26 November 2021: Original Paper
Validation of Accuracy of Non-Invasive Imaging Methods (Magnetic Resonance Imaging (MRI) Fat Fraction Calculation and Computed Tomography (CT) Liver Attenuation Index) for Hepatic Graft Fat Quantification in Living Liver Transplant Donors
Abhideep ChaudharyDOI: 10.12659/AOT.933801
Ann Transplant 2021; 26:e933801






Abstract
BACKGROUND: Diagnosis of significant hepatic graft steatosis remains vital for success of any transplant program as it has an impact on donor morbidity and recipient survival. Even histopathological quantification faces limitations. The present study compared the diagnostic accuracy of CT-LAI and MRI fat fraction imaging with histopathological analysis for donor graft parenchymal fat quantification.
MATERIAL AND METHODS: CT-LAI and MR-FF values and histopathological fat quantification results of 273 patients were identified from electronic records of the author’s institutes from September 2015 to April 2020. Data analysis was done using SPSS version 21.0.
RESULTS: Most participants were young with nearly equal sex distribution and significant number of overweight and obese patients. Moderate agreement and significant positive correlation were found between MR fat fraction (%) and biopsy-macrosteatosis (%). Diagnostic accuracy and negative predictive value of MRI for fat fraction calculation was high (95.24% and 98.07% for fat fraction of 10% threshold, respectively), and it further improved for fat fraction threshold of 15%.
CONCLUSIONS: MRI-based fat quantification calculation displayed near-perfect negative predictive values and very high diagnostic accuracy, suggesting that it can obviate the need for biopsy in patients with graft fat percentage <10% on MRI.
Keywords: Liver Transplantation, Magnetic Resonance Imaging, multidetector computed tomography, Humans, Liver, Living Donors, Tomography, X-Ray Computed
Background
An acute shortage of cadaveric grafts (less than 5 per million population) in the Asia-Pacific region has led to development of a robust living donor liver transplant program in the region, which has been evolving rapidly in the past 2 decades [1]. However, with rapidly expanding programs the concern for donor safety has been increasing. Many authors have considered factors leading to morbidity and prolonged hospitalization among living donors [2,3]. Steatosis of the donor liver is one of the factors responsible for donor morbidity [4]. Besides having an impact on donor health, it also affects graft rejection and recipient survival [5]. Hence, diagnosis of significant graft steatosis remains vital for the success of any transplant program.
The threshold of significant graft steatosis remains institutional and no standard guideline exists for defining acceptable fat steatosis percentage. Multiple authors have claimed that even donors with moderate to severe hepatic steatosis can be accepted for transplant programs with slight alterations and strict surgical algorithms [6–8]. Most authors agree that mild steatosis (≤30%) is an acceptable threshold with non-significant effects on donor morbidity or graft survival. However, there are biochemical derangements and subclinical effects of even mild steatosis leading to a more conservative acceptable threshold of 10–30% in many transplant centers [9,10]. Various diagnostic methods exist for this purpose, with histopathological analysis of the graft liver being the reliable criterion standard, but this method is not free from limitations when used for the purpose. A very small area of the liver is assessed, which can lead to erroneous interpretation due to extrapolation of that result to the entire liver graft. Also, there is subjective variability on assessment of intracellular lipid droplets in the hepatic cells. This, combined with the invasiveness of the method, leads transplant teams to search for non-invasive imaging alternatives for fat quantification and selection for transplant.
Multiple authors have investigated the utility of non-invasive investigations as a screening tool, but few authors have assessed if any of these investigations can obviate the need for biopsy and act as a stand-alone reliable indicator of parenchymal fat percentage. If a non-invasive investigation can quantify the graft parenchymal fat percentage with high negative predictive value and accuracy, it may be possible to use it as a primary tool for fat quantification and donor rejection in cases of higher fat values. The second criterion is that the investigation should be qualitatively and quantitatively reproducible with little inter-observer variation in terms of analysis and interpretation [11,12]. The present study compared the diagnostic accuracy of CT (computed tomography) LAI (liver attenuation index) and MRI fat fraction imaging with histopathological analysis for donor graft parenchymal fat quantification.
Material and Methods
PATIENTS:
A total of 273 patients were identified from electronic records of the authors’ institutes (first institute from September 2015 to July 2019 and second institute from July 2019 to April 2020) from the list of liver donors who underwent pre-operative non-invasive image-guided liver fat quantification and intraoperative graft biopsy as a part of their pretransplant institutional protocol. These included 152 males and 121 females with complete pretransplant CT, MRI (magnetic resonance imaging) evaluation, and liver biopsy results. Demographic characteristics and body mass index (BMI) were recorded. The maximum interval between imaging and transplant (biopsy) was 30 days. Their ages ranged from 18 to 61 years, with a mean age 32 years and a standard deviation of 9 years. The BMI ranged from 15.5 to 37 kg/m2 with mean value of 24.6 kg/m2 and standard deviation of 3.9 kg/m2.
CT SCANNER & TECHNIQUE:
The CT scanning in the first institute was performed on a 64-slice dual-energy GE scanner (CT750HD) and in the second institute on a 128-slice GE scanner (Revolution).
CT-LAI calculation was done as described in the literature [13]. Twenty-five ROIs each measuring 1 cm2 were placed over the liver parenchyma (non-enhanced phase) in both lobes, avoiding the inclusion of any large vessels or biliary structures. The average of the values was taken as the mean liver parenchymal attenuation. Similarly, 5 ROIs were placed in the splenic parenchyma, avoiding large vessels, and the averages of the values were calculated as the splenic parenchymal attenuation index. The liver attenuation index was calculated as the difference of the hepatic and splenic attenuation index.
MR SCANNER & TECHNIQUE:
MR scanning in the first institute was performed on a Philips Ingenia 3 tesla scanner and in the second institute on a GE Sigma 1.5 tesla scanner.
The liver fat fraction was measured by the dual-echo sequences Dixon/IDEAL sequences. The individual sequence parameters in institute 1 were: FOV – 400×353, TR – 3.4, TE1 – 1.16, TE2 – 2.2, and matrix – 236×207, and the parameters in institute 2 were: FOV – 620×400, TR – 12, TE1 – 2.2, TE2 – 4.5, and matrix – 128×160.
HISTOPATHOLOGICAL ANALYSIS:
Intraoperative liver biopsy was performed from all the patients from the edge of the graft liver during the transplant surgery. Biopsy was done using an 18 G automatic needle with 22 mm throw and 19 mm sample notch length. The steatosis was quantified by the histopathologist as the percentage of cells with intracellular fat vacuoles.
STATISTICAL ANALYSIS:
The data were entered in an MS EXCEL spreadsheet and analysis was done using SPSS version 21.0. Categorical variables are presented as number and percentage (%) and continuous variables are presented as mean±SD and median. Inter-rater kappa agreement was used to assess the strength of agreement between MRCP (magnetic resonance cholangio-pancreatography) fat and biopsy-macrosteatosis and between CT-LAI and biopsy-macrosteatosis. Diagnostic testing was used to calculate sensitivity, specificity, PPV (positive predictive value), and NPV (negative predictive value). Receiver operating characteristic curve analysis was used to determine the AUC (area under the curve). Spearman rank correlation coefficient analysis was used to determine the correlation of CT-LAI, MRCP fat (%), and biopsy-macrosteatosis (%) with each other. Bland-Altman plots were used to compare findings of biopsy-macrosteatosis and MRCP fat. A
Results
:
Most participants were young, with 42.86% in the age group 21–30 years; 55.68% of patients were males and 44.32% were females. Most (51.65%) patients had a body mass index (BMI, kg/m2) within normal limits (18.5–24.9), but a significant percentage of patients were overweight (30.77%) or obese (13.19%).
:
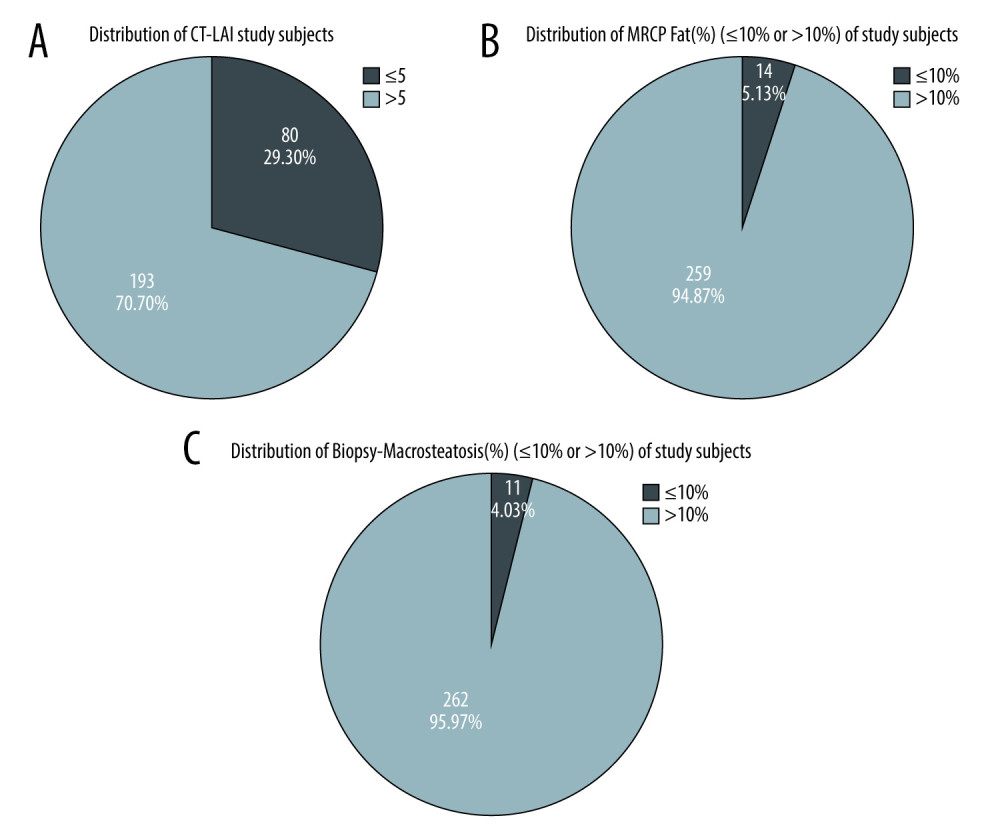
In most (70.70%) patients, CT-LAI was >5, and CT-LAI was ≤5 in 80 out of 273 patients (29.30%). The mean value of CT-LAI of study subjects was 7.45±5.22, with a median (IQR) of 7.3(5–10.3).
:
The mean value of MRCP fat (%) of study subjects was 3.52±3.26, with a median (IQR) of 2.8 (1.2–4.8). In most (94.87%) patients, the MRCP fat fraction was ≤10%, and the MRCP fat fraction was >10% in only 14 out of 273 patients (5.13%). In fact, 99.27% had ≤15% parenchymal fat as detected by MRCP. The MRCP fat fraction was >15% in only 2 out of 273 patients (0.73%).
:
Mean value of biopsy-macrosteatosis (%) of study subjects was 1.5±3.15, with a median (IQR) of 0 (0–2). In most (95.97%) patients, biopsy-macrosteatosis (%) was ≤10%, and biopsy-macrosteatosis (%) was >10% in only 11 out of 273 patients. In most (99.27%) patients, biopsy-macrosteatosis (%) was ≤15%. Biopsy-macrosteatosis (%) was >15% in only 2 out of 273 patients (0.73%).
ACCURACY OF THE NON-INVASIVE IMAGING TESTS COMPARED TO HISTOPATHOLOGY:
There is poor agreement between biopsy-macrosteatosis (%) and CT-LAI, with kappa 0.035 and P value 0.027 (Table 2). Among 271 patients diagnosed as having non-significant via biopsy-macrosteatosis (%), 193 patients had similar findings in CT-LAI. Among 2 patients diagnosed as having significant via biopsy-macrosteatosis (%), 2 patients had similar findings in CT-LAI. The overall concordance rate was 71.43% and the overall discordance rate was 28.57% between biopsy-macrosteatosis (%) and CT-LAI.
There was moderate agreement between biopsy-macrosteatosis (%) and MRCP fat, (%) with kappa 0.455 and P value <.0001 (Table 3). Among 262 patients diagnosed as ≤10% via biopsy-macrosteatosis (%), 254 patients had similar findings in MRCP fat (%). Among 11 patients diagnosed as having >10% via biopsy-macrosteatosis (%), 6 patients had similar findings in MRCP fat (%). The overall concordance rate was 95.24% and the overall discordance rate was 4.76% between biopsy-macrosteatosis (%) and MRCP fat (%) (Table 4).
A significant positive correlation was seen between biopsy-macrosteatosis (%) and MRCP fat (%), with a correlation coefficient of 0.441. A significant negative correlation was seen between biopsy-macrosteatosis (%) and CT-LAI, with a correlation coefficient of −0.283 (Table 5).
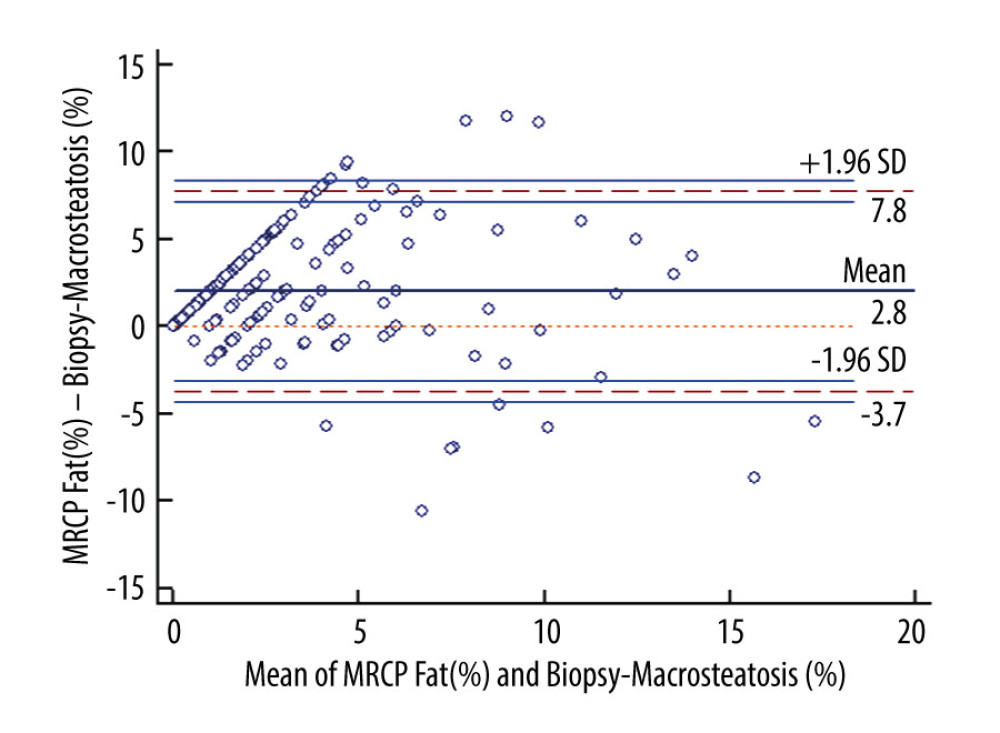
The average of the differences between MRCP and actual fat was 2.02%. This means that on average, the fat measured by MRCP measures 2.02% more than the actual fat. The limits of agreement estimated an interval of −3.7151 to 7.762. The results obtained from fat measured by MRCP may be 3.7151% below or 7.762% above the actual fat (Figure 2).
Discussion
We assessed the diagnostic accuracy of CT-LAI and MR Dixon fat fraction (FF) calculation in computation of graft steatosis in living donors using histopathology as the criterion standard reference. The results demonstrate very high negative predictive values (>97%) of both of these imaging studies in ruling out minimal graft parenchymal steatosis (10% or more). The criterion of 10% steatosis agrees with the institutional threshold, but also kept with the intention to be an accurate predictor in institutions with the most conservative thresholds. If the imaging studies display good diagnostic accuracy with this threshold, the results can be extrapolated with even higher accuracy for institutes with higher thresholds.
Although both CT-LAI and MR Dixon imaging results were positive in terms of high diagnostic accuracy, CT-LAI had limitations due to the semi-quantitative nature of its results, relatively poor statistical correlation with histopathology results, and low specificity. However, the steatosis percentage calculation based on MR-FF imaging revealed a very high negative predictive value (>98%) and diagnostic accuracy (>95%) in predicting fat percentage <10%, which improved at higher fat percentages (>99% NPV and >98% diagnostic accuracy in prediction of fat percentage <15%).
Our results reaffirm the conclusion of previous authors reporting good correlation of CT-LAI and MR-FF imaging with histopathology and high diagnostic accuracy and near-perfect negative predictive values of MR-FF imaging when compared to histopathology for quantification of macrosteatosis in donor livers. Few published studies have assessed the role of MRI-based fat quantification for creating a more selective role of liver biopsy for potential liver donors. However, to the best of our knowledge, there have been very few studies assessing the role of MR fat quantification techniques allowing total replacement of liver biopsy in potential liver donors [12]. A study with the same intent, extracted from data from a different cohort of population, with similar findings of high NPV, could help establish the reproducibility of the results and validate its utility. To the best of our knowledge, our study has the largest sample of patients studied for this purpose. The present study has the strength of being conducted in 2 different institutions, although sequentially, and with the same team of transplant surgeons and investigators. We did not study MR spectroscopy due to lack of institutional protocol of the sequence being used regularly for the purpose, but we believe that it would be technically more challenging, time consuming, and has the same limitation as biopsy of analyzing a small region of interest rather than diffuse parenchyma., Rastogi et al and other authors studied the correlation of MR spectroscopic fat quantification with MR Dixon-based quantification and histopathology, and found no significant difference in results, suggesting that Dixon-based imaging is sufficient for the purpose [14,15].
The low positive predictive value of MRI seen in our study agrees with previous studies. We also noticed that few authors have used MR fat fraction-based cut-off values of 5% to predict steatosis of 10% when compared with histopathological analysis [12,15,16]. This difference of scale was justified and expected, as MR-based methods revealed a relative measure of fat proton signal, whereas histopathology measures intravesicular fat component directly. In this study, we kept the MR fat fraction threshold as 10% for a head-to-head comparison, and found that results did not greatly vary, although the lower threshold and scale difference might lead to even more robust results in terms of NPV. With the results of our study and review of multiple previous retrospective studies mentioned above, we conclude that MR-based fat fraction imaging using the Dixon method can be used for hepatic steatosis calculation in potential liver transplant donors, obviating the need for biopsy in most if not all patients. Patients with higher graft parenchymal percentage detected by MRI (above the institutional threshold) may benefit from dietary modifications and have repeat MRI-based calculations done instead of subjecting them to repeat biopsies. Thus, MRI can be used to completely obviate the need for invasive biopsy in most potential liver donors for liver steatosis quantification.
The major limitation of this study is its retrospective data collection. Although data were collection from 2 institutes, it was done sequentially due to the liver transplant team moving from one institute to the other. Hence, the surgical team and protocol were similar. However, it did have the advantage of using different MRI scanners and confirming reproducibility. The other limitations were small, but the variable time gap between MRI and intraoperative biopsy could have resulted in a slight change in fat percentage. However, in practical real-life settings, such a time gap is to be expected and may give a fair assessment of the utility of imaging-based fat calculation in predicting intraoperative fat percentage. Complex techniques like multi-echo techniques and MR spectroscopy were not used, but would have the benefit of confirming the diagnostic accuracy and reproducibility of the present results obtained using the simpler method of dual-echo fat fraction imaging.
Conclusions
In conclusion, imaging-based hepatic steatosis assessment (CT-LAI and MR-FF imaging) correlated well with histopathological assessment in living donors for liver transplant. The MRI Dixon-based fat quantification calculation displayed near-perfect negative predictive values and very high diagnostic accuracy, suggesting that it can obviate the need for biopsy in such patients with graft fat percentage <10% on MRI. The result can be verified with few large-volume multi-center studies and can help avoid invasive biopsy altogether in these patients.
Tables
Table 1. Demographic distribution of cohort of study subjects.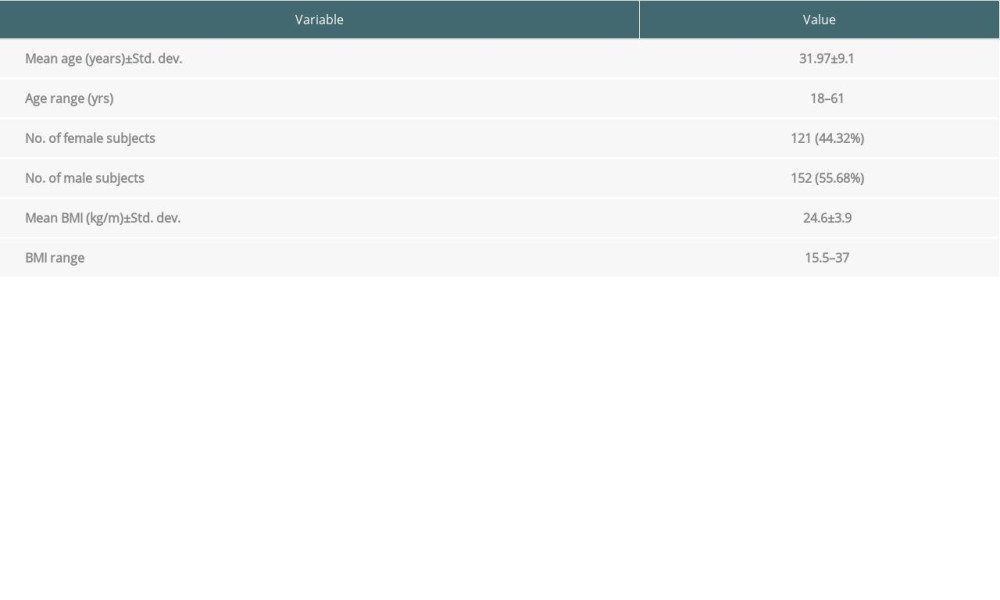 Table 2. Inter-rater kappa agreement of CT-LAI and biopsy-macrosteatosis (%).
Table 2. Inter-rater kappa agreement of CT-LAI and biopsy-macrosteatosis (%).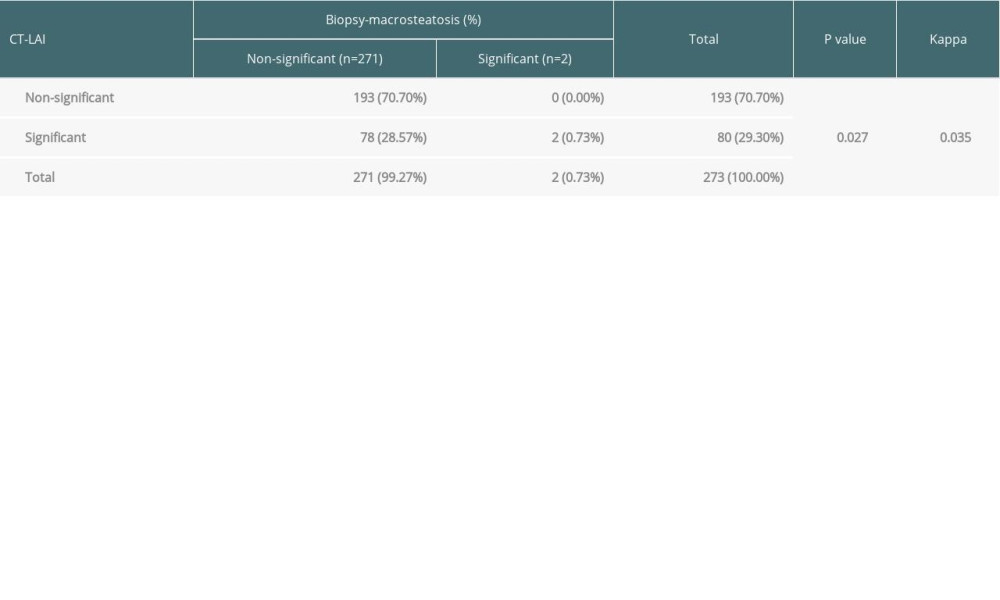 Table 3. Inter-rater kappa agreement of MRCP fat (%) and biopsy-macrosteatosis (%).
Table 3. Inter-rater kappa agreement of MRCP fat (%) and biopsy-macrosteatosis (%).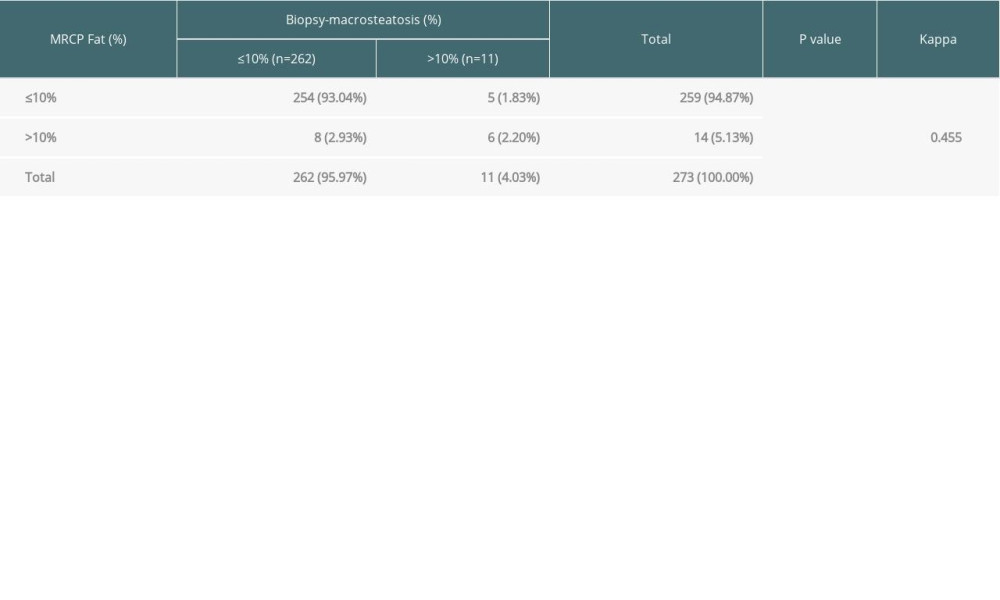 Table 4. Sensitivity, specificity, PPV, and NPV of MRCP fat (%) and CT-LAI for predicting significant fat.
Table 4. Sensitivity, specificity, PPV, and NPV of MRCP fat (%) and CT-LAI for predicting significant fat.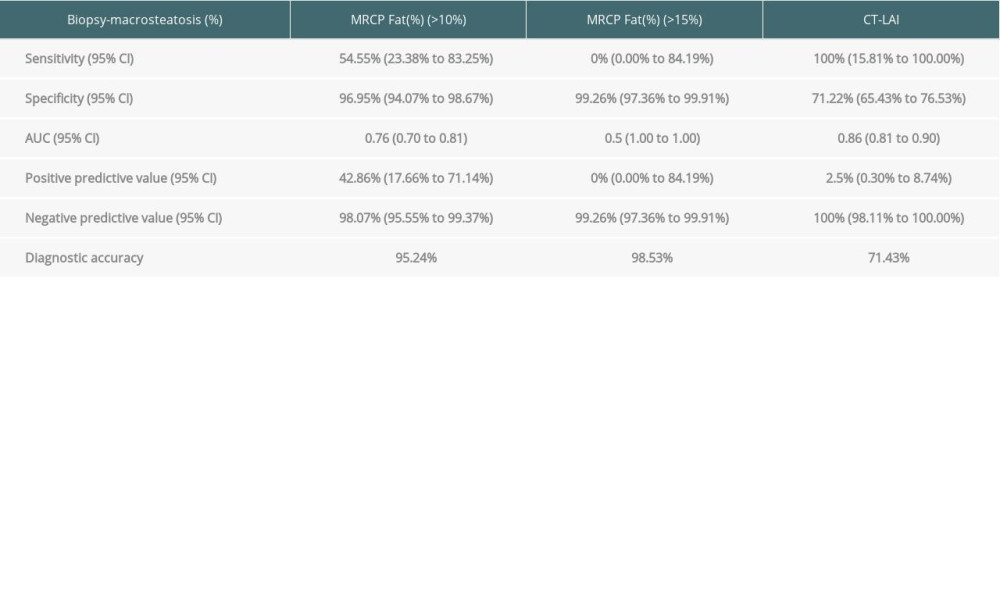 Table 5. Correlation of CT-LAI, MRCP fat (%) and biopsy-macrosteatosis (%) with each other.
Table 5. Correlation of CT-LAI, MRCP fat (%) and biopsy-macrosteatosis (%) with each other.
References
1. De Villa VH, Lo CM, Chen CL, Ethics and rationale of living-donor liver transplantation in Asia: Transplantation, 2003; 75(3); S2-5
2. Shin M, Song S, Kim JM, Donor morbidity including biliary complications in living-donor liver transplantation: Single-center analysis of 827 cases: Transplantation, 2012; 93(9); 942-48
3. Rudow DL, Brown RS, Emond JC, One-year morbidity after donor right hepatectomy: Liver Transplantation, 2004; 10(11); 1428-31
4. Yamamoto K, Takada Y, Fujimoto Y, Nonalcoholic steatohepatitis in donors for living donor liver transplantation: Transplantation, 2007; 83(3); 257-62
5. Perez-Daga JA, Santoyo J, Suarez MA, Influence of degree of hepatic steatosis on graft function and postoperative complications of liver transplantation: In Transplant Proc, 2006; 38(8); 2468-70
6. Andert A, Ulmer TF, Schöning W, Grade of donor liver microvesicular steatosis does not affect the postoperative outcome after liver transplantation: Hepatobiliary Pancreat Dis Int, 2017; 16(6); 617-23
7. Westerkamp AC, de Boer MT, van den Berg AP, Similar outcome after transplantation of moderate macrovesicular steatotic and nonsteatotic livers when the cold ischemia time is kept very short: Transpl Int, 2015; 28(3); 319-29
8. Deroose JP, Kazemier G, Zondervan P, Hepatic steatosis is not always a contraindication for cadaveric liver transplantation: HPB (Oxford), 2011; 13(6); 417-25
9. Nagai S, Fujimoto Y, Kamei H, Mild hepatic macrovesicular steatosis may be a risk factor for hyperbilirubinaemia in living liver donors following right hepatectomy: Br J Surg, 2009; 96(4); 437-44
10. Sharma A, Ashworth A, Behnke M, Donor selection for adult-to-adult living donor liver transplantation: well begun is half done: Transplantation, 2013; 95(3); 501
11. Bohte AE, van Werven JR, Bipat S, Stoker J, The diagnostic accuracy of US, CT, MRI and 1 H-MRS for the evaluation of hepatic steatosis compared with liver biopsy: Aa meta-analysis: Eur Radiol, 2011; 21(1); 87-97
12. Satkunasingham J, Hosseini Nik H, Fischer S, Can negligible hepatic steatosis determined by MRI-proton density fat fraction obviate the need for liver biopsy in potential liver donors: Liver Transpl, 2018; 24(4); 470-77
13. Ma X, Holalkere NS, Mino-Kenudson M, Imaging-based quantification of hepatic fat: Methods and clinical applications: Radiographics, 2009; 29(5); 1253-77
14. Rastogi R, Gupta S, Garg B, Comparative accuracy of CT, dual-echo MRI and MR spectroscopy for preoperative liver fat quantification in living related liver donors: Indian J Radiol Imaging, 2016; 26(1); 5-14
15. Hwang I, Lee JM, Lee KB, Hepatic steatosis in living liver donor candidates: Preoperative assessment by using breath-hold triple-echo MR imaging and 1H MR spectroscopy: Radiology, 2014; 271(3); 730-38
16. Yoon JH, Lee JM, Suh KS, Combined use of MR fat quantification and MR elastography in living liver donors: Can it reduce the need for preoperative liver biopsy?: Radiology, 2015; 276(2); 453-64
Figures
Tables
Table 1. Demographic distribution of cohort of study subjects.Table 2. Inter-rater kappa agreement of CT-LAI and biopsy-macrosteatosis (%).Table 3. Inter-rater kappa agreement of MRCP fat (%) and biopsy-macrosteatosis (%).Table 4. Sensitivity, specificity, PPV, and NPV of MRCP fat (%) and CT-LAI for predicting significant fat.Table 5. Correlation of CT-LAI, MRCP fat (%) and biopsy-macrosteatosis (%) with each other.Table 1. Demographic distribution of cohort of study subjects.Table 2. Inter-rater kappa agreement of CT-LAI and biopsy-macrosteatosis (%).Table 3. Inter-rater kappa agreement of MRCP fat (%) and biopsy-macrosteatosis (%).Table 4. Sensitivity, specificity, PPV, and NPV of MRCP fat (%) and CT-LAI for predicting significant fat.Table 5. Correlation of CT-LAI, MRCP fat (%) and biopsy-macrosteatosis (%) with each other. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988