20 April 2021: Original Paper
Long-Term Outcomes of Early Experience in Donation After Circulatory Death Liver Transplantation: Outcomes at 10 Years
Omar J. Haque12ADEF*, Eve M. Roth12ADEF, Aaron Fleishman12ABCDE, Devin E. Eckhoff12ADG, Khalid Khwaja12ADEGDOI: 10.12659/AOT.930243
Ann Transplant 2021; 26:e930243






Abstract
BACKGROUND: Donation after circulatory death (DCD) livers remain an underutilized pool of transplantable organs due to concerns of inferior long-term patient survival (PS) and graft survival (GS), which factors greatly into clinician decision-making and patient expectations.
MATERIAL AND METHODS: This retrospective study used SRTR data to assess 33 429 deceased-donor liver transplants (LT) and compared outcomes between DCD and donation after brain death (DBD) LT recipients in the United States. Data were collected from 2002 to 2008 to obtain 10 years of follow-up (2012-2018) in the era of MELD implementation. Propensity scores for donor type (DCD vs DBD) were estimated using logistic regression, and the association of donor type with 10-year outcomes was evaluated after adjustment using stabilized inverse probability of treatment weights.
RESULTS: After adjusting for confounders, patient survival for DBD recipients at 10 years was 60.7% versus 57.5% for DCD recipients (P=0.24). Incorporating retransplants, 10-year adjusted patient survival was 60.2% for DBD recipients versus 55.5% for DCD recipients (P=0.07). Adjusted 10-year graft survival for DBD recipients was 56.4% versus 45.4% for DCD recipients (P<0.001). Surprisingly, however, 1 year after LT, DBD and DCD graft failure rates converged to 7.5% over the remaining 9 years.
CONCLUSIONS: These data reveal inferior 10-year DCD graft survival, but only in the first year after LT, and similar 10-year patient survival in DCD LT recipients compared to DBD recipients. Our results show the stability and longevity of DCD grafts, which should encourage the increased utilization of these livers for transplantation.
Keywords: Graft Survival, Liver Transplantation, Outcome Assessment (Health Care), Tissue and Organ Procurement, Tissue Survival, Transplantation Conditioning, Brain Death, Carcinoma, Hepatocellular, Death, End stage liver disease, Liver Neoplasms, Severity of Illness Index, Tissue Donors
Background
In the United States, over 13 000 patients are on the waiting list for a liver transplant (LT), while only 8896 LTs are performed annually [1]. This discrepancy between the supply and demand for organs continues to increase, and as a result, efforts to expand the donor pool are a central focus of the field. One solution to mitigate the liver organ shortage is the increased utilization of donation after circulatory death (DCD) livers [2,3].
DCD livers are procured for transplantation after diagnosed and confirmed cardio-respiratory death. In contrast to donation after brain death (DBD), in which donor organs are perfused via mechanical ventilation throughout the organ recovery process, DCD organs are procured under either controlled or uncontrolled donation conditions. In the former, the anticipated death of a donor prompts planned removal of life-sustaining measures, while in the latter, unexpected cardiopulmonary arrest followed by failed resuscitation leads to subsequent organ procurement [4]. In DCD organ donation, the lengthened time period from withdrawal of cardiopulmonary support until organ cooling via flush during the procurement operation – referred to as warm ischemic time (WIT) – is thought to decrease the quality of procured livers, causing higher rates of early allograft dysfunction and primary nonfunction [4].
Currently in the United States, only 12.1% of all LTs come from DCDs [5]. This practice is largely due to evidence that DCD livers may have worse long-term patient and graft survival compared to DBD livers, attributed to higher rates of biliary complications and ischemic cholangiopathy (IC) [2,6–9]. In addition, DCD grafts have increased rates of retransplantation and prolonged waitlist time for patients needing retransplants [10]. DCD LT has also been linked to end-stage renal disease [11].
However, recent evidence suggests that carefully selected DCD livers from younger donors have excellent outcomes, including better GS compared to DBD livers from older donors [10]. Outcomes may be comparable to DBD LT recipients, especially when IC can be prevented in DCD recipients [12]. In recent years, strategies have been developed to improve DCD LT outcomes, including minimizing cold ischemic time (CIT) and WIT, infusion of tissue plasminogen activator into the hepatic artery, and rapid donor organ removal protocols [10,13].
Additionally, the arrival of machine perfusion in the field of liver transplantation has greatly expanded the avenues to rescue marginal DCD livers for transplantation. Several normothermic machine perfusion (NMP) clinical trials have proven the benefits of recreating ex-vivo normothermic conditions for liver allografts, which are reflected in lower peak transaminase levels, reduced incidence of early allograft dysfunction, less hepatocellular graft injury, and equivalent clinical outcomes. The magnitude of these benefits have been significantly greater for DCD liver allografts compared to DBD grafts [14–18].
Based on the current debate on DCD versus DBD LT outcomes (especially long-term) and the changing landscape of marginal allograft modification with machine perfusion, we conducted a large retrospective cohort study using national SRTR data to assess long-term outcomes from the early experience in DCD versus DBD liver transplantation. In February 2002, the use of the MELD score was implemented by UNOS nationwide to improve LT allocation, and as a result, we chose to assess 10-year DCD LT outcomes in the era of MELD implementation (2002–2008) to obtain follow-up data from 2012–2018.
Because studies have shown the majority of DCD LT graft failure occurs within the first year after transplant [2,8,19], we hypothesized that long-term follow-up data would reveal equivalent graft survival (GS) rates at 1 year after LT. Our second hypothesis was that as rates of retransplantation of DCD allografts decreased and clinical experience with DCD LT increased, long-term patient survival (PS) between DCD and DBD LT recipients would be comparable. Both these hypotheses assess the longevity and stability of DCD liver allografts in a large national cohort and have major implications for their increased utilization in clinical decision-making to mitigate the organ shortage in the United States.
Material and Methods
PATIENT INCLUSION CRITERIA AND DATA ACQUISITION:
This study used data from the SRTR. The SRTR data system includes data on all donors, wait-listed candidates, and transplant recipients in the United States, submitted by the members of the Organ Procurement and Transplantation Network (OPTN). The Health Resources and Services Administration, United States Department of Health and Human Services provides oversight to the activities of the OPTN and SRTR contractors. Transplant recipient baseline data were linked with deceased-donor data and recipient follow-up data within the SRTR database.
We identified adults (≥18 years of age) who underwent a deceased donor, first-time, liver-only transplant between March 2002 and December 2008 to capture MELD score data with 10-year follow-up. Those who were missing data in the SRTR database on DCD versus DBD status (our main exposure), were excluded from our study cohort. The institutional review board at Beth Israel Deaconess Medical Center determined that the study met criteria for exempt status (Protocol #2019P000434).
STATISTICAL ANALYSIS:
We stratified the study cohort into DCD versus DBD recipients. Donor baseline characteristics were summarized as mean (standard deviation) or median (1st quartile and 3rd quartile) for continuous variables and counts (percentages) for categorical variables. To compare characteristics, we performed chi-squared tests for categorical variables, and t tests and Wilcoxon rank sum tests for normally and non-normally distributed data, respectively. To adjust for confounding, we utilized propensity score methods [20]. A propensity score was estimated using logistic regression with donor type as the outcome and all potential confounders as predictors. All covariates in the logistic regression were selected a priori and are presented in Table 1. Continuous variables were modeled flexibly using restricted cubic splines, which allows the model to fit non-linear relationships between predictor and outcome. We used the estimated probabilities from our logistic regression model to calculate stabilized inverse probability of treatment weights (sIPWs) [21]. The sIPWs were used to weight each patient’s contribution to the survival analyses described below. Baseline characteristics in our reweighted cohort were evaluated using standardized differences (SDs) to assess for balance between DCD and DBD groups. After satisfactory covariate balance was determined, treatment effects were estimated. Our primary outcome was overall PS and our secondary outcome was GS.
PATIENT SURVIVAL:
To assess differences in overall PS, recipients were followed from date of first liver transplant until death from any cause. Retransplants and those lost to follow-up were initially censored. However, this approach potentially violated the assumption of non-informative censoring; therefore, we performed a sensitivity analysis in which recipients were followed until death from any cause, including retransplantation. Both analyses with retransplants censored and retransplants incorporated were reported. Finally, LT recipients lost to follow-up were censored in the analysis.
GRAFT SURVIVAL:
In this analysis, we only assessed graft failure for first-time liver transplantation. SRTR defines graft failure as failure from any cause, including need for retransplantation or death, even with a functioning graft [22]. Those lost to follow-up were censored.
Patients with greater than 10 years of follow-up data were administratively censored in all analyses. Overall survival, stratified by donor type, was estimated using the Kaplan-Meier method and after reweighting using sIPWs. Donor types were compared using the log-rank test. The association between DCD and DBD with overall PS and GS was estimated using Cox proportional hazards regression models with reweighting using sIPWs; results were summarized using hazard ratios (HRs) with 95% confidence intervals (95% CIs). We used a robust variance estimator to account for the weights used during estimation [23]. Patients were excluded from survival analyses when missing recipient or donor characteristic information for any continuous variable. All tests were 2-sided and P values <0.05 were considered statistically significant. R version 3.6.3 (R Development Core Team, 2020) was used for all statistical analyses.
Results
PATIENT SURVIVAL (PS):
Median follow-up time for recipients with complete data was 3250 (q1=839, q3=3650) days. During follow-up, a total 10 141 recipients died of any cause. Kaplan-Meier survival analysis of post-LT PS with 10-year follow up was conducted with both unadjusted and reweighted data. With retransplants censored, the unadjusted overall PS for DBD liver recipients at 10 years was 60.1% (95% CI: 59.5%, 60.7%) versus 54.7% (95% CI: 51.9%, 57.7%) for DCD liver recipients (P =0.002) (Figure 1A).
After reweighting by sIPW, the overall adjusted PS for DBD liver recipients with retransplants censored at 1, 3, 5, and 10 years was 88.6% (95% CI: 88.2%, 89.0%), 80.2% (95% CI: 79.7%, 80.7%), 74.1% (95% CI: 73.6%, 74.7%), and 60.7% (95% CI: 60.1%, 61.3%), respectively. The overall adjusted PS for DCD liver recipients with retransplants censored at 1, 3, 5, and 10 years was 87.1% (95% CI: 84.1%, 90.2%), 77.2% (95% CI: 73.3%, 81.3%), 73.0% (95% CI: 68.9%, 77.3%), and 57.5% (95% CI: 52.8%, 62.6%), respectively. Notably, there was no statistically significant difference in 10-year PS after reweighting by sIPW between DBD and DCD liver recipients (p=0.24) (Figure 1B). In this analysis, the hazard ratio comparing overall PS between donor type was 1.11 (95% CI: 0.95, 1.29).
This analysis was repeated including all follow-up time and whether or not recipients were retransplanted. With retransplants incorporated, the unadjusted PS for DBD liver recipients at 10 years was 60.5% (95% CI: 59.9%, 61.1%) compared to 55.8% (95% CI: 52.8%, 59.0%) for DCD liver recipients (P<0.001) (Figure 2A). After reweighting with sIPW, the overall adjusted PS for DBD liver recipients with retransplants incorporated at 1, 3, 5, and 10 years was 88.5% (95% CI: 88.1%, 88.8%), 79.8% (95% CI: 79.4%, 80.3%), 73.7% (95% CI: 73.2%, 74.2%), and 60.2% (95% CI: 59.6%, 60.8%), respectively. The overall adjusted PS for DCD liver recipients with retransplants incorporated at 1, 3, 5, and 10 years was 86.6% (95% CI: 83.7%, 89.6%), 76.4% (95% CI: 72.7%, 80.3%), 72.2% (95% CI: 68.3%, 76.3%), and 55.5% (95% CI: 51.1%, 60.4%), respectively. Notably, there was no statistically significant difference in 10-year PS after reweighting by sIPW, even with retransplants incorporated, between DBD and DCD liver recipients (P=0.07) (Figure 2B). Similar to the primary overall PS analysis, the hazard ratio was 1.15 (95% CI: 1.00, 1.33).
GRAFT SURVIVAL (GS):
Median follow-up time was 3246 (q1=838, q3=3650) days and a total of 11 996 patients had graft failure. The unadjusted GS for DBD liver recipients at 10 years was 56.2% (95% CI: 55.6%, 56.8%) versus 46.1% (95% CI: 43.3%, 49.0%) for DCD liver recipients (P<0.001) (Figure 3A). Following reweighting with sIPW, the adjusted GS for DBD livers at 1, 3, 5, and 10 years was 85.1% (95% CI: 84.7%, 85.5%), 76.0% (95% CI: 75.5%, 76.5%), 69.7% (95% CI: 69.2%, 70.3%), and 56.4% (95% CI: 55.8%, 57.0%), respectively. The adjusted GS for DCD livers at 1, 3, 5, and 10 years was 77.0% (95% CI: 73.4%, 80.8%), 65.9% (95% CI: 61.7%, 70.4%), 59.0% (95% CI: 54.5%, 63.8%), and 45.4% (95% CI: 40.9%, 50.4%), respectively. There was a statistically significant difference in 10-year GS between DCD and DBD livers (P<0.001) (Figure 3B). The hazard ratio for this analysis was 1.42 (95% CI: 1.24,1.62). However, reweighted GS Kaplan-Meier curves revealed that 36% of DCD and 29% of DBD graft failure cases occurred within the first year of LT. At 1 year after LT, the percentage of DBD and DCD graft failure cases converged at 7% and 8%, respectively, per year.
Discussion
In 2019, there were 4000 fewer LTs than patients on the LT waitlist in the United States [1]. As the liver organ shortage persists, efforts to expand the organ pool must continue. Recent data have shown that DCD livers are a potential source of acceptable but underutilized organs [3], with evidence showing comparable graft and patient survival in well-selected recipients [10,12]. The arguments against these conclusions are that they derive from small, single-center cohort studies, or that the follow-up time of 1–5 years is insufficient. Our study addressed this gap by assessing long-term (10-year) DCD liver allograft stability on a national scale. We showed that 10-year PS was not statistically different based on early DCD LT experience compared to DBD LTs. It was previously thought that DCD LT recipients had higher rates of retransplantation, and retransplanted patients had worse outcomes [24]. While the latter remains true, the rate of DCD retransplantation drastically decreased over the years [25]. Thus, as the rates of retransplantation in DCD LT recipients decreased, overall PS of this group rose.
Other reasons for improved long-term DCD LT patient survival were better recipient and organ selection. In 2009, the American Society for Transplant Surgeons (ASTS) released guidelines for DCD LT, which included CIT less than 8 h, total WIT less than 30 min, and donor age younger than 55 years [26]. Adherence to these guidelines leading to stricter allograft selection improved PS, decreased rates of graft nonfunction, and shortened post-operative hospital courses [27–29]. These clinical improvements were reflected in the results of this study, as incorporating retransplanted patients into survival analysis only decreased 10-year DCD PS by 2.0% compared to the retransplant-censored group.
Despite comparable PS, DCD livers were shown to have lower 10-year GS compared to DBD livers. However, the differences in 10-year GS between DCD and DBD livers were due to events in the first year after LT. We showed that DCD allografts that survived the first year had similar 10-year graft failure rates compared to their DBD counterparts, at 7–8% (Figure 3B). This result underscores the importance of assessing long-term outcomes in DCD liver allografts, as the problems with longevity are actually upfront. Additionally, the incorporation of machine perfusion technology in liver transplantation provides a platform to reduce graft failure in these organs. Schlegel et al demonstrated that hypothermic oxygenated perfusion (HOPE)-treated DCD liver allografts had significantly less biliary cirrhosis and fibrosis at 4 weeks after LT due to less reperfusion injury after machine perfusion [30]. The same group demonstrated HOPE livers had longer 5-year GS due to less primary nonfunction and IC compared to static cold storage (SCS) DCD allografts [31]. Dual hypothermic oxygenation machine perfusion (DHOPE)-treated DCD livers also had similar improvements in 6 and 12 month GS and biliary complications [32]. Finally, NMP has been shown to improve GS in DCD allografts. Op Den Dries et al revealed that NMP provided superior preservation of bile duct endothelial cell function in DCD livers compared to allografts preserved with SCS [33]. Additionally, Liu et al indicated that NMP reduced biliary complications after LT by enhancing regeneration of biliary epithelial cells [34]. These studies signify that machine perfusion has the potential to address the Achilles heel of DCD LT: high rates of graft failure within the first year of LT secondary to IC and biliary complications. Our data shows that if the recent assimilation of machine perfusion in clinical practice can alleviate these early biliary problems within the first year of transplant, the long-term stability of DCD allografts is comparable to DBD livers.
The findings of this study have major clinical and policy implications. This analysis of the early experience with DCD liver transplantation revealed that DCD donors were younger and healthier, with fewer comorbidities, than DBD donors. DCD LT recipients were older and had lower median MELD scores (15 versus 17). Thus, the clinical practice trend was transplanting DCD livers in older but relatively healthy recipients, and transplanting DBD livers (which comprise the majority of LTs) into younger patients who had longer life expectancies, or sicker recipients who could not physiologically tolerate DCD liver allografts [35,36]. Our data suggest that this clinical practice can be expanded with increased utilization of DCD livers in well-selected LT patients without compromising long-term PS. Additionally, machine perfusion of DCD liver allografts can now mitigate the high rates of graft failure in these organs. Thus, while the field of LT has gained tremendous clinical experience with DCD livers over the past decade, currently only 12.1% of all LTs come from DCD donors [5], suggesting that transplantable DCD livers are being underutilized.
This study is not without limitations. Despite using a large national transplant database, analysis of biliary tract complications and graft failure reasons were limited due to missing data. Biliary complications were unknown in 82% of DCD LT recipients and 90% of DBD LT recipients, and graft failure reason was unknown in 93% of LTs. Thus, despite the statistical significance of differences between these 2 recipient pools, the large percentages of unknown data due to lack of a United Network for Organ Sharing reporting requirement made these findings null. As a result, the majority of literature on IC and graft failure reasons in DCD versus DBD LT is confined to single-center studies. Statistical issues with lack of power in SRTR data have prompted a call for standardization of transplantation metrics nationwide [37].
Conclusions
In conclusion, our study demonstrated long-term stability of DCD liver allografts. Results showed that 10-year PS was comparable between the early experience in DCD LTs compared to DBD LTs, even after incorporating retransplants. We suspect these findings were due to the decreased rate of retransplantation in DCD LTs secondary to improved organ and patient selection and shorter ischemic times. DCD liver recipients had an 11% lower 10-year GS compared to DBD LTs, but at 1 year after LT, the long-term graft failure rates were equivalent. These data show that clinical experience with DCD LT has increased and with the advent of machine perfusion technology to tackle early biliary complications, the time for increased DCD liver utilization yielding good long-term patient outcomes has arrived.
Figures
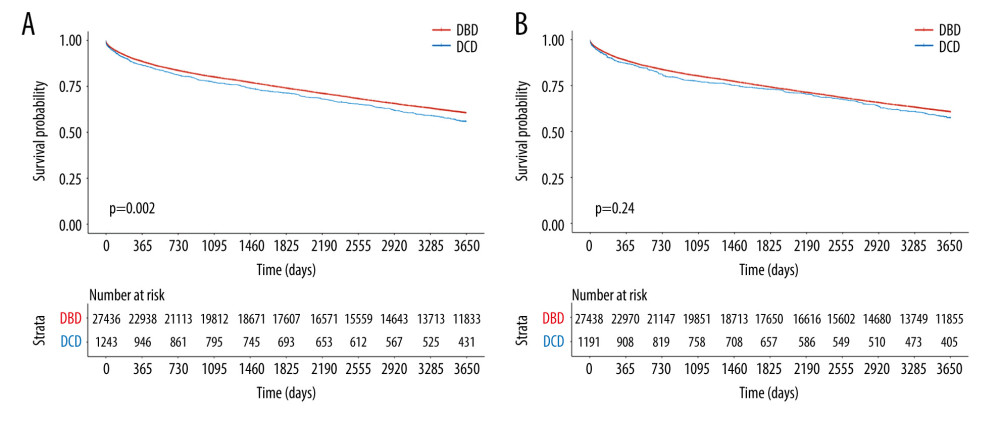 Figure 1. Kaplan-Meier curves of patient survival stratified by DCD vs DBD liver transplant with retransplants censored in (A) unadjusted groups (P=0.002) and (B) sIPW reweighted groups (P=0.24).
Figure 1. Kaplan-Meier curves of patient survival stratified by DCD vs DBD liver transplant with retransplants censored in (A) unadjusted groups (P=0.002) and (B) sIPW reweighted groups (P=0.24). 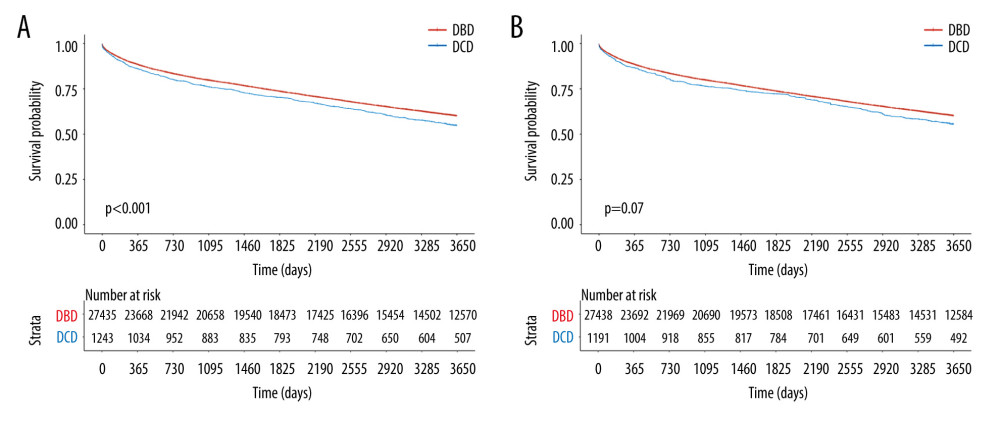 Figure 2. Kaplan-Meier curves of patient survival stratified by DCD vs DBD liver transplant with retransplants incorporated in (A) unadjusted groups (P<0.001) and (B) sIPW reweighted groups (P=0.07).
Figure 2. Kaplan-Meier curves of patient survival stratified by DCD vs DBD liver transplant with retransplants incorporated in (A) unadjusted groups (P<0.001) and (B) sIPW reweighted groups (P=0.07). 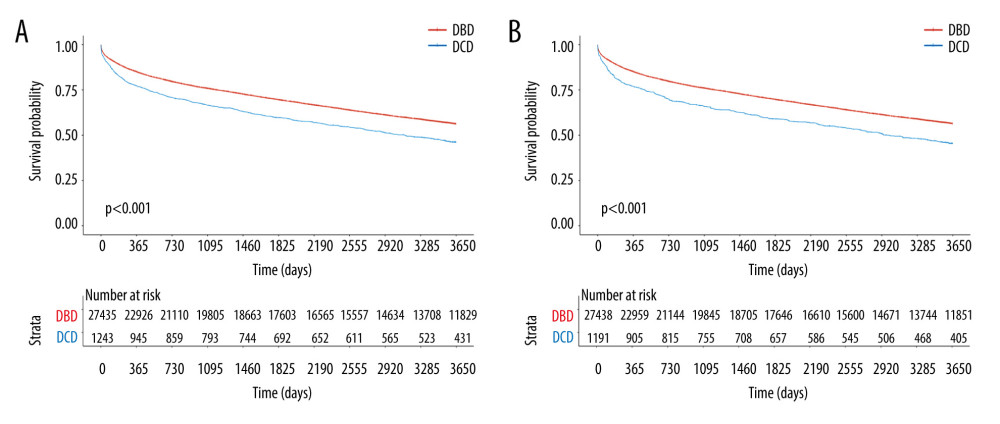 Figure 3. Kaplan-Meier curves of graft survival stratified by DCD vs DBD liver transplant in (A) unadjusted groups (p<0.001) and (B) sIPW reweighted groups (P<0.001).
Figure 3. Kaplan-Meier curves of graft survival stratified by DCD vs DBD liver transplant in (A) unadjusted groups (p<0.001) and (B) sIPW reweighted groups (P<0.001). References
1. Organ Procurement and Transplantation Network: Data | OPTN. Organ Procurement and Transplantation Network, 2019
2. Mathur AK, Heimbach J, Steffick DE, Donation after cardiac death liver transplantation: Predictors of outcome: Am J Transplant, 2010; 10; 2512-19
3. Leithead JA, Tariciotti L, Gunson B, Donation after cardiac death liver transplant recipients have an increased frequency of acute kidney injury: Am J Transplant, 2012; 12; 965-75
4. Monbaliu D, Pirenne J, Talbot D, Liver transplantation using donation after cardiac death donors: J Hepatol, 2012; 56; 474-85
5. Eren EA, Latchana N, Beal E, Donations after circulatory death in liver transplant: Exp Clin Transplant, 2016; 14; 463-70
6. O’Neill S, Roebuck A, Khoo E, A meta-analysis and meta-regression of outcomes including biliary complications in donation after cardiac death liver transplantation: Transpl Int, 2014; 27; 1159-74
7. Foley DP, Fernandez LA, Leverson G, Donation after cardiac death: The University of Wisconsin experience with liver transplantation: Ann Surg, 2005; 242; 724-31
8. Selck FW, Grossman EB, Ratner LE, Utilization, outcomes, and retransplantation of liver allografts from donation after cardiac death: Implications for further expansion of the deceased-donor pool: Ann Surg, 2008; 248; 599-607
9. Jay CL, Lyuksemburg V, Ladner DP, Ischemic cholangiopathy after controlled donation after cardiac death liver transplantation: A meta-analysis: Ann Surg, 2011; 253; 259-64
10. Scalea JR, Redfield RR, Foley DP, Liver transplant outcomes using ideal donation after circulatory death livers are superior to using older donation after brain death donor livers: Liver Transplant, 2016; 22; 1197-204
11. Ruebner RL, Reese PP, Abt PL, Donation after cardiac death liver transplantation is associated with increased risk of end-stage renal disease: Transpl Int, 2014; 27; 1263-71
12. Croome KP, Lee DD, Perry DK, Comparison of longterm outcomes and quality of life in recipients of donation after cardiac death liver grafts with a propensity-matched cohort: Liver Transplant, 2017; 23; 342-51
13. le Dinh H, de Roover A, Kaba A, Donation after cardio-circulatory death liver transplantation: World J Gastroenterol, 2012; 18; 4491-4506
14. Nasralla D, Coussios CC, Mergental H, A randomized trial of normothermic preservation in liver transplantation: Nature, 2018; 577; 50-56
15. Nassar A, Liu Q, Farias K, Ex vivo normothermic machine perfusion is safe, simple, and reliable: Results from a large animal model: Surg Innov, 2015; 22; 61-69
16. Ravikumar R, Jassem W, Mergental H, Liver transplantation after ex vivo normothermic machine preservation: A phase 1 (first-in-man) clinical trial: Am J Transplant, 2016; 16; 1779-87
17. Ravikumar R, Leuvenink H, Friend PJ, Normothermic liver preservation: A new paradigm?: Transpl Int, 2015; 28; 690-99
18. Bral M, Gala-Lopez B, Bigam D, Preliminary single-center canadian experience of human normothermic ex vivo liver perfusion: Results of a clinical trial: Am J Transplant, 2017; 17; 1071-80
19. Merion RM, Pelletier SJ, Goodrich N, Donation after cardiac death as a strategy to increase deceased donor liver availability: Ann Surg, 2006; 244; 555-62
20. Rosenbaum PR, Rubin DB, The central role of the propensity score in observational studies for causal effects: Biometrika, 1983; 70; 41-55
21. Cole SR, Hernán MA, Constructing inverse probability weights for marginal structural models: Am J Epidemiol, 2008; 168; 656-64
22. Kwong A, Kim WR, Lake JR, OPTN/SRTR 2018 annual data report: Liver: Am J Transplant, 2020; 20; 193-299
23. Joffe MM, Ten Have TR, Feldman HI, Model selection, confounder control, and marginal structural models: Review and new applications: American Statistician, 2004; 58; 272-79
24. Sher L, Quintini C, Fayek SA, Attitudes and barriers to the use of donation after cardiac death livers: Comparison of a United States transplant center survey to the united network for organ sharing data: Liver Transplant, 2017; 23; 1372-83
25. Biggins SW, Futility and rationing in liver retransplantation: When and how can we say no?: J Hepatol, 2012; 56; 1404-11
26. Reich DJ, Mulligan DC, Abt PL, ASTS recommended practice guidelines for controlled donation after cardiac death organ procurement and transplantation: Am J Transplant, 2009; 9; 2004-11
27. Chan EY, Olson LC, Kisthard JA, Ischemic cholangiopathy following liver transplantation from donation after cardiac death donors: Liver Transplant, 2008; 14; 604-10
28. Paterno F, Guarrera JV, Wima K, Clinical implications of donor warm and cold ischemia time in donor after circulatory death liver transplantation: Liver Transplant, 2019; 25; 1342-52
29. Mergental H, Perera MTPR, Laing RW, Transplantation of declined liver allografts following normothermic ex-situ evaluation: Am J Transplant, 2016; 16; 3235-45
30. Schlegel A, Graf R, Clavien PA, Dutkowski P, Hypothermic oxygenated perfusion (HOPE) protects from biliary injury in a rodent model of DCD liver transplantation: J Hepatol, 2013; 59; 984-91
31. Schlegel A, Muller X, Kalisvaart M, Outcomes of DCD liver transplantation using organs treated by hypothermic oxygenated perfusion before implantation: J Hepatol, 2019; 70; 50-57
32. van Rijn R, Karimian N, Matton APM, Dual hypothermic oxygenated machine perfusion in liver transplants donated after circulatory death: Br J Surg, 2017; 104; 907-17
33. op den Dries S, Karimian N, Westerkamp AC, Normothermic machine perfusion reduces bile duct injury and improves biliary epithelial function in rat donor livers: Liver Transplant, 2016; 22; 994-1005
34. Liu Q, Nassar A, Farias K, Sanguineous normothermic machine perfusion improves hemodynamics and biliary epithelial regeneration in donation after cardiac death porcine livers: Liver Transplant, 2014; 20; 987-99
35. Grewal HP, Willingham DL, Nguyen J, Liver transplantation using controlled donation after cardiac death donors: An analysis of a large single-center experience: Liver Transplant, 2009; 15; 1028-35
36. Detry O, Seydel B, Delbouille MH, Liver transplant donation after cardiac death: Experience at the University of Liege: Transplant Proc, 2009; 41; 582-84
37. Goldberg D, Karp S, Shah MB, Importance of incorporating standardized, verifiable, objective metrics of organ procurement organization performance into discussions about organ allocation: Am J Transplant, 2019; 19; 2973-78
Figures
Figure 1. Kaplan-Meier curves of patient survival stratified by DCD vs DBD liver transplant with retransplants censored in (A) unadjusted groups (P=0.002) and (B) sIPW reweighted groups (P=0.24).Figure 2. Kaplan-Meier curves of patient survival stratified by DCD vs DBD liver transplant with retransplants incorporated in (A) unadjusted groups (P<0.001) and (B) sIPW reweighted groups (P=0.07).Figure 3. Kaplan-Meier curves of graft survival stratified by DCD vs DBD liver transplant in (A) unadjusted groups (p<0.001) and (B) sIPW reweighted groups (P<0.001). Tables
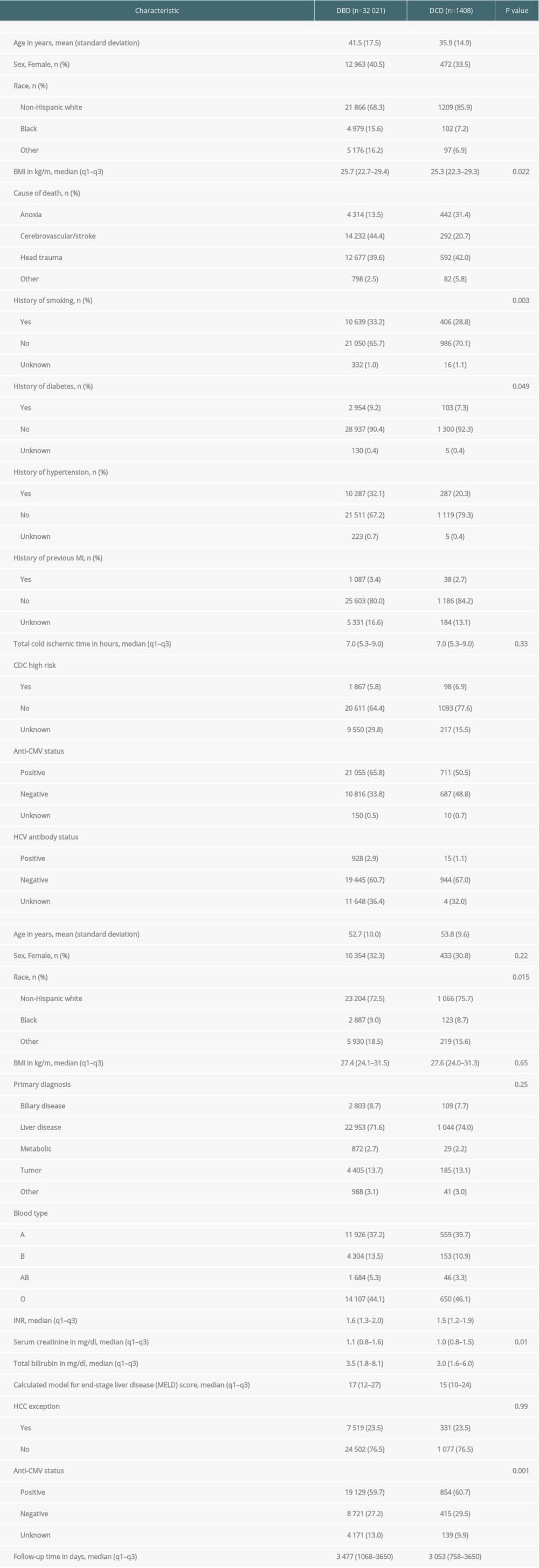 Table 1. Liver transplant donor and recipient characteristics.
Table 1. Liver transplant donor and recipient characteristics.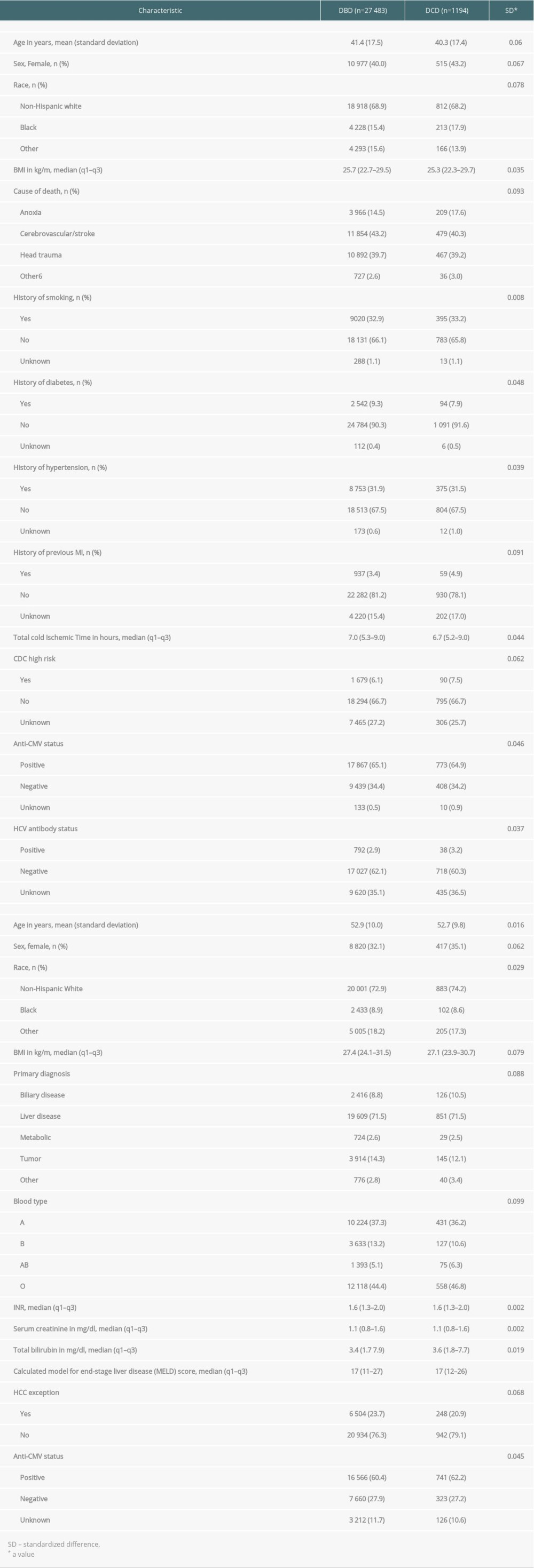 Table 2. Liver transplant donor and recipient characteristics reweighted using stabilized inverse probability of treatment weights (sIPWs).Table 1. Liver transplant donor and recipient characteristics.Table 2. Liver transplant donor and recipient characteristics reweighted using stabilized inverse probability of treatment weights (sIPWs).
Table 2. Liver transplant donor and recipient characteristics reweighted using stabilized inverse probability of treatment weights (sIPWs).Table 1. Liver transplant donor and recipient characteristics.Table 2. Liver transplant donor and recipient characteristics reweighted using stabilized inverse probability of treatment weights (sIPWs). In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988