13 August 2024: Original Paper
Kidney After Lung Transplants or Combined Kidney–Lung Transplantation: A Single-Center Retrospective Cohort Study
Benoît Mesnard1ABCDEF*, Matthieu GlorionDOI: 10.12659/AOT.944049
Ann Transplant 2024; 29:e944049






Abstract
BACKGROUND: End-stage renal disease is a major issue in the management of patients undergoing lung transplantation. Combined kidney–lung transplantation (CKLT) and kidney after lung transplantation (KALT) are the 2 preferred solutions to manage this situation. To evaluate these strategies, we describe kidney and lung graft outcomes and patient survival in patients managed with CKLT and KALT.
MATERIAL AND METHODS: We conducted a retrospective single-center cohort study. Patients who underwent a CKLT or a KALT were included in this study. Retrospective extraction of data from medical records was performed.
RESULTS: Seventeen patients underwent CKLT and 9 underwent KALT. Most of the patients had cystic fibrosis and presented renal failure related to anti-calcineurin toxicity. The 30-day and 1-year survival of CKLT recipients were both 75.6%. No patients with KALT died during the follow-up. Kidney graft prognosis was almost exclusively influenced by patient survival in relation to postoperative lung transplant complications. The rate of severe surgical complications was close to 60% for CKLT compared with 30% for KALT. The kidney graft function (estimated kidney graft function) did not differ according to the transplantation strategy.
CONCLUSIONS: KALT is a safe option, with postoperative morbidity and renal graft function identical to those of kidney transplantation in non-lung-transplanted patients. The results of CKLT depend mainly on the morbidity associated with lung transplantation but remain an attractive option for patients with respiratory failure associated with end-stage renal disease. The choice of transplant strategy must also take into account the most ethical and efficient allocation of kidney grafts.
Keywords: Kidney Transplantation, Lung Transplantation, Intraoperative Complications, Postoperative Complications, Retrospective Studies, Humans, Male, Female, adult, Middle Aged, Kidney Failure, Chronic, Graft Survival, young adult, Treatment Outcome
Introduction
Patients with chronic respiratory failure (CRF) who have undergone lung transplantation (LT) or are enlisted in a program of LT may be affected by chronic kidney disease (CKD), and some will progress to end-stage renal disease (ESRD) [1,2]. First, their renal function is often overestimated by the routine use of serum creatinine to calculate their glomerular filtration rate (GFR) because creatinine is a muscle waste product; for example, patients affected by cystic fibrosis tend to have severe sarcopenia. Second, their GFR may be altered because of comorbidities affecting renal vessels (such as diabetes mellitus or chronic hypertension) [3]. Last, the sequence of LT begins with major thoracic surgery, which is a known risk factor for acute kidney injury (AKI), and AKI is a known risk factor for CKD, and continues with constant exposure to calcineurin inhibitors, the chronic toxicity of which is damages the kidneys, inducing arteriolar hyalinosis and interstitial fibrosis [1,4–7]. The incidence of ESRD is around 1–1.5% per year following non-renal solid organ transplantation, not only LT [1].
Over the last 20 years, the proportion of LT patients listed for a kidney transplantation (KT) has dramatically risen (+635% according to the UNOS database) [8]. This increase is also explained by very strong development of LT in the 1990s.
In the context of LT, CKD compromises the outcome at many levels. For some it is a relative contraindication to lung transplantation [9] because it facilitates fluid overload and hence pulmonary edema. It is associated with a significant increase in postoperative morbidity and mortality at 1 year [10,11]. Conversely, the survival benefit of KT over dialysis in the general population is also seen in LT patients, with a significant reduction in mortality that is maintained and even increased years after KT [12–14].
Assuming CKD has been properly identified and staged in a candidate for LT, a question will arise: what is the best timing for KT? Should it be straightforward, and the patient enlisted for a combined kidney–lung transplantation (CKLT)? Or should it be lung first, then kidney (kidney after lung transplantation, or KALT)? The literature is scarce regarding CKLT, consisting of only a few clinical cases [3] and 2 cohorts [15,16], represent altogether a total of less than 120 patients) and KALT [8,14]. Despite differences in the characteristics of the populations between these 2 patient groups, it seemed important for us to be able to describe the prognosis and outcomes associated with each of these procedures.
We evaluated the respective outcome of CKLT and of KALT in our center, a tertiary referral hospital with experience in both LT and KT. The primary objective was to describe kidney and lung graft outcomes and patient survival in lung recipients subjected to CKLT or KALT. The secondary objective was to analyze the surgical procedures and intra- and postoperative outcomes.
Material and Methods
INCLUSION CRITERIA:
Patients who underwent a CKLT or a KALT between 01/11/1988 and 1/07/2023 at Foch Hopital in Suresnes, France were included in this study. The only exclusion criterion was age <18 years.
DATA EXTRACTION:
A retrospective extraction of medical records was carried out on preoperative, intraoperative, and postoperative data and on the follow-up of recipients. Donor data were also collected. Surgical complications (morbidity and mortality) were defined into 5 classes according to the Clavien-Dindo classification [19]. Delayed graft function after KT was defined as the need for dialysis during the first postoperative week. Primary non-function was defined as permanent need for dialysis despite transplantation. Failure of KT was defined by the need for dialysis or for a new kidney transplant. Chronic lung allograft dysfunction (CLAD) has been defined as chronic rejection of the lung graft and included bronchiolitis obliterans syndrome, neutrophilic reversible allograft dysfunction, and restrictive allograft syndrome.
IMMUNOSUPPRESSION:
Induction of immunosuppression consisted in either an IL2R antagonist or a T-cell-depleting agent, followed by a maintenance regimen combining 3 drugs. The standard regimen combined a calcineurin inhibitor (tacrolimus), mycophenolate mofetil, and steroids. In the case of KALT, the current immunosuppression was simply continued after induction.
PRIMARY AND SECONDARY OUTCOMES:
The primary outcomes were renal and lung graft outcomes and patient survival after CKLT and KALT. The secondary objective was to compare surgical procedures and outcomes.
STATISTICAL ANALYSIS:
Statistical analyses were performed using Wizard software, v1.9.45. Continuous variables were expressed as median and interquartile range (IQR) and categorical variables were expressed as n and percentages. Univariate analyses were performed for continuous variables with Mann-Whitney test (independent data). Categorical data were compared with the chi-square test (independent data). Statistical significance was set at
Results
RECIPIENT AND DONOR CHARACTERISTICS:
The recipients were mainly women, with a median age of 35 years in the CKLT group and 45 in the KALT group. The indication for LT was cystic fibrosis in the vast majority of patients. CKLT was performed in patients with preoperative CKD not treated with dialysis. In contrast, 77% of KALT patients had started dialysis before the surgical procedure. Only 2 CKLT patients received mechanical assistance by extracorporeal membrane oxygenation prior to transplantation. All data are shown in Table 1. Most kidney donors were under age 40 years and had no comorbidities; 44% of donors for the KALT group were living donors (Table 2).
KIDNEY–LUNG TRANSPLANTATION AND EARLY POSTOPERATIVE MORBIDITY:
Except for 1 patient, KTs were always first renal transplants, engrafted in the iliac position. For CKLT, the median duration of cold ischaemia time (CIT) was 10.7 hours. For KALT, median CIT in deceased donor was 26.5 hours. For CKLT transplants, 64% of lung transplants were performed without circulatory support. Data are shown in Table 3.
CKLT patients were hospitalized for more than 2 weeks in the intensive care unit and stayed in the hospital for a median of 3 weeks. The length of hospital stay for KALT was significantly shorter (10 days, P<0.001). The rate of postoperative medical complications was higher in the CKLT group; most were non-severe complications (Clavien <3). There was 1 death related to Clostridium difficile colitis. The surgical complication rate was high in both groups (>50%), and higher in the CKLT group. However, these results were not statistically significant. In the KALT group, there were 2 early revisions for bleeding and 1 marsupialization at one and a half months due to a lymphocele. In the CKLT group, there were 6 revisions – 4 for the renal graft (lymphocele) and 2 for the lung graft. Three deaths occurred in the CKLT group due to surgical complications linked to the LT. All data are provided in Table 4.
LUNG AND KIDNEY GRAFT OUTCOMES:
The median follow-up was 40.5 months (Table 5). Two PNFs occurred in the CKLT group in patients who suffered from circulatory shock and subsequently died. Two patients in the CKLT group developed CLAD and 1 patient needed a third lung transplant (Figure 2). None of the patients who developed DGF were on dialysis prior to the operation. Except for kidney grafts that were lost following recipients’ death, no patient in the CKLT group returned to dialysis. Death-censored renal graft survival was 100% in the CKLT group and 89% in the KALT group (1 patient required a new transplant). Renal function was significantly better in the CKLT group than in the KALT group during the first year following KT, and thereafter they were comparable (Figure 2).
RECIPIENT’S SURVIVAL:
The 30-day and 1-year survival of CKLT recipients were both 75.6% (75% of deaths within the first month were first LT). Four CKLT recipients died within the initial 30-day period. The first patient died following postoperative multi-system failure characterized by hemorrhagic syndrome, severe infection, persistent candidemia, and inability to wean from ECMO. The second died following a presentation of hemorrhagic shock, followed by septic shock and diffuse colitis due to C. difficile. The third died due to profound vasoplegia associated with hemoptysis and hemothorax. The last patient died post-operatively due to cardiac arrest during the initiation of ECMO. Three of these deaths occurred during a primary lung transplantation and 1 during re-transplantation. Recipient survival at 5 years was 55.1%. There were no deaths during the follow-up of KALT recipients. All data are presented in Figure 3.
Discussion
Our study reports the outcomes of patients undergoing CKLT or KALT. Unlike previous studies published from national multicenter registries, our study is the first to report these results in a large single-center cohort, thus making it possible to expose the link between early postoperative complications and medium-term graft outcomes.
We observed that in CKLT, kidney graft prognosis was almost exclusively influenced by patient survival in relation to postoperative lung transplant complications. All losses of viable kidney grafts in the CKLT group in the early and the late postoperative period were associated with death of the recipient. There was no renal graft loss due to urological or nephrological complications. It is also important to note that DGF occurred in patients who had a pre-emptive kidney transplant. This highlights the impact of circulatory shock due to the LT both on the native kidneys and on the graft. Complications related to the kidney graft appeared to be identical to those found in large cohorts of isolated KT [20]. However, the rate of symptomatic lymphocele requiring drainage was high in the CKLT group (>20%). In our cohort, lymphocele has only been reported in patients with cystic fibrosis. In our opinion, this high occurrence of lymphocele may be linked to the variations in venous pressure during the postoperative period (with episodes of venous hyper-pressure that increases lymph production) and to malnutrition, which encourages the development of effusions. Finally, peritoneal fluid and ascites are commonly found in cystic fibrosis patients. We believe that these fluids may play a role and constitute postoperative collections that mimic or at least participate in the collection of lymphoceles. The outcomes for KALT appear to be similar to those available in the literature for isolated KT, in terms of both length of hospitalization and postoperative morbidity.
At 3 years, which is relatively short term, renal function in CKLT and KALT were identical. These data on CKLT are reassuring because the circulatory ordeal imposed by LT might have rapidly compromised renal graft function.
When discussing second or combined transplants, the question of ethics in relation to other patients on the waiting list must be considered. In our cohort, 4 kidney transplants (23.53%) were lost within the first 30 days in the CKLT group compared with 0 in the KALT group. We must also consider patients who have undergone lung transplantation, who were on the waiting list for a renal transplantation and died while on that list. In our center, over the last 30 years, 53 patients with a lung transplant have been placed on a renal transplantation waiting list. Among these 53 patients, 13 have died while on the waiting list, although it cannot be directly attributed to renal insufficiency. CKLT is an attractive treatment option for patients with combined respiratory and renal failure. Indeed, CKLT has been reported to reduce early and medium-term mortality compared with isolated LT in patients on dialysis or with renal function <30ml/min/1.73 m2 [16]. We are not aware of any strong preoperative or intraoperative criteria to contraindicate treatment with CKLT. In our cohort, all complications leading to death occurred after 48 hours of hospitalization, and surgery. We did not find an increased risk of early postoperative mortality in patients managed for a second LT or in whom it was necessary to introduce a circulatory assistance by extracorporeal membrane oxygenation.
Our institution has previously published its experience of first
To date, in our center, the indication for CKLT is validated during a multidisciplinary meeting. Our criteria are in line with international recommendations [23]. Patients awaiting LT are being offered a CKLT if they have stage 4 or 5 (ESRD) CKD. In patients with a stage 3B, a measured (as opposed to estimated) GFR, or a kidney biopsy, may help to refine the indication. These data are supported by the latest data presented by Chen et al [16], who reported a positive impact of CKTL compared with isolated LT on patients’ survival when eGFR is <30 ml/min/1.73 m2 or low enough to indicate renal replacement therapy. Osho et al demonstrated an increase in short- and medium-term mortality in the case of isolated LT in patients with an eGFR <40 mL/min/1.73 m2 compared with those above this threshold [24].
In our hospital, a living donor program is prioritized over that using kidneys from deceased donors, including when KALT is indicated. In our cohort, 44% of KALTs came from living donors [25]. In any case, iliac vessels must be preserved as soon as CKLT or KALT is envisaged. Patients with LT, particularly those with cystic fibrosis, frequently have a history of central venous lines insertion. The surgical strategy must ensure that the iliac vessels are spared. If circulatory assistance is needed before or during transplantation and employs an iliac vessel, efforts must be made well in advance to preserve the contralateral side. Anesthetic and intensive care catheters must be placed in the jugular vein.
Our study has several limitations. The primary limitation lies in the non-identical characteristics of patients undergoing CKLTs and KALTs. Patients exhibit different etiologies of end-stage renal failure, varied indications for renal transplantation, and divergent points in their medical histories. This dissimilarity precludes direct comparison between the 2 surgical management modalities. As a result, these findings are purely exploratory and do not yield a definitive answer regarding the optimal strategy. To provide a conclusive answer, it would be necessary to randomize patients between the 2 procedures, while stratifying based on their characteristics and medical history. Furthermore, despite being a substantial single-center cohort, the sample size was insufficient, preventing the attainment of certain conclusions.
Conclusions
This is the first single-center study to present a relatively large cohort of CKLT and KALT transplant recipients. We report on patients’ survival, renal and lung graft function, and postoperative morbidity. KALT seems a reasonable option, with postoperative morbidity and renal graft function identical to those of KT in non-lung-transplanted patients. CKLT remains an attractive option for patients with respiratory failure associated with ESRD, but the high risk of fatal outcome (related to the procedure of LT) in lung recipient needs to be factored in. We believe that criteria for CKLT could integrate more subtle parameters than renal function at the time of LT.
Figures
 Figure 1. Flowchart of lung transplants between November 1, 1988 and July 1, 2023 (Microsoft® Word, Version 16.83, Microsoft).
Figure 1. Flowchart of lung transplants between November 1, 1988 and July 1, 2023 (Microsoft® Word, Version 16.83, Microsoft).  Figure 2. (A) Kidney function following Combined kidney–lung transplantation and Kidney after lung transplantation. (B) Chronic lung allograft dysfunction in recipient from Combined kidney–lung transplantation (Prism 10, Version 10.2.2, GraphPad Software).
Figure 2. (A) Kidney function following Combined kidney–lung transplantation and Kidney after lung transplantation. (B) Chronic lung allograft dysfunction in recipient from Combined kidney–lung transplantation (Prism 10, Version 10.2.2, GraphPad Software).  Figure 3. Recipient survival according to Kaplan-Meier analysis. Mean±standard error of the mean (Prism 10, Version 10.2.2, GraphPad Software).
Figure 3. Recipient survival according to Kaplan-Meier analysis. Mean±standard error of the mean (Prism 10, Version 10.2.2, GraphPad Software). References
1. Ojo AO, Held PJ, Port FK, Chronic renal failure after transplantation of a nonrenal organ: N Engl J Med, 2003; 349(10); 931-40
2. Chandrakantan A, de Mattos AM, Naftel D, Increasing referral for renal transplant evaluation in recipients of nonrenal solid-organ transplants: A single-center experience: Clin J Am Soc Nephrol, 2006; 1(4); 832-36
3. de Perrot M, Licker M, Robert J, Successful combined lung and kidney transplantation for pulmonary lymphangioleiomyomatosis and renal angiolipomas: Eur Respir J, 1998; 12(6); 1479-81
4. Erdman J, Wolfram J, Nimke D, Lung transplant outcomes in adults in the United States: Retrospective cohort study using real-world evidence from the SRTR: Transplantation, 2022; 106(6); 1233-42
5. Bennett WM, DeMattos A, Meyer MM, Chronic cyclosporine nephropathy: the Achilles’ heel of immunosuppressive therapy: Kidney Int, 1996; 50(4); 1089-100
6. Ivulich S, Dooley M, Kirkpatrick C, Snell G, Clinical challenges of tacrolimus for maintenance immunosuppression post-lung transplantation: Transplant Proc, 2017; 49(9); 2153-60
7. Scaravilli V, Merrino A, Bichi F, Longitudinal assessment of renal function after lung transplantation for cystic fibrosis: Transition from post-operative acute kidney injury to acute kidney disease and chronic kidney failure: J Nephrol, 2022; 35(7); 1885-93
8. El-Husseini A, Aghil A, Ramirez J, Outcome of kidney transplant in primary, repeat, and kidney-after-nonrenal solid-organ transplantation: 15-year analysis of recent UNOS database: Clin Transplant, 2017; 31(11); 13108
9. Leard LE, Holm AM, Valapour M, Consensus document for the selection of lung transplant candidates: An update from the International Society for Heart and Lung Transplantation: J Heart Lung Transplant, 2021; 40(11); 1349-79
10. Woll F, Mohanka M, Bollineni S, Characteristics and outcomes of lung transplant candidates with preexisting renal dysfunction: Transplant Proc, 2020; 52(1); 302-8
11. Osho AA, Castleberry AW, Snyder LD, Assessment of different threshold preoperative glomerular filtration rates as markers of outcomes in lung transplantation: Ann Thorac Surg, 2014; 98(1); 283-90
12. Osho AA, Hirji SA, Castleberry AW, Long-term survival following kidney transplantation in previous lung transplant recipients-An analysis of the UNOS registry: Clin Transplant, 2017; 31(5); 12953
13. Cassuto JR, Reese PP, Sonnad S, Wait list death and survival benefit of kidney transplantation among nonrenal transplant recipients: Am J Transplant, 2010; 10(11); 2502-11
14. Gregor A, Kolansky J, Wirshup K, Benefit of kidney transplantation for post lung transplantation renal failure: J Surg Res, 2023; 284; 303-11
15. Ruderman I, Sevastos J, Anthony C, Outcomes of simultaneous heart-kidney and lung-kidney transplantations: the Australian and New Zealand experience: Intern Med J, 2015; 45(12); 1236-41
16. Chen Q, Malas J, Roach A, Simultaneous lung-kidney transplantation in the United States: Ann Thorac Surg, 2023; 116(5); 1063-70
17. von Elm E, Altman DG, Egger M, The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies: J Clin Epidemiol, 2008; 61(4); 344-49
18. Holm AM, Fedson S, Courtwright A, International society for heart and lung transplantation statement on transplant ethics: J Heart Lung Transplant, 2022; 41(10); 1307-8
19. Clavien PA, Barkun J, de Oliveira ML, The Clavien-Dindo classification of surgical complications: five-year experience: Ann Surg, 2009; 250(2); 187-96
20. Mesnard B, Leroy M, Hunter J, Kidney transplantation from expanded criteria donors: An increased risk of urinary complications – the UriNary Complications of Renal Transplant (UNyCORT) study: BJU Int, 2022; 129(2); 225-33
21. Fessler J, Glorion M, Finet M, Perioperative outcomes during double-lung transplantation and retransplantation in cystic fibrosis patients: A monocentric cohort study: J Cardiothorac Vasc Anesth, 2023; 37(6); 964-71
22. Halloran K, Aversa M, Tinckam K, Comprehensive outcomes after lung retransplantation: A single-center review: Clin Transplant, 2018; 32(6); e13281
23. Organ Procurement & Transplantation network: Establish Eligibility Criteria and Safety Net for Heart-Kidney and Lung-Kidney Allocation https://optn.transplant.hrsa.gov/media/npslvryi/establish-eligibility-criteria-and-safety-net-for-heart-kidney-and-lung-kidney-allocation_winter-2022-pc.pdf
24. Osho AA, Castleberry AW, Snyder LD, Determining eligibility for lung transplantation: A nationwide assessment of the cutoff glomerular filtration rate: J Heart Lung Transplant, 2015; 34(4); 571-79
25. Lentine KL, Smith JM, Hart A, OPTN/SRTR 2020 Annual Data Report: Kidney: Am J Transplant, 2022; 22(Suppl 2); 21-136
Figures
Figure 1. Flowchart of lung transplants between November 1, 1988 and July 1, 2023 (Microsoft® Word, Version 16.83, Microsoft).Figure 2. (A) Kidney function following Combined kidney–lung transplantation and Kidney after lung transplantation. (B) Chronic lung allograft dysfunction in recipient from Combined kidney–lung transplantation (Prism 10, Version 10.2.2, GraphPad Software).Figure 3. Recipient survival according to Kaplan-Meier analysis. Mean±standard error of the mean (Prism 10, Version 10.2.2, GraphPad Software). Tables
 Table 1. Recipient characteristics.
Table 1. Recipient characteristics.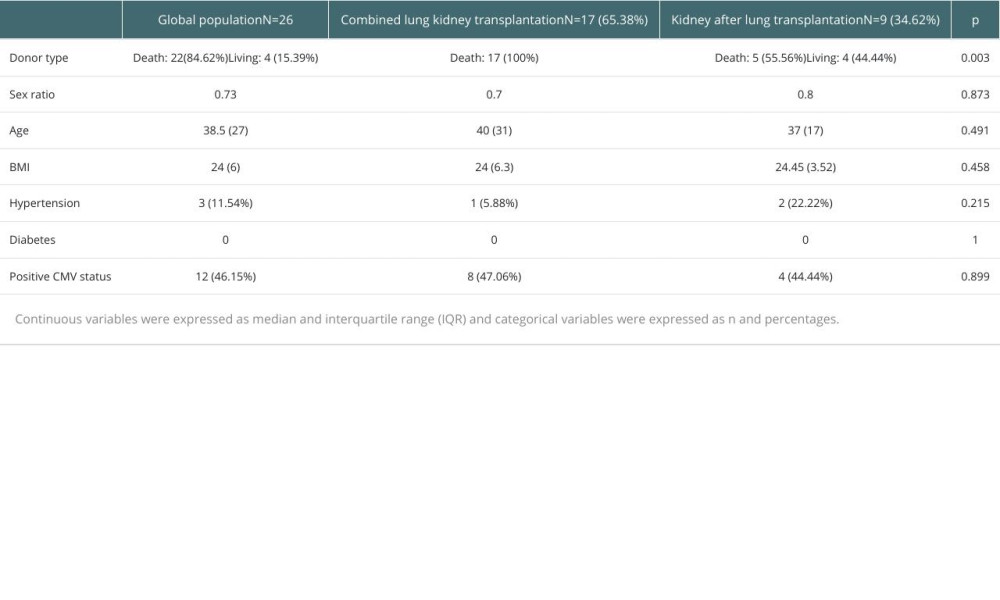 Table 2. Donor characteristics.
Table 2. Donor characteristics.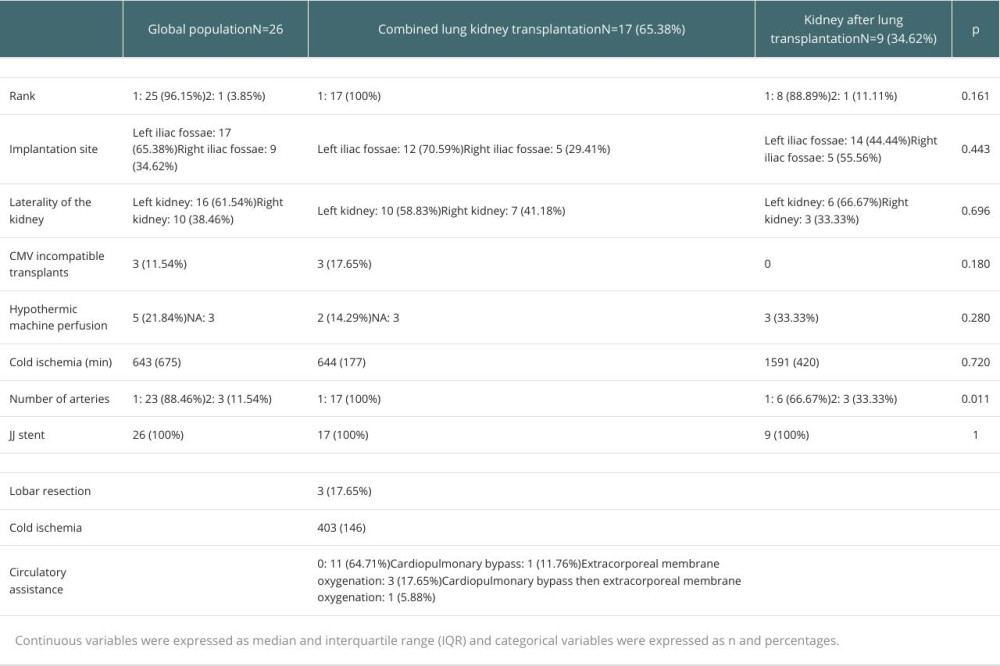 Table 3. Intraoperative data of combined kidney–lung transplantation and kidney after lung transplantation.
Table 3. Intraoperative data of combined kidney–lung transplantation and kidney after lung transplantation. Table 4. Postoperative care and early postoperative outcomes.
Table 4. Postoperative care and early postoperative outcomes.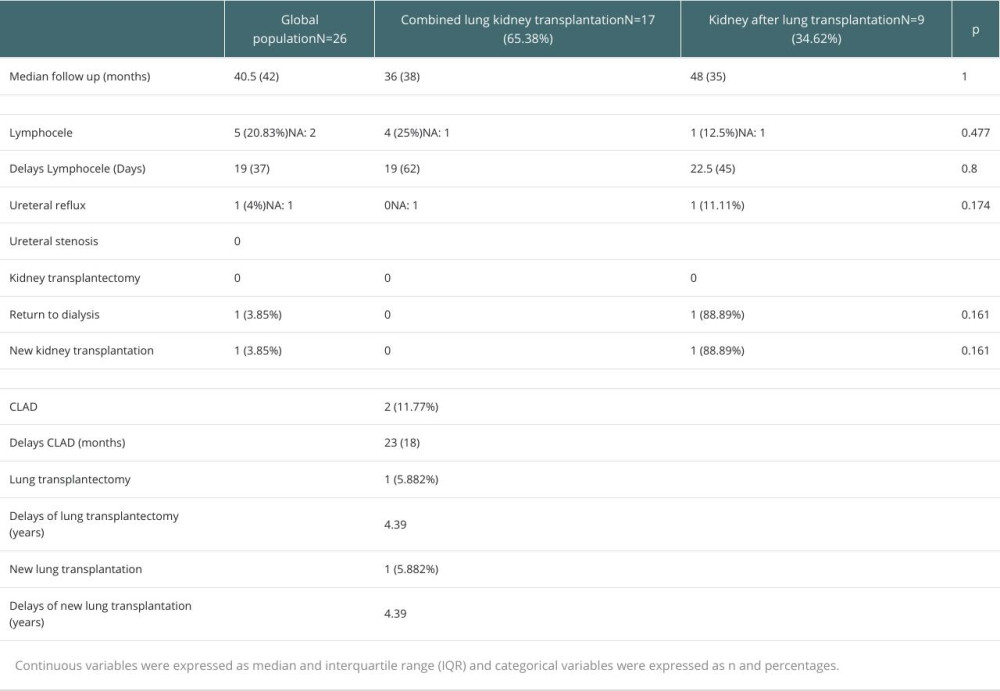 Table 5. Lung and kidney graft outcomes.Table 1. Recipient characteristics.Table 2. Donor characteristics.Table 3. Intraoperative data of combined kidney–lung transplantation and kidney after lung transplantation.Table 4. Postoperative care and early postoperative outcomes.Table 5. Lung and kidney graft outcomes.
Table 5. Lung and kidney graft outcomes.Table 1. Recipient characteristics.Table 2. Donor characteristics.Table 3. Intraoperative data of combined kidney–lung transplantation and kidney after lung transplantation.Table 4. Postoperative care and early postoperative outcomes.Table 5. Lung and kidney graft outcomes. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988