03 June 2025: Original Paper
Effects of Donor-Recipient Race Matching on Kidney Transplant Survival
Marie Chisholm-Burns DOI: 10.12659/AOT.947720
Ann Transplant 2025; 30:e947720






Abstract
BACKGROUND: Given the scarcity of donor organs in the United States, the ability to prolong kidney transplant graft survival is a significant public health concern. Although it has been suggested that donor-recipient race-matching could improve kidney transplant outcomes, findings of previous studies are inconsistent. Therefore, the objective of this study was to conduct a systematic review examining the relationship between Black and White donor-recipient race-matching and graft and patient survival in adult primary kidney transplant recipients.
MATERIAL AND METHODS: Ovid Medline and Embase literature searches were conducted from earliest index date through October 2024. The following data were extracted and summarized: study characteristics, patient population characteristics, and findings associated with graft and patient survival. Quality assessment and magnitude of effects were evaluated, and Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to determine evidence certainty.
RESULTS: Of 4676 citations, 7 studies met inclusion criteria. Two studies reported Black-Black donor-recipient pairings, 2 studies reported Black-White donor-recipient pairings, and 3 studies reported White-Black donor-recipient pairings were at significantly higher risk for graft failure than the reference group; however, effect magnitude was small. Studies found the relationship between race-matching and patient survival was not statistically significant. Per GRADE, evidence concerning graft and patient survival is of low certainty or quality.
CONCLUSIONS: Studies generally found no differences in patient survival, and although Black-Black, Black-White, and White-Black donor-recipient pairings were associated with decreased graft survival in some studies, effects were small and likely clinically irrelevant. Further investigation of modifiable factors influencing graft survival is needed.
Keywords: Graft Survival, Kidney Transplantation, Mortality, Race Factors, transplant recipients, Humans, Black or African American, Donor Selection, Tissue Donors, white
Introduction
Given the scarcity of donor organs in the United States, the ability to prolong kidney transplant graft survival is a significant public health concern, particularly among Black transplant recipients whose survival rates continue to lag behind those of White recipients [1]. Investigators have suggested race-matching could be predictive of solid-organ transplant outcomes because donors “of similar ethnographic origin could provide greater physiologic and genetic similarities between the organ donor and recipient” [2,3]. However, findings of prior studies of race-matching in kidney transplant populations are not consistent.
More specifically, some prior studies found positive associations between race-matching and kidney transplant outcomes, while other studies did not [2–10]. For example, Locke et al [4] found that race-matched adult Black kidney transplant recipients experienced greater graft and patient survival than did Black recipients who received White donor kidneys. In contrast, LeClaire et al [2] found that compared with race-mismatched recipients, race-matched adult Black kidney transplant recipients had worse graft survival but no significant differences in patient survival [2]. Callender et al [6,7] found that race-matched and mismatched Black kidney transplant recipients and race-mismatched White recipients had worse graft survival than did race-matched White recipients. Patient survival outcomes were mixed, with White recipients who received Black donor kidneys at increased risk of mortality and Black recipients who received White donor kidneys at decreased risk of mortality than race-matched White recipients, while there was no significant difference versus race-matched Black recipients [7]. Yet another study found no significant differences in 1-year graft survival in race-matched Black kidney transplant recipients, compared with Black recipients who received White donor kidneys [5].
Due to conflicting evidence and to better understand the effects of race-matching on kidney transplant outcomes, a systematic review that evaluates and synthesizes the existing evidence would be valuable; however, such a synthesis has not yet been published, representing a gap in the literature. Thus, the objective of this study was to address this gap and conduct a systematic review examining the relationship between Black and White donor-recipient race-matching (compared with mismatching, defined as donor and recipient being of different races) and the outcomes of graft and patient survival in adult primary kidney transplant recipients. We hypothesized that the preponderance of evidence would support race-matching is not significantly associated with graft or patient survival among adult kidney transplant recipients. If the hypothesis is substantiated, this would lend further support to the 2024 decision to remove the Black race coefficient from the Kidney Donor Profile Index (KDPI), an algorithm intended to predict quality of a donor organ and assist in determining suitability of an organ match [11,12].
Material and Methods
STUDY SELECTION:
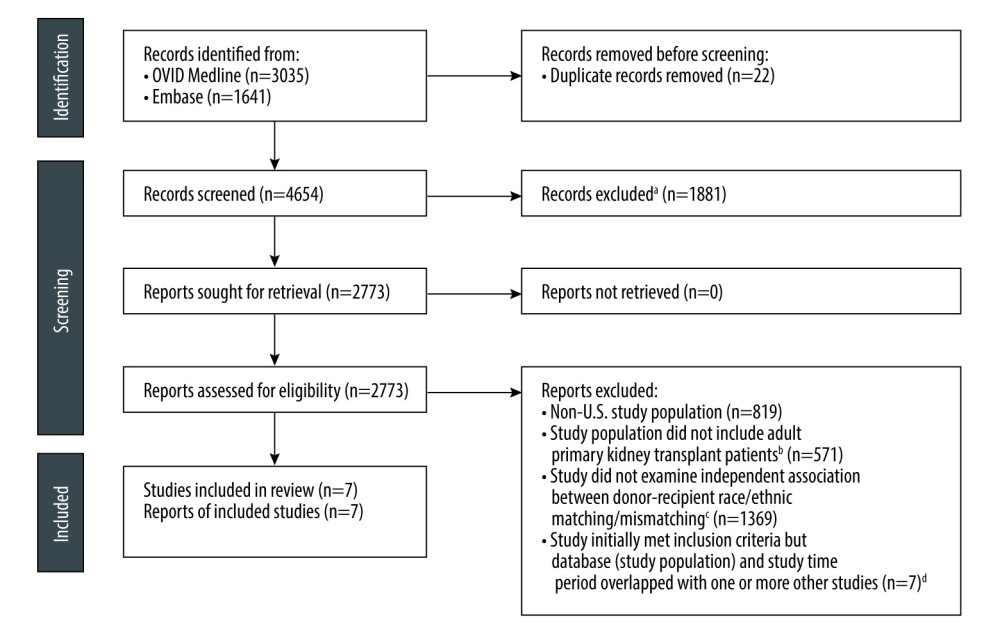
One reviewer (CS) conducted an initial screening of literature search results to exclude non-quantitative studies, such as qualitative studies, commentaries, and editorials (Figure 1). Two reviewers (MCB and CS) then independently conducted the study inclusion process, described in Figure 1. Peer-reviewed studies were included if they met all of the following criteria: (1) U.S. study (patient) population; (2) study population composed of adults (18 years or older) who had undergone primary kidney transplant; (3) quantitative in nature with statistical significance testing; (4) study included at least one Black and/or White race-matched donor-recipient pairing; and (5) analyzed the independent relationship between donor-recipient race-matching and mismatching and outcomes of interest (graft survival/failure and/or patient survival/mortality). In the assessment of eligibility, studies were excluded if they included a non-U.S. patient population, did not focus on adult primary kidney transplant patients, and did not assess the independent relationship between Black and/or White donor-recipient race-matching and graft and/or patient survival. Additionally, and as described in Figure 1, to eliminate redundant populations, studies that otherwise met inclusion criteria were excluded due to overlapping study databases (populations) and/or time periods. Inclusion among studies using the same database was based on not having overlapping populations and time periods, and a combination of considerations, including having a longer study time period, larger study population, and/or examining both outcomes of interest (graft and patient survival). There was no disagreement on included studies between the 2 reviewers.
DATA EXTRACTION:
Two reviewers (MCB and CS) independently used a standardized data extraction tool. Data were collected concerning study characteristics (eg, study design, sample size), patient population characteristics (eg, age, sex, race/ethnicity, donor-recipient pairings, donor type), type of analysis (bivariate, multivariate), and study findings. We primarily focused on Black and White donor-recipient race-matched pairings (eg, Black-Black, White-White) and race-mismatched pairings (eg, Black-White, White-Black), as they represent the largest adult kidney transplant populations (approximately 80% of adult kidney transplant recipients in the U.S. are Black or White) [17]. Other racial and ethnic populations were not consistently represented in studies. When necessary to resolve disagreement, as occurred with 3 studies, reviewers met and reconciled extracted data [14]. A cross-check of extracted data was performed on all included studies as a quality control measure.
When extracting data concerning study findings, the following transplant outcomes in association with donor-recipient race-matching/mismatching were recorded: graft survival (or graft failure/loss) and patient survival (or patient mortality). Additionally, data were collected concerning length of the follow-up period, reference or comparator group (eg, White-White donor-recipient pairing was commonly used as the reference group across studies), and statistical significance of the association between transplant outcome and donor-recipient race-matching. For statistically significant associations between donor-recipient race-matching and transplant outcomes (ie, graft survival/failure, patient survival/mortality), effect measures (eg, hazard, odds, risk ratios) and direction of the association were described (for example, graft or patient survival was better or worse among race-matched vs mismatched recipients). Study data are available upon request to the corresponding author.
QUALITY APPRAISAL:
Two reviewers (MCB and CS) independently conducted a quality assessment of included studies using the Quality Assessment of Observational Cohort and Cross-Sectional Studies tool published by the National Institutes of Health [18]. The tool includes a series of questions concerning whether a given study was designed to address risks of bias and internal validity threats. A study was rated as “good quality” if it addressed at least 70% of risks, “fair quality” if it addressed at least 50% of risks, and “poor quality” if it addressed less than 50% of risks [19,20]. To resolve disagreements, as occurred with 5 studies, reviewers met and reconciled the quality assessment [14].
CERTAINTY OF EVIDENCE ASSESSMENT:
Certainty of evidence for each outcome of interest (graft survival/loss and patient survival/mortality) was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) guideline [21]. According to Guyatt et al, “quality of evidence” for systematic reviews “reflects the extent of confidence that an estimate of effect is correct” [21]. Per GRADE, there are 4 levels of certainty evidence (high, moderate, low, very low), with starting values based on study design. Specifically, randomized trials begin as high-certainty (high-quality) evidence, while observational studies begin as low-certainty (low-quality) evidence [21]. There are 5 factors that can decrease certainty of evidence: study limitations, inconsistency of results, indirectness of evidence, imprecision, and publication bias [21]. Likewise, there are 3 factors that can increase certainty of evidence: large magnitude of effect, plausible confounding, and dose-response gradient [21]. Each included study was assessed by 2 reviewers (MCB and CS) using GRADE by first determining study design and then considering the factors that can decrease or increase certainty of evidence.
DATA SYNTHESIS:
Data were synthesized using Microsoft Excel (Microsoft Corporation, Redmond, WA). Study characteristics and outcomes were summarized using frequency counts. Of note, multiple studies examined the association between donor-recipient race-matching and outcomes of interest at different time points after transplantation. Frequency counts summarized results of multivariate analysis (or bivariate analysis, when multivariate was not conducted) and overall finding (if available, rather than multiple time periods in the same study). Interpretation of magnitude of effects, which were primarily hazard ratios or risk ratios, was based on Lu et al [22] and Chen et al [23]. For example, Lu et al [22] suggested hazard ratios of 1.16–1.68 indicate small effects, and Chen et al [23] suggested odds ratios of 1.46–1.68 indicate small effects.
Results
Of 4676 citations identified in the literature search, 7 studies were included in the systematic review (Figure 1). The design of all 7 studies was classified as observational or case-control, with 4 using large registry or database data (Table 1). No randomized controlled trials met inclusion criteria. All 7 studies reported graft survival or loss outcomes. Three studies reported patient survival or mortality outcomes. In the quality assessment (Table 2), all 7 studies were rated as good or fair.
Included study sample sizes ranged from 510 to 265 177, with 5 studies having samples greater than 5000 (Table 1). Three of 7 studies provided data on patient sex. Three studies included only deceased donor transplants, and the remaining 4 included deceased and living donor transplants. Among donor-recipient racial pairings, Black-Black pairings were included in 6 of 7 studies, White-White pairings in all 7 studies, Black-White pairings in 5 studies, and White-Black pairings in 5 studies. Mismatched-White and mismatched-Black donor-recipient pairings were included in 2 studies.
Table 1 summarizes the outcomes of each of the 7 included studies [2,5,24–28]. Five of 7 studies reported statistically significant associations between race-matching or mismatching and the graft survival/failure outcome (Tables 1, 3). Two studies conducted multivariate analysis to control for confounding variables, with small magnitude of effects (hazard/risk ratios of 1.118 and 1.26). GRADE indicates the evidence is low-certainty (low-quality), as the studies are observational. Two of 6 studies reported Black-Black donor-recipient pairings were at significantly higher risk for graft failure, or decreased graft survival, compared with the reference group (White-White or race-mismatched pairing). Three of 5 studies reported White-Black donor-recipient pairings were at significantly higher risk for graft failure versus White-White pairing, while 1 study did not find a statistically significant relationship versus Black-Black pairing. Two of 5 studies reported Black-White donor-recipient pairings were at significantly higher risk for graft failure, or decreased graft survival, compared with the White-White reference group. Two of 3 studies found the relationship between race-matching and patient survival was not significant, while the third found patient survival was independent of recipient race, with White donor organs associated with increased patient survival, compared with Black donor organs, regardless of recipient race (Tables 1, 4).
Discussion
With nearly 90 000 patients on the U.S. kidney transplant waitlist and an ongoing shortage of donor organs, efforts to use donor organs more effectively and prolong graft survival remain a focal point of care [17,29]. To that end, the present systematic review examined the association between donor-recipient race-matching and graft and patient survival among Black and White kidney transplant recipients. We hypothesized the findings of this systematic review would demonstrate race-matching is not significantly associated with graft or patient survival. Consistent with our hypothesis, the studies in our systematic review generally indicated no significant differences in patient survival based on race-matching or mismatching, supporting that race-matching, on its face, has limited utility in patient survival.
Inconsistent with our hypothesis, the preponderance of studies (5 of 7) indicated that Black-Black, Black-White, and/or White-Black donor-recipient pairings were at greater risk for decreased graft survival. However, the findings are likely clinically insignificant, as GRADE suggests low-certainty evidence. This assessment was based on study design, with all 7 included studies being observational or case-control, as well as having a lack of factors that would increase certainty, such as large magnitude of effects. Observational studies are considered low-certainty evidence, due to increased risk of bias (eg, confounding) and inability to make causal inferences. Indeed, only 2 studies controlled for confounding factors, and closer examination of these 2 studies reveals their findings, although statistically significant, are of small magnitude. For example, LeClaire et al [2] found race-matched Black kidney transplant recipients experienced statistically significantly worse graft survival (ranging from 0.8% to 4%, depending on time period), compared with mismatched Black recipients, but concluded race-matching did “not influence patient outcomes enough to factor into organ allocation offers.”
The lack of large effects, low certainty of evidence, and insubstantial value in clinical practice noted in our systematic review supports the recent decision to remove the Black race coefficient from the KDPI [11,12]. The use of race as a coefficient in the KDPI scores a kidney from a Black donor as lower quality than from a non-Black donor [30,31]. Iltis [32] argued that this downgrading of Black donor kidneys contributed to increased non-use and potential waste of donor organs. Based on our findings, and to increase transplant access, we concur the quality of the current evidence does not justify utilization of a Black race coefficient to reduce the score of donor kidneys. Race is a social construct, rather than a biological one, and could be a likely proxy of genetic risk factors such as APOL1 gene variants and other factors (eg, the social determinants of health [SDOH) contributing to individual health [32–34]. As such, there is a strong argument for carefully considering how race is used in medical decision-making.
Additionally, strategies to improve organ allocation and transplant outcomes should focus on the SDOH, which are more salient factors underlying associations between race and health outcomes [34]. The SDOH are “conditions in the environment where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks” [35]. We posit kidney transplant access and outcomes may be bolstered through increased understanding of and intervening to address SDOH that negatively impact the health and well-being of some potential kidney transplant recipients and society as a whole (ie, the pool of potential kidney transplant donors). SDOH include the domains of healthcare access and quality, education access and quality, neighborhood and built environment, social and community context, and economic stability [35]. Donors can be affected by SDOH such as health insurance, food and housing insecurity, social support, employment, income, and health literacy in a number of ways that contribute to healthcare access, overall health and well-being, and ultimately, the viability of donor organs. These same SDOH can likewise affect the health and well-being of kidney transplant recipients, both before and after transplant, influencing the prevalence of chronic kidney disease and end-stage renal disease, access to pre- and post-transplant care (including immunosuppressant medications), and graft and patient survival outcomes.
Numerous approaches can be used to mitigate SDOH in kidney transplant care. One such approach starts with screening and monitoring SDOH, as identification of SDOH uniquely affecting individual patients will allow providers to recommend and coordinate with appropriate support services [36]. For example, kidney transplant recipients with limited income as a barrier to obtaining prescription medication can be referred to programs that specialize in supporting medication accessibility. Increasing access can, in turn, increase medication adherence, which is critical to graft survival. As another example, at the community level, Callendar et al [6] recommend health education campaigns raising awareness about the importance of organ health, which could serve 2 functions: encourage prevention of kidney disease and increase interest in and ability to serve as an organ donor. Future studies should evaluate the effects of SDOH-targeted interventions in improving kidney transplant care access and outcomes.
This systematic review has strengths and limitations. Among its strengths, the study used an expansive literature search strategy to capture studies that may otherwise have not been included in a more narrow strategy. Additionally, although studies with pediatric patients were excluded to eliminate this confounding factor, some studies were not explicit on this characteristic when describing their population; given this uncertainty and to optimize study inclusion yield, we elected to retain these studies in our synthesis. As the included studies were observational and retrospective in nature, causality of the relationship between race-matching and graft and patient survival outcomes cannot be determined. Although not a limitation, a meta-analysis was not conducted due to heterogeneity of the included studies.
Conclusions
This systematic review is the first of its kind to summarize evidence concerning the effects of donor-recipient race-matching on kidney transplant outcomes among Black and White recipients. Regarding patient survival, studies examining this outcome generally did not find significant differences based on race-matching. Although Black-Black, Black-White, and White-Black donor-recipient pairings were associated with decreased graft survival across some studies, because of their small magnitude, these effects are likely clinically irrelevant. As such, race-matching or mismatching between donor and recipient should not influence decision-making regarding organ allocation. Further investigation of donor and recipient factors affecting graft and patient survival, particularly genetic and structural factors influencing health, is warranted to improve utilization of donor kidneys, access to kidney transplantation, and outcomes of kidney transplant recipients.
Tables
Table 1. Description of graft and patient survival outcomes of included studies (n=7) [2,5,24–28].![Description of graft and patient survival outcomes of included studies (n=7) [2,5,24–28].](https://jours.isi-science.com/imageXml.php?i=t1-anntransplant-30-e947720.jpg&idArt=947720&w=1000) Table 2. Quality assessment of included observational and case-control studies (n=7) [2,5,24–28a b].
Table 2. Quality assessment of included observational and case-control studies (n=7) [2,5,24–28a b].![Quality assessment of included observational and case-control studies (n=7) [2,5,24–28a b].](https://jours.isi-science.com/imageXml.php?i=t2-anntransplant-30-e947720.jpg&idArt=947720&w=1000) Table 3. Graft survival outcomes (n=7) [2,5,24–28].
Table 3. Graft survival outcomes (n=7) [2,5,24–28].![Graft survival outcomes (n=7) [2,5,24–28].](https://jours.isi-science.com/imageXml.php?i=t3-anntransplant-30-e947720.jpg&idArt=947720&w=1000) Table 4. Patient survival outcomes (n=3) [2,25,26].
Table 4. Patient survival outcomes (n=3) [2,25,26].![Patient survival outcomes (n=3) [2,25,26].](https://jours.isi-science.com/imageXml.php?i=t4-anntransplant-30-e947720.jpg&idArt=947720&w=1000)
References
1. Lentine K, Smith JM, Lyden GR, OPTN/SRTR 2022 annual data report: Kidney: Am J Transplant, 2024; 24(2 Suppl 1); S19-S118
2. LeClaire JM, Smith NJ, Chandratre S, Solid organ donor-recipient race-matching: Analysis of the United Network for Organ Sharing database: Transplant Int, 2021; 34; 640-47
3. Lv K, Wu Y, Lai W, Simpson’s paradox and the impact of donor-recipient race-matching on outcomes post living or deceased donor kidney transplantation in the United States: Front Surg, 2022; 9; 1050416
4. Locke JE, Warren DS, Dominici F, Donor ethnicity influences outcomes following deceased-donor kidney transplantation in Black recipients: J Am Soc Nephrol, 2008; 19; 2011-19
5. Gaston RS, Hudson SL, Deierhoi MH, Improved survival of primary cadaveric renal allografts in Blacks with quadruple immunosuppression: Transplantation, 1992; 53(1); 103-9
6. Callendar CO, Cherikh WS, Miles PV, Blacks as donors for transplantation: Suboptimal outcomes overcome by transplantation into other minorities: Transplant Proc, 2008; 40; 995-1000
7. Callendar CO, Cherikh WS, Traverso P, Effect of donor ethnicity on kidney survival in different recipient pairs: An analysis of the OPTN/UNOS database: Transplant Proc, 2009; 41; 4125-30
8. Kwan JM, Hajjiri Z, Chen YF, Donor and recipient ethnicity impacts renal graft adverse outcomes: J Racial Ethn Health Disparities, 2018; 5; 1003-13
9. Molnar MZ, Kovesdy CP, Bunnapradist S, Donor race and outcomes in kidney transplant recipients: Clin Transplant, 2013; 27; 37-51
10. Schold JD, Kaplan B, Chumbler NR, Access to quality: evaluation of the allocation of deceased donor kidneys for transplantation: J Am Soc Nephrol, 2005; 16; 3121-27
11. Organ Procurement & Transplantation Network: OPTN board approves exclusion of race, heptatis c status from estimate of deceased donor function June 28, 2024 Available from: https://optn.transplant.hrsa.gov/news/optn-board-approves-exclusion-of-race-hepatitis-c-status-from-estimate-of-deceased-donor-kidney-function/
12. Organ Procurement & Transplantation Network: A guide to calculating and interpreting the Kidney Donor Profile Index (KDPI) Update: March 23, 2020
13. Page MJ, Moher D, Bossuyt PM, PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews: BMJ, 2021; 372; n160
14. Higgins J, Thomas J: Cochrane handbook for systematic reviews of interventions Available from:https://training.cochrane.org/handbook/current
15. : Medline® 2025 Database Guide Available from: https://ospguides.ovid.com/OSPguides/medline.htm
16. Embase: Embase content is updated daily and expanding globally Available from:https://ospguides.ovid.com/OSPguides/medline.htm
17. Organ Procurement & Transplantation Network: National data Available from:https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/
18. National Heart, Lung, and Blood Institute: Study quality assessment tools Available from:https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tool
19. Uloko AE, Musa BM, Ramalan MA, Prevalence and risk factors for diabetes mellitus in Nigeria: A systematic review and meta-analysis: Diabetes Ther, 2018; 9; 1307-16
20. Li Z-H, Hasson F, Resilience, stress, and psychological well-being in nursing students: A systematic review: Nurse Education Today, 2020; 90; 104440
21. Guyatt GH, Oxman AD, Vist GE, GRADE: What is “quality of evidence” and why is it important to clinicians?: Br Med J, 2008; 336; 995-98
22. Lu Y, Cen W, Wang W, How big is a big hazard ratio in clinical trials?: Int J Clin Trials, 2023; 10(3); 195-200
23. Chen H, Cohen P, Chen S, How big is a big odds ratio? Interpreting the magnitudes of odds ratios in epidemiological studies: Communications in Statistics – Simulation and Computation, 2010; 38; 860-64
24. Meier-Kriesche H-U, Ojo AO, Cibrik DM, Relationship of recipient age and development of chronic allograft failure: Transplantation, 2000; 70(2); 306-10
25. Opelz G, Mickey MR, Terasaki PI, Influence of race on kidney transplant survival: Transplant Proc, 1977; 9(1); 137-42
26. Perdue ST, Terasaki PI, Analysis of interracial variation in kidney transplant and patient survival: Transplantation, 1982; 34(2); 75-77
27. Tiwari J, Terasaki PI, Mickey MR, Factors influencing kidney graft survival in the cyclosporine era: A multivariate analysis: Transplant Proc, 1987; 19(1 pt 3); 1839-41
28. Vincenti F, Duca RM, Amend W, Immunologic factors determining survival of cadaver-kidney transplants. The effect of HLA serotyping, cytotoxic antibodies and blood transfusions on graft survival: N Eng J Med, 1978; 299(15); 793-98
29. Health Resources & Services Administration: Organ donation statistics Available from:https://www.organdonor.gov/learn/organ-donation-statistics
30. Miller J, Lyden GR, McKinney WT, Impacts of removing race from the calculation of the kidney donor profile index: Am J Transplant, 2023; 23; 636-41
31. Gumber RI, Doshi MD, Is it time to drop the use of race from kidney donor risk index calculator?: Transplantation, 2024; 108(8); 1643-46
32. Iltis AS, Despite high demand, kidneys donated by Black Americans are more likely to be thrown away: Here’s why June 26, 2024, CNN Available from: https://www.cnn.com/2024/06/26/health/black-kidney-donations-bioethics-reaj/index.html
33. APOLLO Transplantation Outcomes Consortium: Study description Available from: https://theapollonetwork.org/
34. Bundy JD, Mills KT, He H, Social determinants of health and premature death among adults in the USA from 1999 to 2018: A national cohort study: Lancet Public Health, 2023; 8(6); e422-e31
35. U.S. Department of Health and Human Services, Social determinants of health: Healthy People 2030 Available from:https://health.gov/healthypeople/priority-areas/social-determinants-health
36. Davidson KW, Kemper AR, Doubeni CA, Developing primary care-based recommendations for social determinants of health: methods of the U.S. Preventive Services Task Force: Ann Intern Med, 2020; 173; 461-67
Tables
Table 1. Description of graft and patient survival outcomes of included studies (n=7) [2,5,24–28].Table 2. Quality assessment of included observational and case-control studies (n=7) [2,5,24–28a b].Table 3. Graft survival outcomes (n=7) [2,5,24–28].Table 4. Patient survival outcomes (n=3) [2,25,26].Table 1. Description of graft and patient survival outcomes of included studies (n=7) [2,5,24–28].Table 2. Quality assessment of included observational and case-control studies (n=7) [2,5,24–28a b].Table 3. Graft survival outcomes (n=7) [2,5,24–28].Table 4. Patient survival outcomes (n=3) [2,25,26]. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988