09 July 2024: Original Paper
Impact of Recipient and Donor Body Mass Index on Survival Outcomes After Intestinal Transplantation: A United Network for Organ Sharing Database Analysis
Prince Addo AmeyawDOI: 10.12659/AOT.943994
Ann Transplant 2024; 29:e943994






Abstract
BACKGROUND: Long-term patient survival after intestinal transplantation (IT) remains low compared with other organ transplants despite years of advancement in clinical experience. While patients with extremely high or low body mass index (BMI) are often considered ineligible for IT, the impact of BMI on post-transplant IT survival remains understudied.
MATERIAL AND METHODS: Using the United Network for Organ Sharing Standard Transplant database, we conducted a retrospective cohort study on patients who underwent IT between April 11, 1994, and September 29, 2021. We assessed the association of recipient and donor BMI at transplant with post-transplant mortality using Kaplan-Meier survival curves and univariate and multivariate Cox regression analyses.
RESULTS: A total of 1541 patients were included in our final sample. Of these patients, 806 were females (52.5%) and most were in the normal-weight BMI subgroup (54.2%). Obese class II (mean; 36.8±10.92 years) and underweight patients (mean; 37.6±13.37 years) were significantly younger than patients in other BMI categories. The adjusted multivariate model demonstrated an increased risk of mortality in underweight IT recipients compared to normal-weight IT recipients (aHR=1.25, 95% confidence interval [CI], 1.02-1.54; P=0.032).There was no significant association between donor BMI categories and survival in IT recipients.
CONCLUSIONS: Recipient BMI below normal is associated with an increased risk of mortality after intestinal transplantation and represents a potentially modifiable patient characteristic to improve survival outcomes.
Keywords: Obesity, transplant recipients, Survival Analysis, Body Mass Index, Intestine, Large, Intestine, Small, Humans, Female, Male, adult, Retrospective Studies, Intestines, Middle Aged, Databases, Factual, Tissue Donors, Tissue and Organ Procurement, Organ Transplantation, Survival Rate, United States
Introduction
The World Health Organization (WHO) defines obesity as abnormal or excessive fat accumulation, which poses a health risk. It is further classified into classes: class 1 (body mass index [BMI] ≥30.0–34.9 kg/m2), class 2 (BMI ≥35.0–39.9 9 kg/m2), and class 3 or severe (BMI ≥40.0 9 kg/m2) [1]. In the United States (US) the prevalence of obesity has been steadily increasing across all sexes, races, and ethnicities. According to data from the National Health and Nutrition Examination Survey, the prevalence of obesity in US adults increased from 30.5% in 1999–2000 to 42.4% in 2017–2018 [2,3].
Obesity is associated with multiple comorbidities, including cardiovascular, renal, non-alcoholic steatohepatitis, and metabolic syndrome, leading to end-organ dysfunction, which can impact surgical outcomes, including transplant outcomes [4,5]. Due to obesity-related complications, many transplant programs have listed class 2 obesity (BMI 35–39.9 kg/m2) and class 3 obesity (BMI greater than 40 kg/m2) as absolute or relative contraindication until patients undergo pre-transplant weight reduction [6]. This precaution aims to prevent post-transplant complications such as surgical site infections (SSIs), increased mortality rates, and graft failures [7]. Underweight patients face equally significant yet often less emphasized challenges. They are often plagued with comorbidities, including malignancies, metabolic and immunodeficiency diseases, which have a negative impact on postoperative outcomes. Further, underweight patients have higher risks of malnutrition, which places them at a significant risk of postoperative death and increased length of hospital stay [8–10]. While criteria to exclude transplant candidates with high BMI are commonly established, a corresponding low BMI threshold for patient exclusion remains less clearly defined.
Intestinal transplantation is a life-saving modality for patients with intestinal failure who have been non-responsive or developed life-threatening complications to parenteral nutrition [11]. There has been a gradual rise in intestinal transplantations in the US since 2019, with about 90 intestinal transplants performed annually [12]. In intestinal transplants, advancements in therapy have contributed to a decrease in mortality rates [11]. Despite these advances, long-term patient and graft survival remains substantially lower compared to other organ transplants, except for lung transplants [20], with all-cause mortality rates of nearly 44% at 5 years [13].
Despite its increasing utility and clinical advancements, the persistent suboptimal outcomes necessitate evaluation of additional modifiable predictors of survival. BMI remains an important yet understudied potential modifiable factor in post-transplant survival in intestinal transplantation.
However, only a few studies with very small sample sizes have explored this relationship [14,15]. Thus, this study aimed to investigate the impact of recipient and donor BMI on survival outcomes after intestinal transplantation using data from a national database.
Material and Methods
DATA SOURCE AND STUDY DESIGN:
We conducted a retrospective cohort study using data extracted from the Standard Transplant Analysis and Research (STAR) United Network for Organ Sharing (UNOS) database. The UNOS database is nationally representative and contains baseline demographic, clinical, and laboratory data of IT recipients from over 250 transplant centers in the US. We also retrieved data on donor information and post-transplant follow-up information on recipients. Our study was deemed exempt from consent requirements by the Institutional Review Board, as we used de-identified patient data.
STUDY POPULATION AND ANALYSIS:
The study population included adult patients (aged ≥18 years) who underwent their first IT from April 11, 1994, to September 29, 2021. We excluded patients with multiorgan transplants and those with missing data on BMI. The study’s main objective was to assess the association of recipient and donor BMI at transplant with increased post-transplant mortality. Recipient and donor BMIs were the primary variables of interest in our study. We categorized recipient and donor BMI into 6 main groups based on the World Health Organization BMI classes – underweight (BMI <18.5 kg/m2), normal weight (BMI 18.5–24.9 kg/m2; reference), overweight (BMI 25–29.9 kg/m2), obese class I (BMI 30–34.99 kg/m2), obese class II (BMI 35–39.99 kg/m2), and obese class III (BMI ≥40 kg/m2) [16].
We considered recipient demographic and clinical information for inclusion in the study analysis based on previous literature and/or plausibility [17,18]. These variables were: recipient’s self-reported race and ethnicity (classified as Non-Hispanic White, Non-Hispanic Black, Hispanic, Non-Hispanic Asian, and other/multiracial), recipient on life support (whether on 1 or more of extracorporeal membrane oxygen devices, artificial ventilation, prostaglandins, and inhaled nitrates), intensive care unit admission at transplant, serum creatinine (an indicator of kidney function), serum total bilirubin (an indicator of liver malfunction), and graft total ischemic time, which is the length of time between harvesting and reperfusion of the graft into a patient [19–21]. To account for historical bias, we categorized participants into 3 groups from different eras: 1994–2003, 2004–2013, and 2014–2021. For donor characteristics, we also explored variables found in prior studies to be independently associated with post-transplant mortality and included them in the multivariable model. The variables included were donor and recipient sex match, donor and recipient race match, and donor age.
Additionally, we considered the following recipient clinical variables for inclusion in our analysis: history of smoking or illicit drug use, history of pre-transplant malignancy, and history of diabetes or hypertension. On donor–recipient matching, we considered weight matching (donor–recipient weight ratio 0.8–1), Cytomegalovirus (CMV) mismatch (an IgG-positive donor CMV serology with a negative recipient CMV serology), ABO mismatch (donor and recipient with different ABO blood groups), and human leukocyte antigen mismatch (≥4 mismatched antigens).
We calculated means and standard deviations for continuous variables and computed percentages and standard deviations for categorical variables. Comparisons of donor and recipient demographic, clinical, and matching variables were made across the categories of BMI, using ANOVA for continuous variables and the χ2 test for categorical variables. Using Kaplan-Meier survival curves, we compared survival across different BMI categories and assessed for differences in survival using the log-rank test.
Univariate Cox regression analyses were utilized to compute crude hazard ratios for mortality across different BMI categories, with normal weight (BMI 18.5–24.9 kg/m2) as the reference group. Subsequently, multivariate Cox analysis was performed to estimate the hazard ratios of post-transplant survival across different BMI categories while adjusting for potential confounders (recipient race, recipient age, ICU stay, history of diabetes mellitus (DM), serum creatinine, serum bilirubin, total ischemic time, race match, and weight mismatch). A backward and forward selection method was used to select the final multivariable model. A
Results
Between April 11, 1994, and September 29, 2021, there were 1582 adults who received intestinal transplants. After exclusions for missing BMI data, the final analysis involved 1541 recipients categorized by BMI: underweight (N=220, 14.3%), normal weight (N=835, 54.2%), overweight (N=343, 22.3%), obese class I (N=90, 5.8%), obese class II (N=41, 2.7%), and obese class III (N=12, 0.8%) (Figure 1). Sex distribution across the categories showed a slight female predominance (52.5%), but the difference was not statistically significant (
The mean age of recipients was 41.3±13.21 years, with a significant difference across BMI categories (
Mean serum creatinine and bilirubin levels tended to increase with higher BMI categories, although serum bilirubin values showed no significant differences across BMI categories (
No significant differences were observed in pre-transplant malignancy (
From the Kaplan-Meier curves stratified by recipient BMI categories (Figure 2), underweight recipients showed lower survival rates across the study period. Survival curves for other recipient BMI categories were comparable, with no statistically significant differences in long-term survival. For donor BMI, Kaplan-Meier curves for post-transplant recipient mortality across categories of donor BMI did not significantly differ (log-rank
The Kaplan-Meier curves corresponded with results from the univariate Cox regression analysis (Table 4). For recipient BMI, underweight recipients had a significantly higher risk of post-transplant mortality (HR=1.269, 95% CI=1.045–1.542,
The multivariable analysis results are displayed in Tables 2 and 5. After adjusting for covariates, underweight recipients had 25% higher mortality compared to recipients within the normal-weight range (HR=1.25, 95% CI=1.02–1.54,
All donor BMI categories remained non-significant, after adjusting for variables in the multivariable analysis underweight (HR=1.07, 95% CI=0.87–1.33,
Discussion
There has been an overall steady increase in global intestinal transplant rates regionally since 1985, with North America accounting for 76% of this volume [23]. Despite the significant strides made through improved immunosuppression regimens resulting in reduced cellular rejection rates, aggressive approach to CMV and EBV disease prophylaxis, and improved surgical techniques [24], long-term patient and graft survival remains significantly lower compared to other organ transplants [25]. Despite improvement in some centers, overall post-transplant patient survival since 2000 remains at 58% and 47% at 5 and 10 years, respectively [23]. There is, therefore, a need to carefully select patients for improved outcomes. This study aimed to improve patient selection and optimization by investigating the impact of recipient and donor BMI on survival outcomes after intestinal transplantation.
In our study, recipient BMI below normal body weight was found to be detrimental to post-intestinal transplant survival outcomes, with a 29% increased risk of death compared to normal BMI. However, there was no statistically significant increase in mortality risk associated with the other BMI categories. This finding agrees with a retrospective study involving 94 patients who had undergone intestinal, multivisceral, and modified multivisceral transplantations in the United Kingdom, where poorer survival outcomes were noted in the underweight group, although it was not statistically significant [15]. Additionally, our findings were consistent with results from liver transplant studies [26,27]. Du et al found a relatively increased risk of mortality and hospital length of stay in underweight patients after liver transplantation [26]. Longer survival was also noted among overweight and obese patients after liver transplantation using data from UNOS [26]. A retrospective study utilizing the Scientific Registry of Transplant Recipient’s database found underweight recipients had higher risk of death than patients in other BMI classes, but the difference was not statistically significant (HR=1.28,
Patients who are underweight are often malnourished and have low functional status, which leads to increased hospital length of stay, mortality, and postoperative complications such as wound infections, respiratory infections, venous thromboembolism, and renal dysfunction [26,31]. Micronutrient deficiencies can worsen electrolyte abnormalities and increase vulnerability to refeeding syndrome, ileus, and cardiac arrhythmias [26]. Preoperative hypoalbuminemia is a strong predictor of morbidity and mortality in patients undergoing gastrointestinal surgeries [36]. Underweight surgical candidates have a low threshold to tolerate preoperative starvation and surgery-induced stress as a result of their underlying malnutrition [31]. Recipient characteristics shown in prior studies to be associated with increased mortality after organ transplantation include increasing age, diabetes mellitus, renal dysfunction, ICU stay, and longer total ischemic time [17,32,33]. The predictors of post-transplant mortality in our study were consistent with these known variables. However, after adjusting for these variables in our multivariate analysis, being underweight still remained significant and thus was an independent predictor of post-transplant mortality.
All donor BMI categories, as well as overweight and obese recipient BMI, were not associated with significantly higher mortality rates. Our findings of favorable survival outcomes in recipients with BMI in the overweight and obese categories may be explained by the obesity paradox, which has been demonstrated in hemodialysis and cardiovascular diseases [35,37]. In our context, overweight/obese patients may have better nutritional reserves, including lipid stores and muscle mass, compared to underweight recipients who might be having more severe forms of intestinal failure. Also, the relatively fewer recipients in the obesity classes 2 and 3 could have led to the underpowering of the outcome of interest. There is conflicting data on post-transplant survival outcomes and pre-transplant obesity in liver, lung, kidney, and heart transplantation [26–30,34]. In contrast to our findings, most of these studies found that recipient obesity was associated with poor survival outcomes [28–30]. Obesity and its well-documented health ramifications, including impaired pulmonary function, wound infection, metabolic syndrome, cardiovascular adverse events, and the increased technical difficulties of operating on obese patients, present unique challenges that can adversely affect post-transplant outcomes [35]. Class 2 and 3 obesity are listed as relative and absolute contraindications for certain organ transplants in the hope of achieving positive post-transplant survival outcomes and good stewardship of scarce donor organs [35].
Additional studies are needed to determine whether a recipient BMI below normal values should be considered a contraindication to intestinal transplantation. Our study provides evidence of the need to improve nutrition in the broad context of prehabilitation prior to intestinal transplantation to enhance survival outcomes. This will require a great deal of multidisciplinary effort, as most intestinal transplant candidates are patients with intestinal failure who have developed severe, intolerable complications of parenteral nutrition [11].
Although our study provides evidence that underweight BMI IT recipients have comparatively worse survival outcomes, limitations of the study should be considered when interpreting our study findings. First, the data in the UNOS dataset is retrospective and observational; therefore, conclusions from the study represent associations rather than causation. Also, peripheral edema and/or ascites are a consequence of hypoalbuminemia from malabsorption and malnutrition in patients with intestinal failure requiring IT. In such cases, a high BMI might be indicative of fluid overload rather than actual body fat, potentially leading to a misrepresentation of overweight or obesity in these groups. In addition, the study population was limited to patients considered to be eligible candidates for the transplant waitlist. It is possible that patients who had extremely high or low BMI were not included in this group, as they might have been excluded from the waitlist, and subsequently were not transplanted. This could result in a selection bias, where patients at the extremes of the BMI spectrum, potentially with other negative health factors, were not considered for analysis. This exclusion could have led to an underestimation of the variations in survival outcomes across different BMI categories in the study. Lastly, the study’s relatively small sample size, distributed across 6 BMI categories, might have restricted our ability to detect significant differences in survival benefits among the BMI groups.
Conclusions
Our study sought to examine the impact of BMI on survival outcomes in intestinal transplantation. Underweight recipients were found to have an increased risk of mortality after transplant. No significant mortality increase was associated with recipient BMI in the overweight and obesity categories, as well as all donor BMI categories. The knowledge that recipient BMI below normal range is an independent predictor of mortality and a potentially alterable pre-transplant characteristic can be acted upon to improve survival outcomes. Additional research is needed to improve patient selection through recipient nutritional optimization, rehabilitation, and identification of additional modifiable pre-transplant predictors of outcome.
Figures
 Figure 1. Relative percentage distribution of donor and recipient BMI categories. The figure depicts the comparative distribution of body mass index (BMI) categories among donors and recipients. Each BMI category is represented by a pair of bars, with blue color indicating the percentage distribution of recipients and the green color for donors. The categories displayed on the horizontal axis are ‘Underweight’, ‘Normal weight’, ‘Overweight’, ‘Obese Class I’, ‘Obese Class II’, and ‘Obese Class III’. The vertical axis represents the percentage distribution of each category. Figure created with RStudio 2023.03. 0-daily+82. pro2 for Windows 10+ (installer-less), PBC.
Figure 1. Relative percentage distribution of donor and recipient BMI categories. The figure depicts the comparative distribution of body mass index (BMI) categories among donors and recipients. Each BMI category is represented by a pair of bars, with blue color indicating the percentage distribution of recipients and the green color for donors. The categories displayed on the horizontal axis are ‘Underweight’, ‘Normal weight’, ‘Overweight’, ‘Obese Class I’, ‘Obese Class II’, and ‘Obese Class III’. The vertical axis represents the percentage distribution of each category. Figure created with RStudio 2023.03. 0-daily+82. pro2 for Windows 10+ (installer-less), PBC.  Figure 2. Survival curves by recipient BMI categories. Kaplan-Meier survival curves illustrating the survival probability over the follow-up period for recipients categorized by recipient BMI categories at the time of transplant. The categories are ‘Underweight’, ‘Normal weight’, ‘Overweight’, ‘Obese Class I’, ‘’Obese Class II’, and ‘Obese Class III’. Numbers at risk at various time points are displayed below the x-axis for each category. Figure created with RStudio 2023.03. 0-daily+82. pro2 for Windows 10+ (installer-less), PBC.
Figure 2. Survival curves by recipient BMI categories. Kaplan-Meier survival curves illustrating the survival probability over the follow-up period for recipients categorized by recipient BMI categories at the time of transplant. The categories are ‘Underweight’, ‘Normal weight’, ‘Overweight’, ‘Obese Class I’, ‘’Obese Class II’, and ‘Obese Class III’. Numbers at risk at various time points are displayed below the x-axis for each category. Figure created with RStudio 2023.03. 0-daily+82. pro2 for Windows 10+ (installer-less), PBC.  Figure 3. Survival curves by donor BMI categories. Kaplan-Meier survival curves illustrating the survival probability over the follow-up period for donors categorized by donor BMI categories at the time of transplant. The categories are ‘Underweight’, ‘Normal weight’, ‘Overweight’, ‘Obese Class I’, ‘’Obese Class II’, and ‘Obese Class III’. Numbers at risk at various time points are displayed below the x-axis for each category. Figure created with RStudio 2023.03. 0-daily+82. pro2 for Windows 10+ (installer-less), PBC.
Figure 3. Survival curves by donor BMI categories. Kaplan-Meier survival curves illustrating the survival probability over the follow-up period for donors categorized by donor BMI categories at the time of transplant. The categories are ‘Underweight’, ‘Normal weight’, ‘Overweight’, ‘Obese Class I’, ‘’Obese Class II’, and ‘Obese Class III’. Numbers at risk at various time points are displayed below the x-axis for each category. Figure created with RStudio 2023.03. 0-daily+82. pro2 for Windows 10+ (installer-less), PBC. Tables
Table 1. Demographic and clinical characteristics of intestinal transplant recipients by BMI category. Table 2. Multivariate Cox proportional hazards model for recipient BMI and other covariates in intestinal transplant survival analysis.
Table 2. Multivariate Cox proportional hazards model for recipient BMI and other covariates in intestinal transplant survival analysis. Table 3. Survival probabilities for recipient BMI.
Table 3. Survival probabilities for recipient BMI.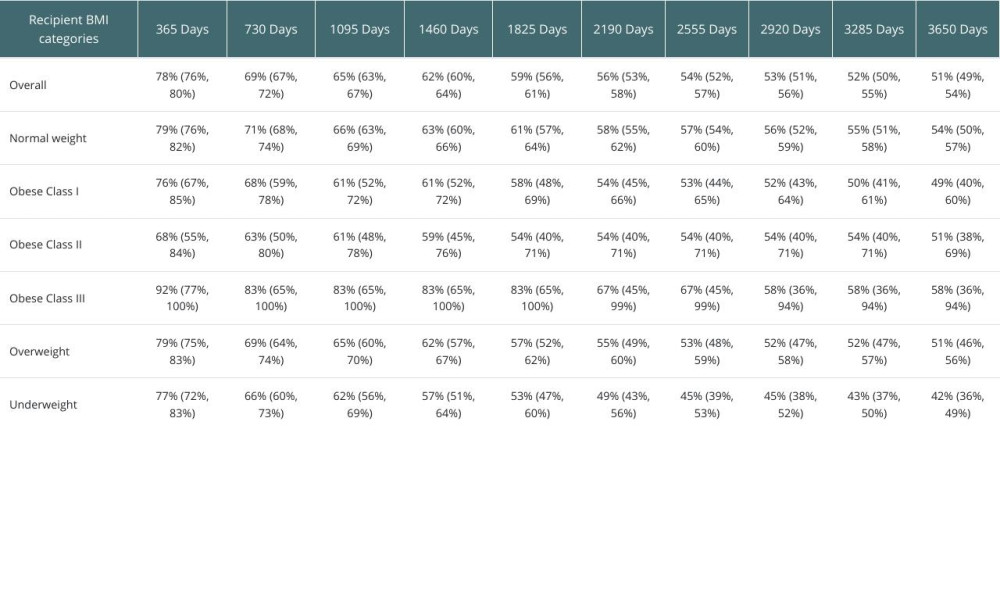 Table 4. Univariate Cox analysis- recipient and donor BMI categories.
Table 4. Univariate Cox analysis- recipient and donor BMI categories. Table 5. Multivariate Cox proportional hazards model for donor BMI and other covariates in intestinal transplant survival analysis.
Table 5. Multivariate Cox proportional hazards model for donor BMI and other covariates in intestinal transplant survival analysis.
References
1. World Health Organization, Obesity and Overweight: Fact Sheet Published 9 June 2021
2. Hales CM, Carroll MD, Fryar CD, Ogden CL, Prevalence of obesity and severe obesity among adults: United States, 2017–2018: NCHS Data Brief, 2020(360); 1-8
3. Hales CM, Carroll MD, Fryar CD, Ogden CL, Prevalence of obesity among adults and youth: United States, 2015–2016: NCHS Data Brief, 2017(288); 1-8
4. Scheuermann U, Babel J, Pietsch UC, Recipient obesity as a risk factor in kidney transplantation: BMC Nephrol, 2022; 23(1); 37
5. Foucher Y, Lorent M, Albano L, Renal transplantation outcomes in obese patients: A French cohort-based study: BMC Nephrol, 2021; 22(1); 79
6. Yemini R, Rahamimov R, Nesher E, The impact of obesity and associated comorbidities on the outcomes after renal transplantation with a living donor vs deceased donor grafts: J Clin Med May 29, 2022; 11(11); 3069
7. Winfield RD, Reese S, Bochicchio K, Obesity and the risk for surgical site infection in abdominal surgery: Am Surg, 2016; 82(4); 331-36
8. Cederholm T, Bosaeus I, Barazzoni R, Diagnostic criteria for malnutrition – An ESPEN Consensus Statement: Clin Nutr, 2015; 34(3); 335-40
9. Narendra K, Kiss N, Margerison C, Johnston B, Chapman B, Impact of nutritional status/risk and post-operative nutritional management on clinical outcomes in patients undergoing gastrointestinal surgery: A prospective observational study: J Hum Nutr Diet, 2020; 33(4); 587-97
10. GlobalSurg Collaborative and NIHR Global Health Unit on Global Surgery, Impact of malnutrition on early outcomes after cancer surgery: An international, multicentre, prospective cohort study: Lancet Glob Health, 2023; 11(3); e341-e49
11. Bharadwaj S, Tandon P, Gohel TD, Current status of intestinal and multivisceral transplantation: Gastroenterol Rep (Oxf), 2017; 5(1); 20-28
12. : OPTN/SRTR Annual Data Report, n.d Retrieved January 13, 2024, from: https://www.srtr.org/reports/optnsrtr-annual-data-report/
13. Cunha-Melo JR, Costa G, Intestinal transplantation: Evolution and current status: Medical Express (Sao Paulo, online), 2014; 1(6); 307-22
14. Yeap SP, Butler AJ, Russel NK, Impact of body mass index on survival after small intestinal and multivisceral transplantation: Clinical Nutrition ESPEN December; 22; p130-131
15. Yeap S, Hogg R, Allen E, The impact of body mass index on survival following intestinal and multivisceral transplantations in the United Kingdom: Transplantation, 2017; 101(6S2); S86
16. : Defining Adult Overweight & Obesity | Overweight & Obesity, n.d, CDC Retrieved January 13, 2024, from: https://www.cdc.gov/obesity/basics/adult-defining.html
17. Farmer DG, Venick RS, Colangelo J, Pretransplant predictors of survival after intestinal transplantation: Analysis of a single-center experience of more than 100 transplants: Transplantation, 2010; 90(12); 1574-80
18. Morris AA, Kransdorf EP, Coleman BL, Colvin M, Racial and ethnic disparities in outcomes after heart transplantation: A systematic review of contributing factors and future directions to close the outcomes gap: J Heart Lung Transplant, 2016; 35(8); 953-61
19. Lee J, Kim EJ, Lee JG, Clinical impact of serum bilirubin levels on kidney transplant outcomes: Sci Rep, 2021; 11(1); 6889
20. Kashani K, Rosner MH, Ostermann M, Creatinine: From physiology to clinical application: Eur J Intern Med, 2020; 72; 9-14 [Erratum in: Eur J Intern Med. 2023;116:168–69]
21. Ghaidan H, Fakhro M, Lindstedt S, Impact of allograft ischemic time on long-term survival in lung transplantation: A Swedish monocentric study: Scand Cardiovasc J, 2020; 54(5); 322-29
22. , Organ transplant statistics worldwide 2022: Statista, n.d Retrieved December 29, 2023, from: https://www.statista.com/statistics/398645/global-estimation-of-organ-transplantations/
23. Grant D, Abu-Elmagd K, Mazariegos GIntestinal Transplant Association, Intestinal transplant registry report: Global activity and trends: Am J Transplant, 2015; 15(1); 210-19
24. Hind JM, Long-term outcomes of intestinal transplantation: Curr Opin Organ Transplant, 2021; 26(2); 192-99
25. Horslen SP, Wood NL, Cafarella M, Schnellinger EM, OPTN/SRTR 2021 Annual Data Report: Intestine: Am J Transplant, 2023; 23(2 Suppl 1); S264-S99
26. Du AL, Danforth DJ, Waterman RS, Gabriel RA, Is obesity associated with better liver transplant outcomes? A retrospective study of hospital length of stay and mortality following liver transplantation: Anesth Analg, 2022; 135(1); 118-27
27. Pelletier SJ, Schaubel DE, Wei G, Effect of body mass index on the survival benefit of liver transplantation: Liver Transpl, 2007; 13(12); 1678-83
28. Doumouras BS, Fan CS, Mueller B, The effect of pre-heart transplant body mass index on posttransplant outcomes: An analysis of the ISHLT Registry Data: Clin Transplant, 2019; 33(7); e13621
29. Upala S, Panichsillapakit T, Wijarnpreecha K, Underweight and obesity increase the risk of mortality after lung transplantation: A systematic review and meta-analysis: Transpl Int, 2016; 29(3); 285-96
30. Ahmadi SF, Zahmatkesh G, Streja E, Body mass index and mortality in kidney transplant recipients: A systematic review and meta-analysis: Am J Nephrol, 2014; 40(4); 315-24
31. Yasunaga H, Horiguchi H, Matsuda S, Body mass index and outcomes following gastrointestinal cancer surgery in Japan: Br J Surg, 2013; 100(10); 1335-43
32. Foroutan F, Alba AC, Guyatt G, Predictors of 1-year mortality in heart transplant recipients: A systematic review and meta-analysis: Heart, 2018; 104(2); 151-60
33. Elsabbagh AM, Hawksworth J, Khan KM, Long-term survival in visceral transplant recipients in the new era: A single-center experience: Am J Transplant, 2019; 19(7); 2077-91
34. Lafranca JA, Jermans IJN, Betjes MG, Dor FJ, Body mass index and outcome in renal transplant recipients: A systematic review and meta-analysis: BMC Med, 2015; 13; 111 [Erratum in: BMC Med. 2015;13:141]
35. Diwan TS, Lee TC, Nagai S, Obesity, transplantation, and bariatric surgery: An evolving solution for a growing epidemic: Am J Transplant, 2020; 20(8); 2143-55
36. Petch-In P, Saokaew S, Phisalprapa P, Dilokthornsakul P, The association of pre-operative serum albumin levels and post-operative in-hospital death in patients undergoing gastrointestinal surgeries in Thailand: A retrospective cohort study: Drugs Real World Outcomes, 2023; 10(2); 341-49
37. Tutor AW, Lavie CJ, Kachur S, Updates on obesity and the obesity paradox in cardiovascular diseases: Prog Cardiovasc Dis, 2023; 78; 2-10
Figures
Figure 1. Relative percentage distribution of donor and recipient BMI categories. The figure depicts the comparative distribution of body mass index (BMI) categories among donors and recipients. Each BMI category is represented by a pair of bars, with blue color indicating the percentage distribution of recipients and the green color for donors. The categories displayed on the horizontal axis are ‘Underweight’, ‘Normal weight’, ‘Overweight’, ‘Obese Class I’, ‘Obese Class II’, and ‘Obese Class III’. The vertical axis represents the percentage distribution of each category. Figure created with RStudio 2023.03. 0-daily+82. pro2 for Windows 10+ (installer-less), PBC.Figure 2. Survival curves by recipient BMI categories. Kaplan-Meier survival curves illustrating the survival probability over the follow-up period for recipients categorized by recipient BMI categories at the time of transplant. The categories are ‘Underweight’, ‘Normal weight’, ‘Overweight’, ‘Obese Class I’, ‘’Obese Class II’, and ‘Obese Class III’. Numbers at risk at various time points are displayed below the x-axis for each category. Figure created with RStudio 2023.03. 0-daily+82. pro2 for Windows 10+ (installer-less), PBC.Figure 3. Survival curves by donor BMI categories. Kaplan-Meier survival curves illustrating the survival probability over the follow-up period for donors categorized by donor BMI categories at the time of transplant. The categories are ‘Underweight’, ‘Normal weight’, ‘Overweight’, ‘Obese Class I’, ‘’Obese Class II’, and ‘Obese Class III’. Numbers at risk at various time points are displayed below the x-axis for each category. Figure created with RStudio 2023.03. 0-daily+82. pro2 for Windows 10+ (installer-less), PBC. Tables
Table 1. Demographic and clinical characteristics of intestinal transplant recipients by BMI category.Table 2. Multivariate Cox proportional hazards model for recipient BMI and other covariates in intestinal transplant survival analysis.Table 3. Survival probabilities for recipient BMI.Table 4. Univariate Cox analysis- recipient and donor BMI categories.Table 5. Multivariate Cox proportional hazards model for donor BMI and other covariates in intestinal transplant survival analysis.Table 1. Demographic and clinical characteristics of intestinal transplant recipients by BMI category.Table 2. Multivariate Cox proportional hazards model for recipient BMI and other covariates in intestinal transplant survival analysis.Table 3. Survival probabilities for recipient BMI.Table 4. Univariate Cox analysis- recipient and donor BMI categories.Table 5. Multivariate Cox proportional hazards model for donor BMI and other covariates in intestinal transplant survival analysis. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988