06 June 2023: Original Paper
Results of Liver Retransplantation After Rescue Hepatectomy: A Single-Center Study
Erika LaineDOI: 10.12659/AOT.939557
Ann Transplant 2023; 28:e939557






Abstract
BACKGROUND: Liver retransplantation (reLT) is a well-accepted treatment for liver graft failure in selected patients. A rescue hepatectomy (RH), on the contrary, is a rare and controversial procedure in which a deteriorating liver graft causing failure of other organ systems is removed to stabilize the patient’s condition before a new liver graft is available.
MATERIAL AND METHODS: In this retrospective cohort study, we evaluated the outcomes of the 104 patients who were listed for a first single-organ reLT in our center during the period 2000-2019, to compare the results after RH to other reLTs.
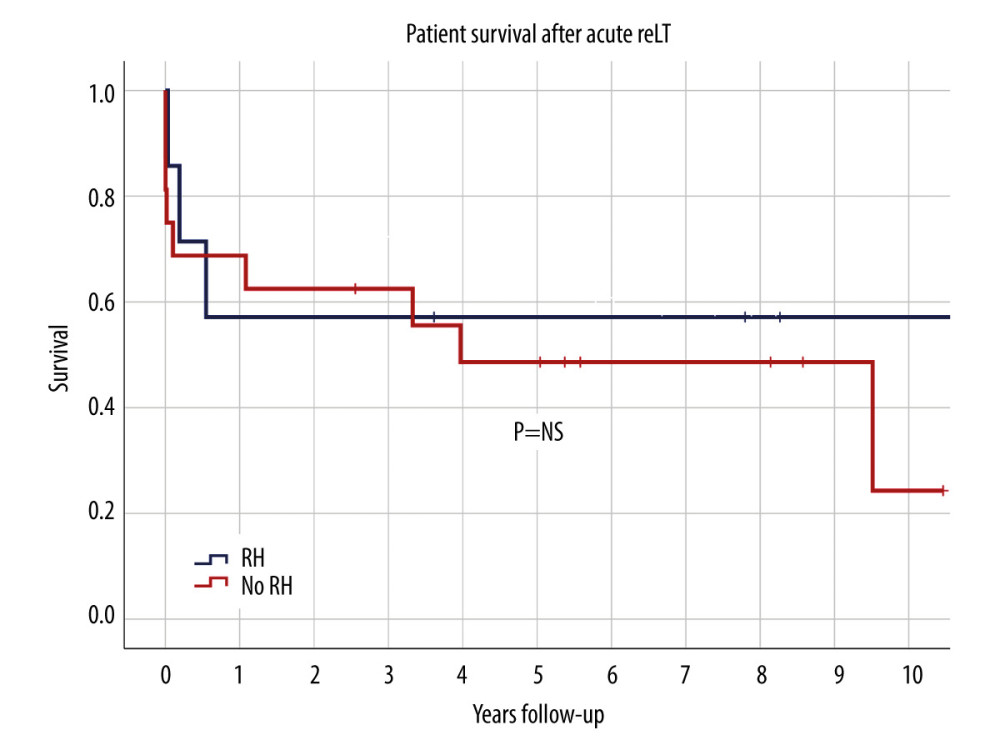
RESULTS: In the study population, RH was performed on 8 patients, while 7 of these received a new graft (8% of all first time reLTs) and 1 died before reLT. All RHs were performed within 1 week after the first transplantation. The median anhepatic time after RH was 36 hours (range 14-99). The 1-year patient survival rate was 57% for reLTs with RH and 69% for acute reLTs without RH that were performed within 14 days after the first transplantation (P=0.66). The 5-year survival rate was 50% in the RH and 47% in the non-RH group (P=1.0).
CONCLUSIONS: The use of RH prior to reLT results in a similar outcome to reLTs without RH. Therefore, RH should be considered in patients with a severe clinical instability caused by a deteriorating liver graft. However, further studies are needed to establish guidelines based on objective parameters for when RH should be performed.
Keywords: Liver Transplantation, Hepatectomy, Survival, Humans, Reoperation, Retrospective Studies, Risk Factors, Liver Diseases
Background
The most common indications for liver retransplantation (reLT) early after first liver transplantation (fLT) are primary non-function (PNF) and thrombovascular complications, whereas recurrence of primary disease, chronic rejection, and biliary complications account for the majority of late reLTs [1–5]. In cases of PNF and other causes for early failure of the liver graft, the deterioration of liver function is rapid, and it may also result in severe dysfunction of other organ systems, leading to hemodynamic instability, multi-organ failure and, eventually, the patient’s death [6]. The deteriorating liver graft not only fails to serve its metabolic function but also produces and leaks toxic substances to the patient’s circulation and is thus called toxic liver syndrome [7]. Occasionally, the need for acute removal of the liver graft is so evident that surgeons may decide to perform a rescue hepatectomy (RH) as a first part of a 2-stage reLT procedure, in which the deteriorating first graft is removed before a new graft is available [8]. In RH, a temporary portocaval shunt is established to achieve sufficient circulatory and clinical stabilization so that the patient can be further managed in an intensive care unit (ICU) while waiting for a new liver graft, and enormous intensive care efforts are required to maintain the patient in a prolonged anhepatic state. Thus, RH is an uncommon procedure performed only in critical situations when other options are few, and there are only a few studies, mainly case reports, describing its role before retransplantation [8–17]. Furthermore, there have been few reports on results after a RH compared to a standard acute reLT, and it is unknown whether RH before reLT affects the long-time outcome. In this study, we analyzed the liver retransplantations performed in our center in the past 2 decades to evaluate the impact of RH on the long-term results.
Material and Methods
STUDY POPULATION:
A retrospective cohort study was performed on patients who were listed for their first reLT at Karolinska University Hospital in Stockholm between January 2000 and December 2019. Patients who had undergone their first transplantation at other hospitals or had received a multi-organ transplantation, either previously or at the same time as reLT, were excluded from the study.
RHs were then identified by assessing the operation journals of patients with an AHT exceeding 3 hours. As there are no commonly defined indications when RH should be performed, decisions to perform RH in our patients were made by the responsible surgeon, with support from other members of the transplant team, on a case-by-case basis. The most important driving factors in the surgeon’s decision to perform RH were the dynamics of respiratory, circulatory, and metabolic deterioration in each patient. The key aspect considered was whether leaving the deteriorating liver graft in the recipient would worsen the patient’s general status within hours to such a degree that the patient would have to be removed from the waiting list (WL) for reLT. In most cases, the decision to perform RH was made before receiving information about the availability of a new liver graft. To identify a control group for the patients who underwent a RH, the patients without RH were divided into 3 groups: acute (within 2 weeks days after fLT), early (between 2 weeks and 3 months), and late (after 3 months), based on the timing of their reLT.
DATA COLLECTION:
Data were collected from the local liver transplantation registry (Ekvator) and supplemented with information from patients’ medical records when needed. Missing data were added using the Scandiatransplant database for organ transplantation (YASWA). The collected data contained characteristics of recipients and donors, as well as perioperative variables from both the recipient and the donors for both the primary transplantation and the retransplantation. Recipient variables included age, sex, weight, body mass index (BMI), primary diagnosis, model for end-stage liver disease (MELD) score prior to fLT and reLT, and date and cause of death. Liver graft function was assessed based on daily standard liver blood tests, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), international normalized ratio (INR), bilirubin, and platelet count (PLT) preoperatively and 3 months, 1 year, and 5 years after retransplantation. The data also included whether a patient had had a biliary or vascular complication or kidney failure requiring permanent renal replacement therapy with dialysis or kidney transplantation during the follow-up. Donor variables included age, sex, weight, BMI, length of ICU stay prior to donation, cause of death, and last available ALT, AST, and bilirubin before donation. The perioperative variables included type of graft (whole liver or living/reduced/split liver), operating time, cold and warm ischemia time, intraoperative bleeding, perioperative blood transfusions, and anhepatic time (AHT). For patients undergoing RH, we collected data on the postoperative day when RH was performed, and if the molecular adsorbent recirculation system (MARS) was used prior to or during AHT.
STATISTICAL ANALYSIS:
Data are mainly presented as a median (range). The
Results
OUTCOME AFTER RETRANSPLANTATION:
All patients with RH survived the reLT operation, while there was 1 intraoperative death (6.3%) in the acute reLT group without RH. The total perioperative mortality for acute reLTs was 17.4%, with 1 death (14.3%) in the RH group and 3 in the non-RH group (18.8%). In the RH group, 1- and 5-year patient survival was 57.1% and 50%, respectively (Figure 1). In the group of acute reLTs without RH, the 1-year patient survival was 68.8% and the 5-year survival 46.7% (P=0.657 and P=1.0, respectively). The most common causes of death were infections (50%) followed by bleeding complications (25%). There were no differences in laboratory test values or incidence of complications (Table 3) between the groups. None of the acutely retransplanted patients underwent a third liver transplantation during the follow-up, graft survival thus equaling patient survival in both the RH and non-RH group.
Discussion
This retrospective study was conducted to gain more insight into RH and outcome after 1 in the context of reLT. To the best of our knowledge, this is the first cohort study comparing long-term results after RH vs results of other reLTs.
RH has been suggested as a bridging procedure before a liver transplantation when a patient’s life is threatened by toxicity caused by the failing liver or exsanguination from the liver [8]. As there are no established policies with standardized indications and objective parameters for when RH should be performed, the decision to perform a RH is still made by individual surgeons in each case, which leads to very subjective decision-making relying on the surgeon’s experience and difficulties comparing different cases with each other. The exact decision-making process in each case was also difficult to analyze due to the retrospective nature of our study. However, in many cases, factors such as high lactate values and need for several vasopressors with a maximal dosage played an important role in it. Nevertheless, we would like to stress that the decision of performing RH, at least in our study population, is made in emergency situations where other measures have been deemed insufficient and the prognosis extremely poor. The question of whether hepatectomized patients would have a different outcome without a RH is difficult to answer. In our study, the only RH patient who died before reLT had a relatively long AHT of 41 h compared to many other reports [9,10,12–15]. However, there have been several patients surviving a longer anhepatic time with a good outcome, both in our study and in the literature [9,11,16,17]. It is also difficult to determine a time limit between AHT and reLT beyond which reLT may be considered futile, both due to lack of data on the subject and variability in the deterioration of a patient’s condition from case to case [18]. As RHs were performed within the first 14 days after the fLT, all RH patients qualified for an “urgent call” within Scandiatransplant [19]. The average waiting time on the urgent call WL is relatively short, supported by the fact that only 1 patient (12.5%) died before a new graft was available. That is comparable to mortality for non-RH patients on the same WL in our study and, for example, to the mortality on the Eurotransplant’s urgent and United Network for Organ Sharing status 1a WL [20,21]. Thus, from the organ availability point of view, RH should be considered a feasible alternative, as the organ supply in critical situations is relatively good, at least in these areas. Furthermore, the number of deaths on the WL has not increased over the studied period, although the number of reLTs has been rising, which also seems to be a trend in the Nordic countries [22].
The small number of patients made it difficult to perform any further subgroup analyses, including analyzing pediatric patients as a separate group. The small sample size – 87 retransplanted patients and only 8 patients with RH during the 20-year study period – is undeniably the main limitation of this study. All conclusions should therefore be tentative. Nevertheless, RH did not seem to affect the outcome in our patients. The long-term survival after reLTs with a prior RH is the same as the results of other acute reLTs, and can therefore be regarded as good, which indirectly validates RH as an emergency alternative in unstable patients with questionable graft viability and function and who do not respond to other treatments.
Conclusions
The use of RH prior to reLT results in the same patient survival rate as acute reLTs without RH. RH should therefore be considered in patients with deterioration of the first liver graft and with clinical instability. However, further studies are needed to establish guidelines based on objective parameters for when RH should be performed.
References
1. Kitchens WH, Yeh H, Markmann JF, Hepatic retransplant: What have we learned?: Clin Liver Dis, 2014; 18(3); 731-51
2. Zarrinpar A, Hong JC, What is the prognosis after retransplantation of the liver?: Adv Surg, 2012; 46; 87-100
3. Berumen J, Hemming A, Liver retransplantation: How much is too much?: Clin Liver Dis, 2017; 21(2); 435-47
4. Jeffrey AW, Delriviere L, McCaughan G, Excellent contemporary graft survival for adult liver retransplantation: An Australian and New Zealand registry analysis from 1986 to 2017: Transplant Direct, 2019; 5(8); e472
5. Takagi K, Domagala P, Porte RJ, Liver retransplantation in adult recipients: Analysis of a 38-year experience in the Netherlands: J Hepatobiliary Pancreat Sci, 2020; 27(1); 26-33
6. Masior Ł, Grąt M, Primary non-function and early allograft dysfunction after liver transplantation: Dig Dis, 2022; 40(6); 766-76
7. Dar WA, Sullivan E, Bynon JS, Ischaemia reperfusion injury in liver transplantation: Cellular and molecular mechanisms: Liver Int, 2019; 39(5); 788-801
8. Ringe B, Pichlmayr R, Lübbe N, Total hepatectomy as temporary approach to acute hepatic or primary graft failure: Transplant Proc, 1988; 20(Suppl 1); 552-57
9. Oldhafer KJ, Bornscheuer A, Frühauf NR, Rescue hepatectomy for initial graft non-function after liver transplantation: Transplantation, 1999; 67(7); 1024-28
10. Montalti R, Busani S, Masetti M, Two-stage liver transplantation: an effective procedure in urgent conditions: Clin Transplant, 2010; 24(1); 122-26
11. Arora H, Thekkekandam J, Tesche L, Long-term survival after 67 hours of anhepatic state due to primary liver allograft nonfunction: Liver Transpl, 2010; 16(12); 1428-33
12. Ringe B, Lübbe N, Kuse E, Total hepatectomy and liver transplantation as two-stage procedure: Ann Surge, 1993; 218(1); 3-9
13. Singh N, Washburn K, Schenk A, Rescue hepatectomy and anhepatic phase management after primary nonfunction in a liver transplant: Exp Clin Transplant, 2022; 20(8); 776-79
14. Bustamante M, Castroagudín JF, Gonzalez-Quintela A, Intensive care during prolonged anhepatic state after total hepatectomy and porto-caval shunt (two-stage procedure) in surgical complications of liver transplantation: Hepatogastroenterology, 2000; 47(35); 1343-46
15. Frank PN, Sharma VV, Gereboff A, Hepatitis B immunoglobulin-induced hypercoagulability complicating liver transplantation necessitating ECMO, rescue hepatectomy, and retransplantation: J Clin Anesth, 2018; 44; 64-65
16. Hammer GB, So SK, Al-Uzri A, Continuous venovenous hemofiltration with dialysis in combination with total hepatectomy and portocaval shunting. Bridge to liver transplantation: Transplantation, 1996; 62(1); 130-32
17. Ringe H, Henning S, Herre S, Seven day anhepatic survival in a 19-month-old child: An interdisciplinary challenge: Archives of Pediatric Surgery, 2019; 3(1); 39-44
18. Biggins SW, Futility and rationing in liver retransplantation: When and how can we say no?: J Hepatol, 2012; 56(6); 1404-11
19. , Liver exchange and pay back rules [Internet]: Scandiatransplant, 2021 [Cited 2022 Jul 12]. Available from: http://www.scandiatransplant.org/organ-allocation/NLTG_Exchange_payback_rules_Nov_2021.pdf/view
20. de Boer JD, Braat AE, Putter H, Outcome of liver transplant patients with high urgent priority: Are we doing the right thing?: Transplantation, 2019; 103(6); 1181-90
21. Wood NL, VanDerwerken DN, King EA, Life expectancy without a transplant for status 1A liver transplant candidates: Am J Transplant, 2022; 22(1); 274-78
22. Melum E, The Nordic liver transplant registry: Annual report 2021 [Internet]: Scandiatransplant, 2022; e939557-7 [cited 2022 Jul 7]. Available from: http://www.scandiatransplant.org/members/nltr/TheNordicLiverTransplantRegistryANNUALR EPORT2021.pdf
Tables
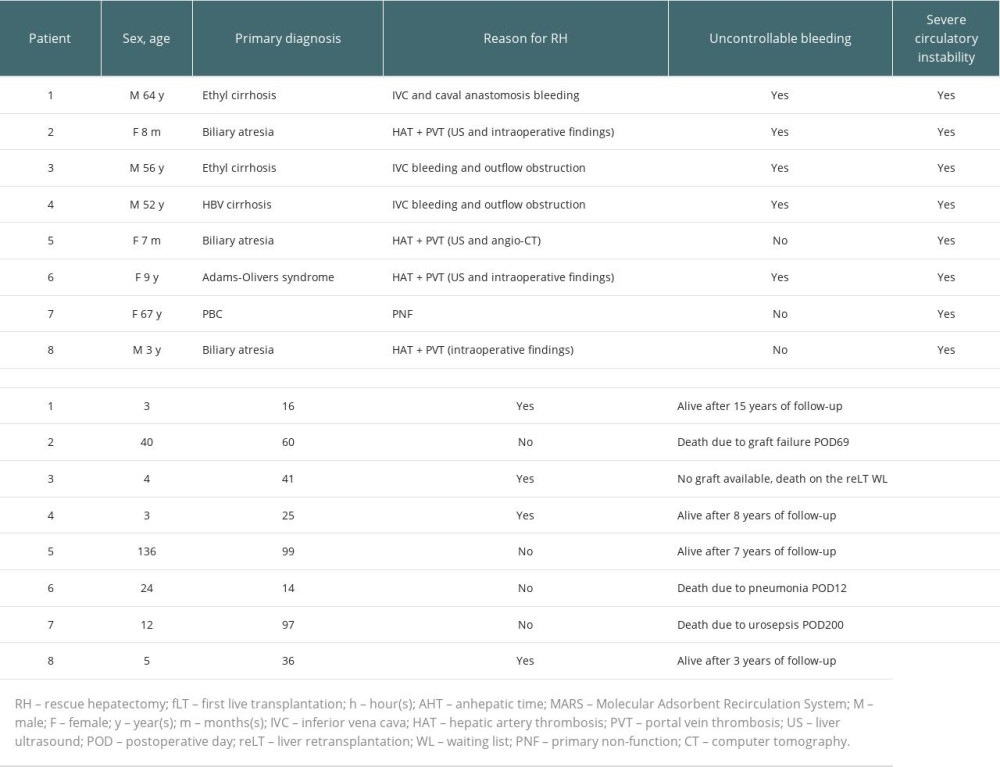 Table 1. Patients who underwent RH.
Table 1. Patients who underwent RH.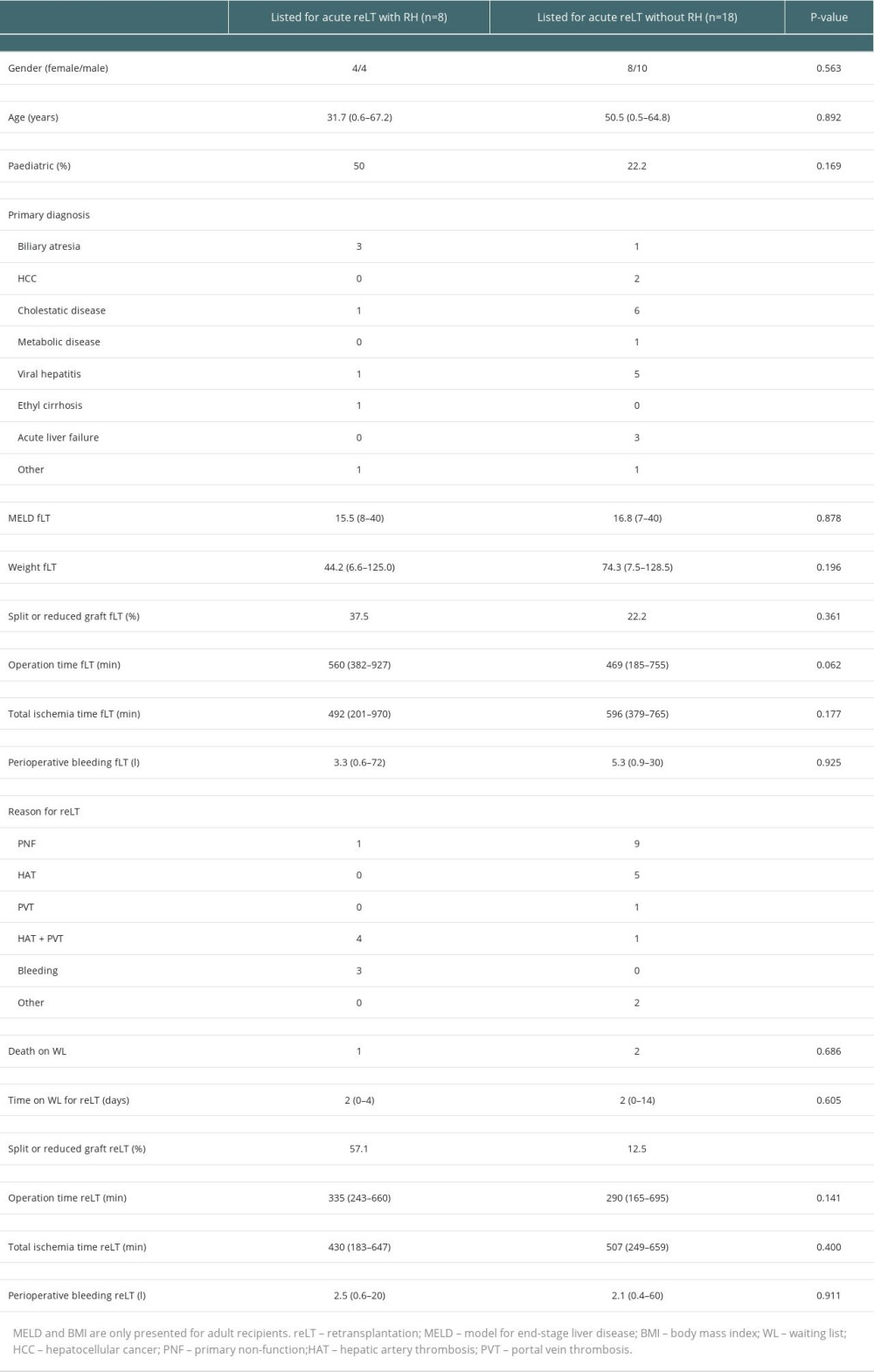 Table 2. Characteristics of patients who were listed for acute reLT with and without RH.
Table 2. Characteristics of patients who were listed for acute reLT with and without RH.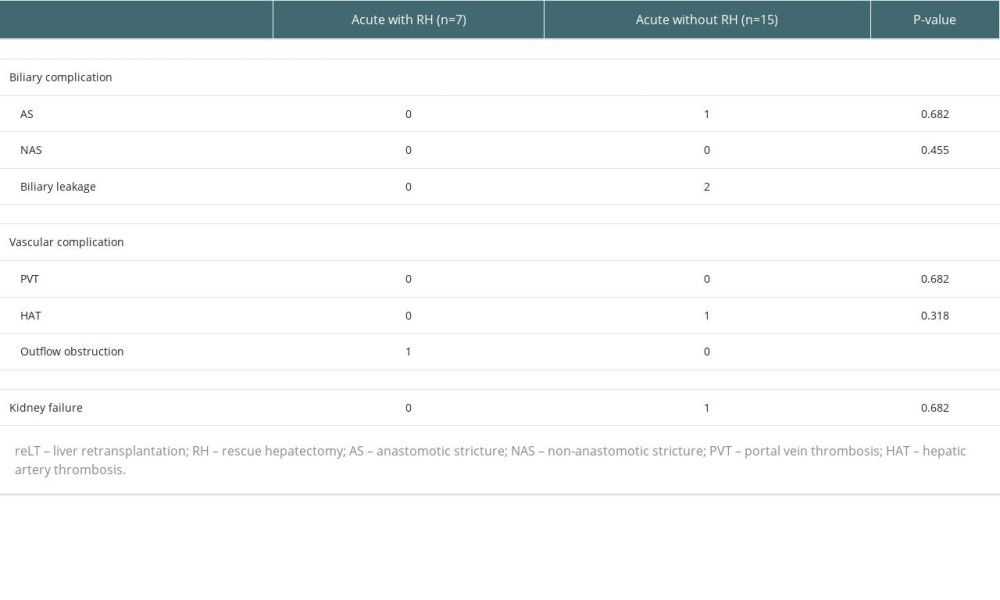 Table 3. Complications after acute reLT.Table 1. Patients who underwent RH.Table 2. Characteristics of patients who were listed for acute reLT with and without RH.Table 3. Complications after acute reLT.
Table 3. Complications after acute reLT.Table 1. Patients who underwent RH.Table 2. Characteristics of patients who were listed for acute reLT with and without RH.Table 3. Complications after acute reLT. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988