced the willingness to donate organs after brain death in Germany. In 2010, 1271 donations were registered; this number dropped to 769 in 2017. Although national guidelines have been adapted since 2017 and intense audits of transplant centers have been conducted, the number of donations has not yet recovered (899 in 2019; annual reports at www.eurotransplant.org). Because 80% of the donated livers are nationally allocated in the Eurotransplant area (of the 1571 donated livers, 1264 were nationally allocated in total, according to the 2019 annual report), marginal organs have been increasingly accepted for transplantation, with a simultaneous increase of BC in our personal experience.
BCs after LTx are various problems arising from the intrahepatic or extrahepatic bile ducts or the papillary region. Bile leaks mainly occur at the anastomosis, with a reported incidence of 1–25% [8,10]. Risk factors for bile leaks include partial graft transplantations, hepaticojejunostomy, insufficient surgical technique, and ischemia; t-tube use remains under debate [8,10]. Anastomotic strictures (Figures 1, 2) occur within 1 cm of the surgical anastomosis, with an incidence of 1–18% [6,8]. Risk factors for anastomotic strictures are postoperative bile leaks, sex mismatch, prolonged duration of warm and cold ischemia, insufficient surgical technique, ischemia, and hepaticojejunostomy anastomosis and partial graft use [6,8,10]. Nonanastomotic strictures (NASs; Figure 3) arise outside the anastomotic region and are regarded the most challenging BC [8,11]. Because of different definitions and various manifestations, the reported incidence ranges widely (between 1% and 20%) [6,7,10]. The presumed causes of NASs are ischemia, ABO incompatibility, chronic rejection, recurrent primary sclerosing cholangitis, older donor age, and, especially, organ quality [6,10].
The onset time of BCs differs for leaks and anastomotic/nonanastomotic strictures; most BCs occur during the first year after transplantation [10]. Diagnosis is mainly accomplished with imaging. Abdominal ultrasonography is not reliable for the diagnosis of biliary obstruction, but in combination with Doppler examination, it is crucial for ruling out hepatic artery occlusion [6,11,12]. Both biliary leakage and strictures can be diagnosed with endoscopic retrograde cholangiopancreatography (ERCP) or magnetic resonance cholangiopancreatography (MRCP), both of which have high sensitivity and specificity (>90%) [8,10,11]. MRCP is noninvasive, but its availability might be limited. ERCP has the advantage of combining diagnostic and therapeutic measures in the same session [6]. Because contrast media can be injected into the bile ducts with pressure, even small insufficiencies that might be missed with MRCP can be detected on ERCP. If Roux-en-Y reconstruction has been performed, percutaneous cholangiography might be indicated [8,10]. Liver biopsy is helpful for diagnosing other causes of graft dysfunction, such as rejection, recurrent hepatitis C virus infection, or cytomegalovirus-induced hepatitis [10,13].
We hypothesized that obligatory evaluation of BCs with ERCP after LTx and early treatment can help improve morbidity and mortality rates. All cases of BCs that were suspected on the basis of results of isolated cholestatic liver tests, bilious secretion into the drains, and severe graft dysfunction without other suspected causes during the study period were therefore evaluated by ERCP.
Material and Methods
STATISTICAL ANALYSIS:
All patient data were prospectively recorded and anonymously stored in our liver transplant database in an Excel file (Microsoft Corporation, Redmond, WA, USA). For this study, SPSS 24 (IBM Corporation, Armonk, NY, USA) was used to retrospectively analyze the data. Continuous and normally distributed variables were analyzed with the
Results
Between 2013 and 2018, LTx with whole-liver grafts was performed in 102 patients. Of these, 43 experienced some degree of BCs. Mild forms included cholestasis, detected in laboratory tests, without symptoms. Every form of bilious secretion indicated BCs. In severe cases, parenchymal decompensation occurred as a result of biliary strictures. In uncertain cases, liver biopsy was performed. In 41 patients, ERCP was successful. In 2 patients, ERCP could not be conducted because of Roux-en-Y reconstruction, and percutaneous transhepatic cholangial drainage was performed. The first ERCP was conducted on a median of postoperative day 56. In 2 patients, no biliary problem could be detected; all others were diagnosed with either bile leaks, anastomotic, or nonanastomotic strictures. More than 1 ERCP was needed in 78% of the patients. In patients with anastomotic strictures, the success rate of endoscopic treatment was 72%. Nonanastomotic strictures were treated successfully in only 24% of cases, with many patients still under recurrent endoscopic treatment at the end of follow-up.
Patients’ demographic characteristics are listed in Table 1. Most patients with BCs had not undergone transplantation for viral hepatitis (
The overall 1-year mortality rate was 12.7% and the 3-year mortality rate was 17.6%. Table 4 lists significant risk factors for 1-year mortality. No patients with viral hepatitis died during the first postoperative year (
Discussion
Since the early days of LTx, the bile duct has been called the “Achilles heel” of this procedure [4,5]. BCs represent important risk factors for morbidity, graft loss, and even mortality. In particular, NAS are challenging to treat. Graft loss rate of up to 46% in the first 2 postoperative years and a mortality rate of 22.2% among patients with NAS have been reported [14]. Patients with the worst prognosis seem to be those in whom NAS occurs during the first year after transplantation [11,15]. Therefore, all transplant recipients were intensively monitored for BC and underwent ERCP. Bile leaks can be interventionally treated; success rates are 85–100% [6,10]. For anastomotic strictures, ERCP treatment yields success rates of 70–90% [8,11,12], and even NAS can be successfully treated in 50–75% of cases [6,8,12]. With this intensified endoscopic diagnostic regimen, we diagnosed BCs in 42% of our patients after LTx. This percentage is higher than those reported previously [6–8], but this finding can be explained by several factors: ERCP was undertaken at the slightest suspicion of BC, even mild cholestasis detected in laboratory tests prompted invasive diagnostic measures, and perhaps these BCs would not have been diagnosed under normal circumstances. After introduction of the Model for End-Stage Liver Disease organ allocation system, the incidence of BCs after LTx increased [9,16]; this is attributable to the reduced quality of donor organs. In our experience, the shortage of liver grafts in Germany has clearly necessitated the increased use of marginal organs. Other transplant centers have also observed a rise in BCs in recent years [16]. Apart from poorer organ quality, the rising frequency of BCs can be explained by an increased awareness of the signs of BCs in transplant centers and by the improvement in diagnostic modalities [3].
Some risk factors for the development of BCs could not be confirmed in our study. Primary sclerosing cholangitis was described by other investigators as a risk factor [14,17]. Of our patients, 14% underwent transplantation for this indication, but we found no difference in the incidence of BCs between these patients and others. Hepatic artery thrombosis is an important risk factor [18]; a total of 21 vascular reconstructions had to be performed during LTx among our patients. Although these reconstructions were more frequently performed in patients without BCs (24%) than in those with BCs (16%), occlusion of the hepatic artery was more common in those with BCs (7%) than in those without (2%;
BCs were a risk factor for mortality within 1 year after LTx in our cohort (69% of patients with BCs vs 38% of those without;
Preexisting cardiac comorbidity was another significant risk factor for 1-year mortality, with an odds ratio of 4.556 (
Conclusions
The incidence of BCs after LTx is even higher than previously reported. At our institution, every case of suspected BCs is checked with endoscopic- or radiologically-guided intervention. This is of utmost importance because BCs represent a significant risk factor for posttransplantation morbidity and mortality. An intensified focus on cardiac comorbidity is needed for patients on the waiting list for LTx.
Figures
 Figure 1. Anastomotic stricture (arrow) visualized via endoscopic retrograde cholangiopancreatography (ERCP).
Figure 1. Anastomotic stricture (arrow) visualized via endoscopic retrograde cholangiopancreatography (ERCP).  Figure 2. Same patient as in Figure 1. After dilatation and stent placement.
Figure 2. Same patient as in Figure 1. After dilatation and stent placement.  Figure 3. Nonanastomotic strictures (arrows) visualized via endoscopic retrograde cholangiopancreatography (ERCP).
Figure 3. Nonanastomotic strictures (arrows) visualized via endoscopic retrograde cholangiopancreatography (ERCP). References
1. Merion RM, Schaubel DE, Dykstra DM, The survival benefit of liver transplantation: Am J Transplant, 2005; 5(2); 307-13
2. Charlton MR, Roadmap for improving patient and graft survival in the next 10 years: Liver Transpl, 2016; 22(S1); 71-78
3. Verdonk RC, Buis CI, Porte RJ, Anastomotic biliary strictures after liver transplantation: Causes and consequences: Liver Transpl, 2006; 12(5); 726-35
4. Starzl TE, Putnam CW, Hansbrough JF, Biliary complications after liver transplantation: With special reference to the biliary cast syndrome and techniques of secondary duct repair: Surgery, 1977; 81(2); 212-21
5. Calne RY, McMaster P, Portmann B, Observations on preservation, bile drainage and rejection in 64 human orthotopic liver allografts: Ann Surg, 1977; 186(3); 282-90
6. Verdonk RC, Buis CI, Porte RJ, Biliary complications after liver transplantation: A review: Scand J Gastroenterol Suppl, 2006; 243; 89-101
7. Wojcicki M, Milkiewicz P, Silva M, Biliary tract complications after liver transplantation: A review: Dig Surg, 2008; 25(4); 245-57
8. Roos FJM, Poley J-W, Polak WG, Biliary complications after liver transplantation; Recent developments in etiology, diagnosis and endoscopic treatment: Best Pract Res Clin Gastroenterol, 2017; 31(2); 227-35
9. Sundaram V, Jones DT, Shah NH, Posttransplant biliary complications in the pre- and post-model for end-stageliver disease era: Liver Transpl, 2011; 17(4); 428-35
10. Seehofer D, Eurich D, Veltzke-Schlieker W, Biliary complications after liver transplantation: old problems and new challenges: Am J Transplant, 2013; 13(2); 253-65
11. Larghi A, Tringali A, Rimbaş M, Endoscopic management of benign biliary strictures after liver transplantation: Liver Transpl, 2019; 25(2); 323-35
12. Sharma S, Gurakar A, Jabbour N, Biliary strictures following liver transplantation: Past, present and preventive strategies: Liver Transpl, 2008; 14(6); 759-69
13. Gopal DV, Pfau PR, Lucey MR, Endoscopic management of biliary complications after orthotopic liver transplantation: Curr Treat Options Gastroenterol, 2003; 6(6); 509-15
14. Guichelaar MMJ, Benson JT, Malinchoc M, Risk factors for and clinical course of non-anastomotic biliary strictures after liver transplantation: Am J Transplant, 2003; 3(7); 885-90
15. Verdonk RC, Buis CI, van der Jagt EJ, Nonanastomotic biliary strictures after liver transplantation, part 2: Management, outcome, and risk factors for disease progression: Liver Transpl, 2007; 13(5); 725-32
16. Kaltenborn A, Gutcke A, Gwiasda J, Biliary complications following liver transplantation: Single-center experience over three decades and recent risk factors: World J Hepatol, 2017; 9(3); 147-54
17. Sankary HN, McChesney L, Frye E, A simple modification in operative technique can reduce the incidence of nonanastomotic biliary strictures after orthotopic liver transplantation: Hepatology, 1995; 21(1); 63-69
18. Stange BJ, Glanemann M, Nuessler NC, Hepatic artery thrombosis after adult liver transplantation: Liver Transpl, 2003; 9(6); 612-20
19. Buis CI, Verdonk RC, Van der Jagt EJ, Nonanastomotic biliary strictures after liver transplantation, part 1: Radiological features and risk factors for early vs. late presentation: Liver Transpl, 2007; 13(5); 708-18
20. Thethy S, Thomson BN, Pleass H, Management of biliary tract complications after orthotopic liver transplantation: Clin Transplant, 2004; 18(6); 647-53
21. Heidenhain C, Pratschke J, Puhl G, Incidence of and risk factors for ischemic-type biliary lesions following orthotopic liver transplantation: Transpl Int, 2010; 23(1); 14-22
22. Sanchez-Urdazpal L, Gores GJ, Ward EM, Ischemic-type biliary complications after orthotopic liver transplantation: Hepatology, 1992; 16(1); 49-53
23. Iacob S, Cicinnati VR, Dechêne A, Genetic, immunological and clinical risk factors for biliary strictures following liver transplantation: Liver Int, 2012; 32(8); 1253-61
24. Mehrabi A, Mood ZA, Fonouni H, A single-center experience of 500 liver transplants using the modified piggyback technique by Belghiti: Liver Transpl, 2009; 15(5); 466-74
25. Rull R, Garcia Valdecasas JC, Grande L, Intrahepatic biliary lesions after orthotopic liver transplantation: Transpl Int, 2001; 14(3); 129-34
26. Sanchez-Urdazpal L, Batts KP, Gores GJ, Increased bile duct complications in liver transplantation across the ABO barrier: Ann Surg, 1993; 218(2); 152-58
27. Li X, Xu H, Gao P, ABO blood group and diabetes mellitus influence the risk for pancreatic cancer in a population from China: Med Sci Monit, 2018; 24; 9392-98
28. Baudouy D, Moceri P, Chiche O, B blood group: A strong risk factor for venous thromboembolism recurrence: Thromb Res, 2015; 136(1); 107-11
29. Adam R, McMaster P, O’Grady JG, Evolution of liver transplantation in Europe: Report of the European Liver Transplant Registry: Liver Transpl, 2003; 9(12); 1231-43
30. Yoshizumi T, Taketomi A, Kayashima H, Estimation of standard liver volume for Japanese adults: Transplant Proc, 2008; 40(5); 1456-60
31. Heinemann A, Wischhusen F, Püschel K, Standard liver volume in the Caucasian population: Liver Transpl Surg, 1999; 5(5); 366-68
32. Tiukinhoy-Laing SD, Rossi JS, Bayram M, Cardiac hemodynamic and coronary angiographic characteristics of patients being evaluated for liver transplantation: Am J Cardiol, 2006; 98(2); 178-81
33. Neal DAJ, Tom BDM, Luan J, Is there disparity between risk and incidence of cardiovascular disease after liver transplant?: Transplantation, 2004; 77(1); 93-99
34. Johnston SD, Morris JK, Cramb R, Cardiovascular morbidity and mortality after orthotopic liver transplantation: Transplantation, 2002; 73(6); 901-6
Figures
Tables
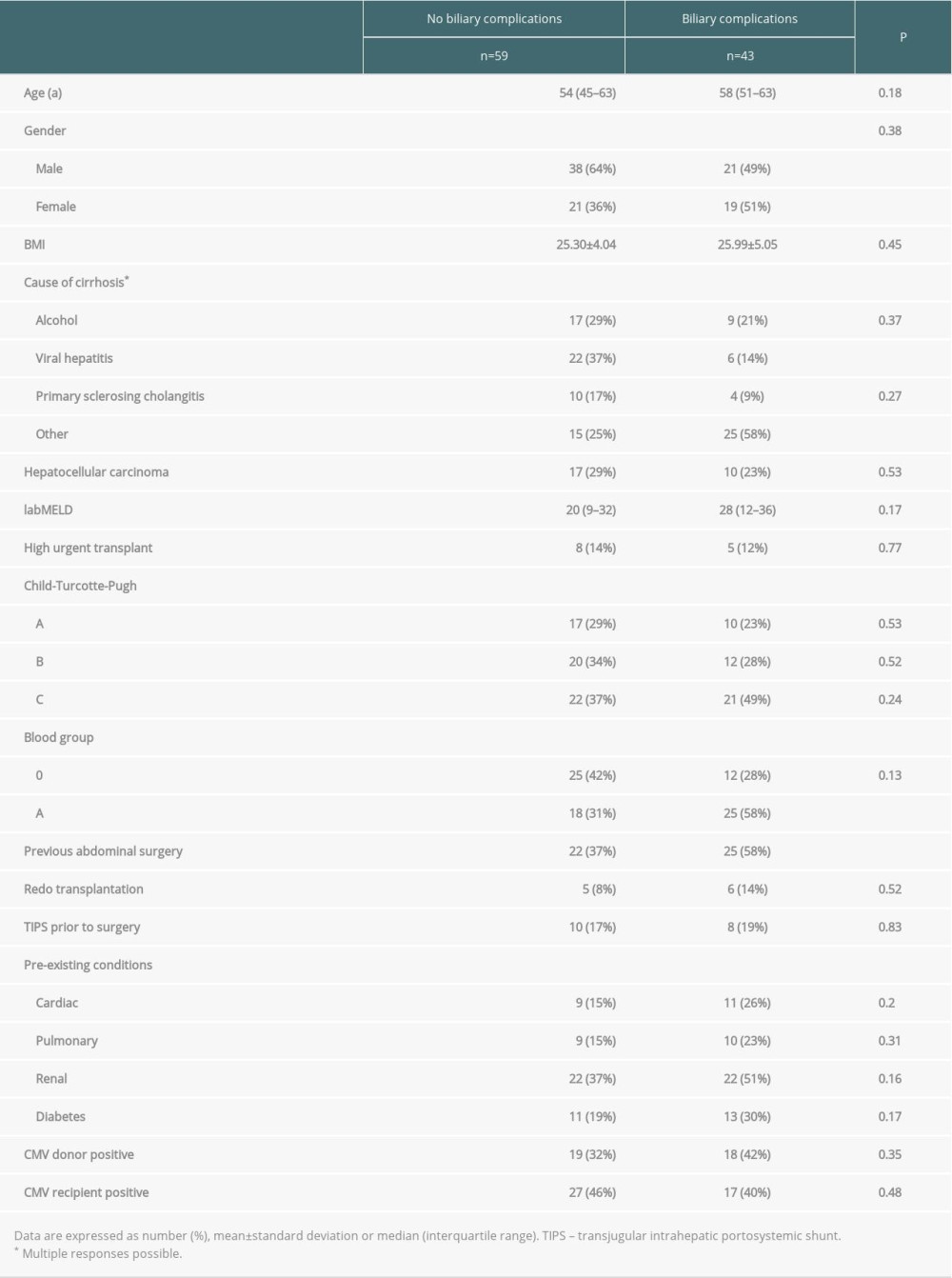 Table 1. Demographics.
Table 1. Demographics.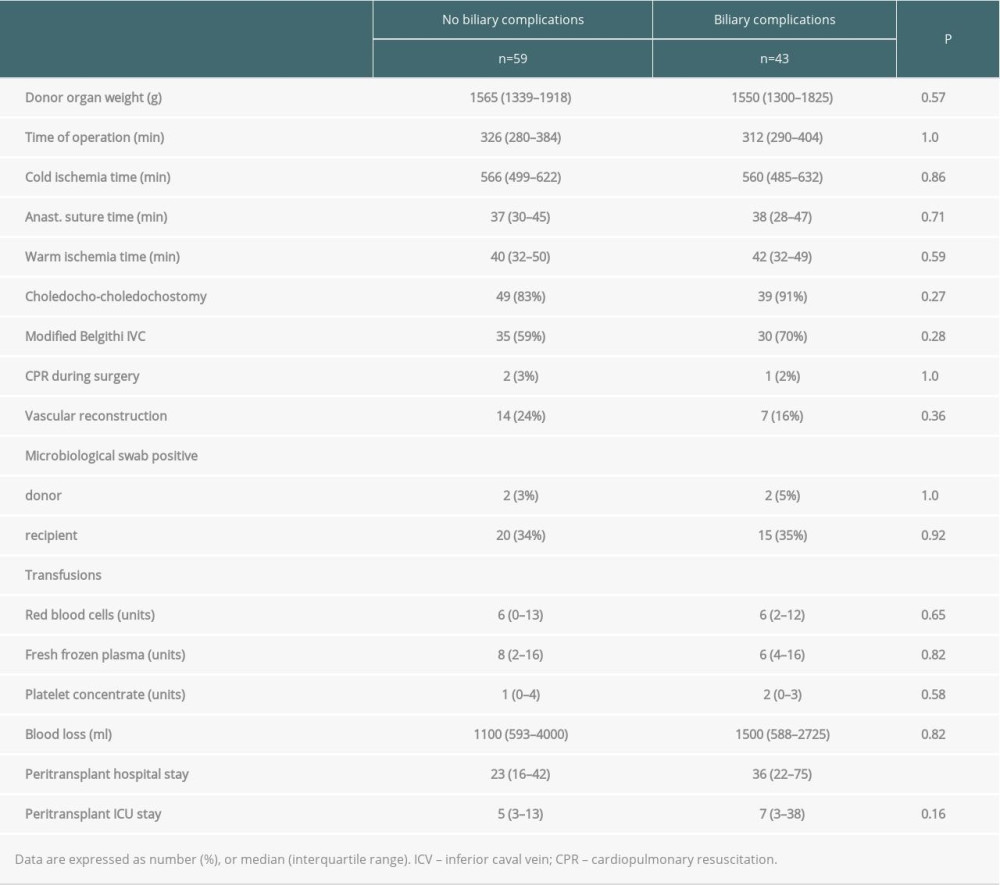 Table 2. Perioperative characteristics.
Table 2. Perioperative characteristics.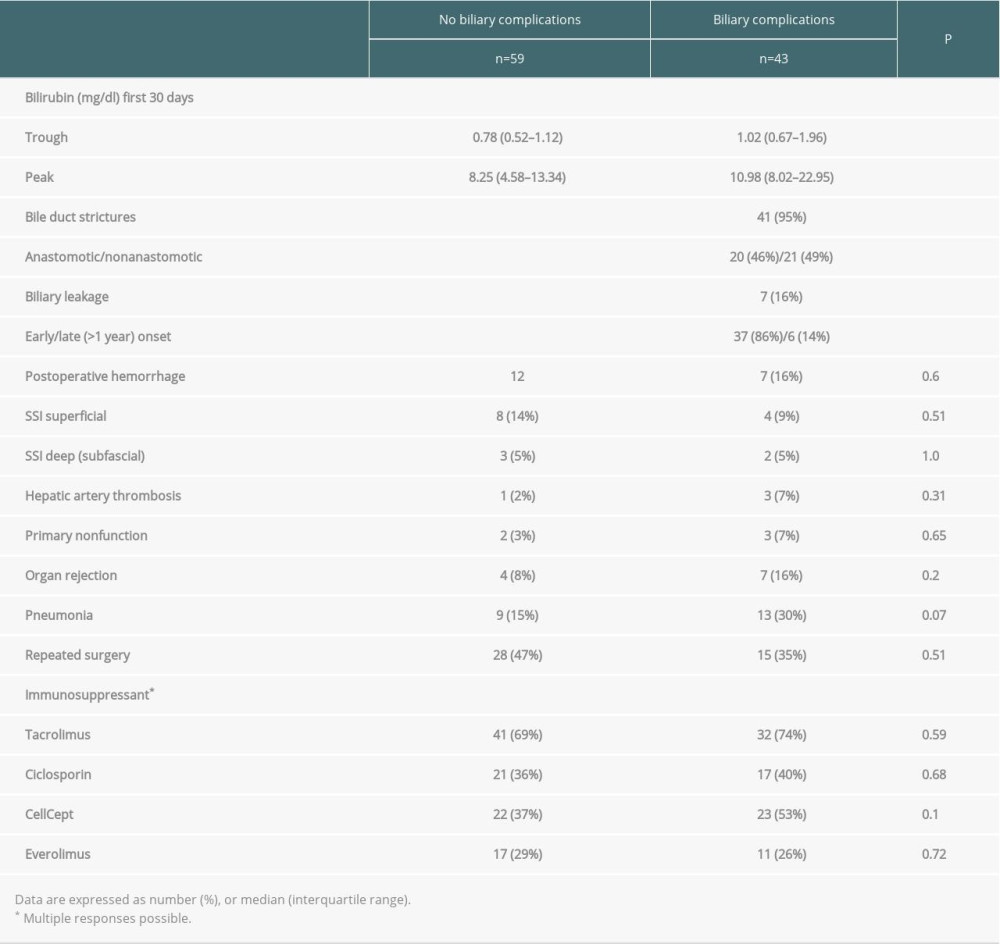 Table 3. Complications and immunosuppressive regimens.
Table 3. Complications and immunosuppressive regimens. Table 4. Risk factors for one-year mortality.
Table 4. Risk factors for one-year mortality.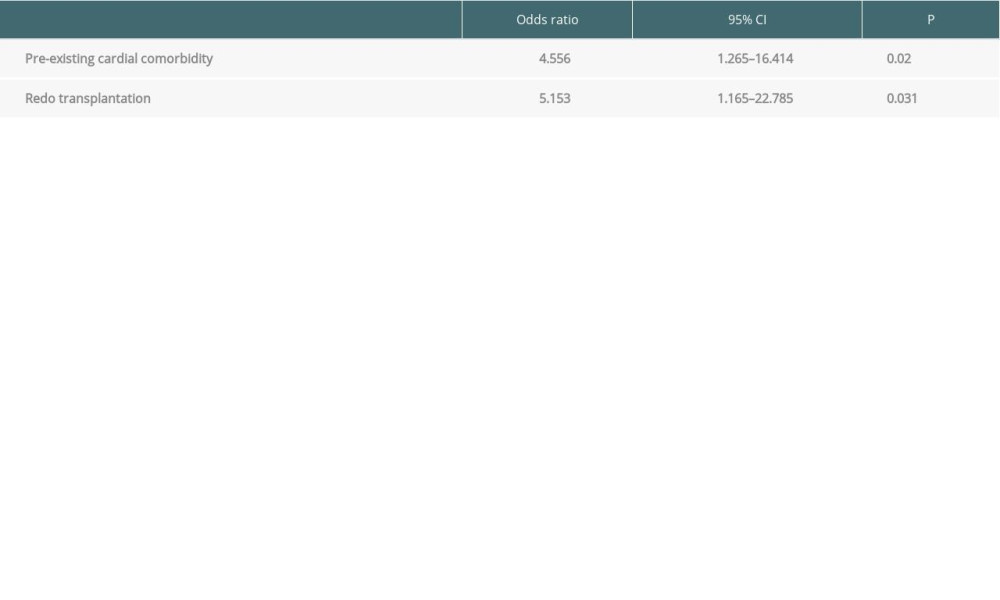 Table 5. Preoperative risk factors for one-year mortality: multivariate logistic regression analysis.Table 1. Demographics.Table 2. Perioperative characteristics.Table 3. Complications and immunosuppressive regimens.Table 4. Risk factors for one-year mortality.Table 5. Preoperative risk factors for one-year mortality: multivariate logistic regression analysis.
Table 5. Preoperative risk factors for one-year mortality: multivariate logistic regression analysis.Table 1. Demographics.Table 2. Perioperative characteristics.Table 3. Complications and immunosuppressive regimens.Table 4. Risk factors for one-year mortality.Table 5. Preoperative risk factors for one-year mortality: multivariate logistic regression analysis. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988