27 May 2025: Original Paper
Impact of Preoperative Treatment on Donor Hepatic Steatosis in Living Donor Liver Transplantation
Ahmet Atasever DOI: 10.12659/AOT.947772
Ann Transplant 2025; 30:e947772






Abstract
BACKGROUND: Living donor liver transplantation (LDLT) faces increasing challenges due to the rising prevalence of hepatic steatosis among potential donors. Moderate steatosis (30-60%) is particularly problematic, often leading to donor exclusion and reducing the available donor pool. Preoperative interventions aiming to reduce hepatic fat content have emerged as a potential strategy, but data regarding their safety and efficacy remain limited.
MATERIAL AND METHODS: This retrospective, single-center study evaluated 34 living liver donors between June 2023 and August 2024. Fourteen donors received preoperative treatment for moderate hepatic steatosis, while 20 donors with mild or no steatosis served as controls. Pre- and post-treatment assessments included body mass index (BMI), liver fat assessment via computed tomography (CT), liver function tests, and perioperative outcomes.
RESULTS: Preoperative treatment significantly reduced hepatic fat content, with all treated donors achieving steatosis levels below 30% (P<0.001). BMI and GGT levels also decreased significantly after treatment (P=0.01 and P=0.04, respectively). Postoperative liver function, intensive care unit stay, and hospital discharge times were comparable between the treated and control groups (P>0.05). No donor experienced serious complications during the early postoperative period or the first year of follow-up. All donors maintained satisfactory graft and remnant liver function, and no treatment-related adverse events were observed.
CONCLUSIONS: Preoperative management of moderate hepatic steatosis in living liver donors is effective in reducing liver fat to acceptable levels without compromising donor safety. This approach offers a promising strategy to expand the LDLT donor pool. Further large-scale, multicenter studies with extended follow-up are necessary to validate these findings.
Keywords: Donor Selection, Fatty Liver, Liver Transplantation, Humans, Living Donors, Male, Retrospective Studies, Female, adult, Middle Aged, Preoperative Care, Body Mass Index, Treatment Outcome
Introduction
Living donor liver transplantation (LDLT) has been shown to be reliable and has many advantages over deceased liver transplantation in the curative treatment of liver cirrhosis. However, there are many limiting factors in LDLT, such as the insufficient number of organ donors, insufficient donor liver volume, presence of vascular or biliary malformations in the donor liver, and advanced donor age [1].
Finding suitable donors for liver transplantation is a significant challenge due to the increasing number of patients requiring transplantation and the limited availability of donor organs [2]. Hepatic steatosis (HS) is one of the major factors limiting LDLT. It is usually associated with obesity, diabetes mellitus, alcohol use, and metabolic diseases [3]. Its association with obesity is well characterized in potential liver donors with body mass index (BMI) over 28 [4]. Globally rising obesity rates contribute significantly to the increased prevalence of hepatic steatosis [5]. In particular, the rising prevalence of obesity has led to an increased incidence of hepatic steatosis among potential donors, further complicating the process of identifying suitable liver donors.
The degree of HS is divided into 3 main groups according to the fat content in hepatocytes: mild (<30%), moderate (30–60%), and severe (>60%) [6]. Steatotic grafts are associated with impaired hepatocyte function and regeneration, as well as impaired cellular metabolism and microcirculatory disfunction. Additionally, HS is associated with an enhanced proinflammatory cytokine response that further worsens hepatocellular injury. Studies have shown that grafts with steatosis are more susceptible to endothelial damage and sinusoidal swelling during cold preservation. Mild (<30%) steatosis has not been associated with poor patient or graft survival, whereas severe (>60%) steatosis has been associated with poorer outcomes, including increased rates of graft dysfunction and early allotransplant dysfunction (EAD) and primary dysfunction (PNF), and prolonged hospital stay [7].
Currently, there is no established and accepted guideline worldwide regarding the use of fatty liver donors in liver transplantation [8–10]. The use of donors with fatty liver varies by country and transplant centers. Currently, grafts with <30% steatosis are considered usable by most centers, whereas donors with severe steatosis (>60%) are considered an absolute contraindication to use. There is insufficient information on LT outcomes of grafts with moderate (30–60%) steatosis, and there is ongoing debate about the use of these organs as grafts. HS exceeding 30% is recognized as an independent risk factor for graft loss [11]. Further studies are needed to better characterize the impact of moderate steatosis on recipient and graft outcomes [4,7].
Increasing obesity rates and inadequate organ donations significantly increase the rate of fatty liver donor candidates in LDLT. Therefore, especially in patients with few potential donors, reducing the fatty liver of donors to appropriate levels of steatosis in the preoperative period has become important for the success of the operation [12].
Treatment of potential donors with fatty liver is a multidisciplinary process and consists of several stages. Many medical professionals, such as transplant hepatologists, transplant nurses, dieticians, and transplant coordinators, are involved in this process. In the first stage, lifestyle changes, low-calorie diet, and resulting sufficient weight loss are targeted. Pharmacological treatment options constitute the second stage in reducing liver fat. Many drugs and drug combinations have been tried in patients, such as vitamin E, milk thistle, metformin, pioglitazone, SGLT-2 inhibitors, bile acids (ursodeoxycholic acid), obethycolic acid (OCA), LXL2 antibody (simtuzumab), pan-caspase inhibitors (emricasan), ASK-1 inhibitors (selonsertib), statins, and GLP-1 receptor agonists [13].
In the context of donor scarcity, this study attempted to expand the donor pool by treating and utilizing liver grafts with moderate steatosis (30–60%) in appropriately selected candidates. The impact of preoperative treatment on postoperative donor safety outcomes was also investigated.
Material and Methods
PREOPERATIVE DONOR EVALUATION FOR FATTY LIVER:
Computed tomography (CT) is routinely performed in the preoperative evaluation of donor candidates in our center. Liver biopsy is not routinely used to assess the level of donor liver steatosis. Donor candidates who do not have fatty liver or have less than 30% fatty liver can be living donor liver donors if other parameters are sufficient. Donor candidates with 30–60% fatty liver can be donors after they are treated and their liver fat ratio level drops below 30%. In our center, liver fat ratio control after treatment is also performed with CT. Considering the donor candidate’s compliance with treatment and the recipient’s clinical condition, no fixed protocol was applied regarding the duration of treatment and control time.
PARTICIPANTS:
The study included 37 living liver donor candidates who were studied at Demiroğlu Bilim University Florence Nightingale Hospital Liver Transplantation Center between June 2023 and August 2024 after informed consent was obtained. Seventeen donor candidates had received treatment for fatty liver. Twenty non-fatty donors were included in the study as a control group. Three patients could not become donors due to treatment incompatibility, as detailed in Figure 1. We compared the post-donor hepatectomy data of 14 patients who had received fatty liver treatment and 20 patients without fatty liver.
STUDY DESIGN AND SUBJECTS:
All demographic, clinical, radiological, and laboratory data were systematically entered into the transplant center’s electronic database by trained transplant coordinators and cross-checked for accuracy before analysis.
DEMOGRAPHIC AND CLINICAL DATA:
Donor candidates’ sex, age, status of receiving fat treatment, treatment duration, height, pre- and post-treatment body weight, and BMI data were recorded.
BIOCHEMICAL ASSESSMENT:
At the time of application, we assessed donor candidates for cholesterol (mg/dl, normal range <200), high-density lipoprotein cholesterol (HDL-s) (mg/dl, normal range >40), low-density lipoprotein cholesterol (LDL-c) (mg/dl, normal range <100), very low-density lipoprotein cholesterol (VLDL-c) (mg/dl, normal range <30), triglyceride (mg/dl, normal range <150), aspartate aminotransferase (AST) (U/L, normal range 11–34), alanine aminotransferase (ALT) (U/L, normal range <34), alkaline phosphatase (ALP) (U/L, normal range 46–122), gamma-glutamyl transferase (GGT, normal range 8–33), total bilirubin (mg/dl, normal range 0.31–1.20), direct bilirubin (mg/dl, normal range <0.5), international normalized ratio (INR, normal range 0.75–1.20), homeostatic model assessment - insulin resistance (HOMA-IR, normal range <2.5), hemoglobin A1C (HbA1C) (%, normal range 4–6), and fasting blood glucose (mg/dl, normal range 74–100). Post-treatment AST, ALT, ALP, GGT, total bilirubin, direct bilirubin, and INR values were recorded. The highest values of AST, ALT, ALP, GGT, total bilirubin, direct bilirubin, and INR were recorded after donor hepatectomy.
RADIOLOGICAL ASSESSMENT:
In the diagnosis of hepatosteatosis, the Hounsfield units (HU) ratio between the liver and spleen was examined on CT. Liver fat ratios were also recorded before and after treatment. The Myrian® 2.7.1 software program was used for liver volume assessments. Liver volumes were recorded before and after treatment.
HEPATOSTEATOSIS TREATMENT AND FOLLOW-UP:
Combined antioxidant medical treatment consisting of vitamin E, milk thistle, silibilin, and artichoke leaf extract was started for donor candidates with 30–60% fatty liver. Metformin 2×1000 mg treatment was also added to the treatment for donor candidates with a HOMA-IR ratio over 2.5. Donor candidates were called for weekly follow-ups, and weekly weight and BMI checks were performed. At 1–3 months after treatment, donor candidates who were able to lose at least 5 kg or more and whose liver transaminases returned to normal underwent second CT scans to check for fatty liver. Three patients were excluded from the study due to non-compliance with diet and medical treatment. All donors were systematically followed postoperatively with clinical and laboratory evaluations at 1 week, 1 month, 6 months, and 1 year after hospital discharge. All donors completed the scheduled postoperative follow-up evaluations, and no loss to follow-up occurred throughout the postoperative period.
STATISTICAL ANALYSES:
Descriptive statistics are presented as means and standard deviations for continuous variables and as numbers and percentages for categorical variables. Comparisons between groups (treated vs untreated donors) were performed using the Pearson chi-square test for categorical variables. Multivariate logistic regression analysis was used to identify independent factors associated with treatment outcomes, and odds ratios (ORs) with 95% confidence intervals (CIs) were reported.
No survival analysis, hazard ratio, or relative risk modeling was performed, as the study focused on perioperative donor outcomes rather than long-term survival. All statistical analyses were conducted using SPSS software version 22.0 (IBM Corp., Armonk, NY, USA). A two-tailed
Results
A total of 37 cases were included in the study. There were 17 donor candidates in the 30–60% hepatosteatosis group, while there were 20 donor candidates in the control group with less than 30% hepatosteatosis. Three patients in the treatment group were excluded from the study due to treatment incompatibility. Thus, a total of 34 cases were included in the study (Figure 1). Preoperative treatment resulted in a significant reduction in hepatic steatosis, with all treated donors achieving steatosis levels below 30% (
When the data obtained during the first application before treatment were evaluated, there was no significant difference between the groups in terms of age and sex (
When preoperative laboratory data were evaluated, pre-treatment fasting glucose, triglyceride, VLDL cholesterol and serum ALT levels were found to be significantly higher in the treated group compared to the untreated control group (
In the high hepatic steatosis group, a significant decrease in BMI levels was observed after treatment (
When the data obtained in the postoperative period were evaluated, it was observed that intensive care unit and hospital discharge times were similar in both liver donor groups. When the postoperative liver synthesis and excretion functions were evaluated, there was no statistically significant difference between the 2 groups, and the INR, AST, ALT, GGT, ALP, and bilirubin movements of the donors whose liver steatosis rate was reduced by treatment were similar to the control group that did not receive treatment (Table 4).
In the final stage, liver volumes of patients treated in the preoperative period were compared before and after treatment. In the donor group with 30–60% fatty liver, total liver volume and right and left lobe volumes were higher before treatment, as expected. In this group, total liver volume decreased by an average of 11% after treatment. While the right lobe volume decreased by an average of 12%, the left lobe volume decreased by an average of 8%. Remnant liver volume did not fall below 30% in any patient after treatment. In one of the patients who received treatment, a left lobe graft was transplanted to the recipient. In all other donors, a right lobe graft was used. The mean preoperative treatment period of the patients who were successfully treated and underwent donor hepatectomy was 40 days. Although the 3 patients who failed treatment were treated for an average of 90 days, the treatment was not successful due to treatment incompatibility. No significant difference was found between the 2 groups in terms of remnant volume/donor total body weight ratio and harvested graft weights. The ratio of intraoperatively removed/preoperatively calculated graft weights was very close to 1 and was similar between the 2 groups (Table 5).
Discussion
Detailed clinical and laboratory evaluations of potential donor candidates are mandatory to select a medically suitable donor. The rate of liver steatosis is a determining parameter that directly affects postoperative survival, recovery, and complication rates of healthy donor candidates. Therefore, liver steatosis is one of the main challenges that clinicians face before living donor liver transplantation [14,15]. Minimal hepatic steatosis is a common finding in living liver donor candidates and is generally considered reliable. Liver steatosis rates greater than 30% may have adverse effects on graft survival and have been shown to be associated with primary graft dysfunction and other posttransplant complications [16,17]. Many donor candidates cannot become donors due to high liver fat content and this situation significantly negatively affects the survival of many patients with advanced cirrhosis and hepatocellular carcinoma [18].
Rohan et al showed that liver steatosis of up to 20% is safe for living donor liver transplantation in their study of 325 donors. In their study, 325 donor candidates with 20% or less liver fat ratio were divided into 3 groups, and the postoperative prognosis of AST, ALT, bilirubin, and prothrombin time tests were followed in all 3 groups; similar to our study, no statistically significant difference was found between the peak and normalization times of the tests [19].
A global study examining the selection criteria and transplantation outcomes of suitable living liver donors at 24 centers performing more than 19 000 living donor liver transplants found that donors needed a median upper BMI limit of 33 to meet transplantation criteria [20]. In our study, the level of liver steatosis decreased to 30% and below in the control CT measurements of donors who lost weight and whose BMI decreased after treatment, and the postoperative recovery and AST, ALT, bilirubin, and prothrombin time test results in this donor group were almost the same as those of donors with normal weight and no steatosis.
Due to increasing obesity rates, difficulties in organ procurement, and the increased number of patients with liver cirrhosis requiring transplantation, the importance of using donor candidates with 20–30% liver fat ratio and a BMI over 30 as donors is steadily increasing [21]. The present study found that, in all donors with high liver steatosis and BMI, whose liver steatosis decreased to 30% or less after treatment, the post-transplantation enzyme, bilirubin, and INR peak and normalization process were similar to the group that did not receive treatment and did not have liver steatosis. The results of our study show that the safety margin of steatosis rate in living donor liver transplantation can be increased up to 30% and the upper limit of BMI can be increased up to 30–33.
In the measurements made after the treatment in donors with high liver steatosis, it was observed that the BMI and liver steatosis rate decreased, and there were decreases in total liver volume and right and left lobe volumes proportional to the weight loss. In addition, we found no significant change after the treatment applied in the 30% minimal remnant and GRWR >0.8 rates accepted all over the world in terms of donor safety [22]. This situation shows that there was no significant change in liver volume measurement findings that would prevent transplantation after the protocol applied in our center. Therefore, we believe that the difficulties in finding a suitable liver donor candidate in cirrhotic patients who do not require urgent transplantation can be significantly reduced with our treatment protocol.
In scientific publications, especially from Asia, when the only option for the recipient is a steatotic graft, transplant surgeons have suggested dual-graft transplantation, in which a fatty cadaveric graft containing 70–80% fat and a small non-steatotic graft are transplanted to the recipient at the same time. In the cadaveric graft, spontaneous fat dissolution has been observed within 2–4 weeks after surgery, by an unknown mechanism. The most widely accepted hypothesis regarding the spontaneous fat dissolution in the fatty cadaveric graft is that the body develops an intense and rapid mobilization of fat from the liver due to the excessive stress and hypermetabolic state that develops in response to major surgery [22]. Our study found that optimal liver steatosis and volume ratios can be achieved in an average of 6–8 weeks with an appropriate treatment combination in decompensated cirrhotic patients with fatty donor candidates. It was also shown that postoperative results of donors whose BMI and steatosis levels were reduced after a combination of diet and medical treatment were similar to donors with normal weight and no steatosis. Therefore, this treatment protocol applied in our center could be an alternative to dual-graft transplantation in recipients who do not require urgent liver transplantation.
Our study has some limitations. Firstly, the single-center, retrospective design and the small sample size restrict the generalizability of the results. The small sample size may also have limited the ability to detect statistically significant differences between groups. Donors were followed for only 1 year postoperatively, and long-term outcomes, such as potential metabolic changes in later years, were not assessed. Finally, the reasons for treatment non-compliance among excluded candidates were not thoroughly analyzed. Despite its disadvantages, we believe that our study can make important contributions to increasing the use of insufficient liver donor candidates through treatment.
Conclusions
Preoperative treatment in living liver donor candidates with moderate hepatic steatosis (30–60%) effectively reduced liver fat content, achieving levels below 30% in all treated donors. Donors who underwent treatment demonstrated similar liver function and recovery outcomes compared to the control group during the early postoperative period and within the first year. These findings suggest that preoperative treatment can safely expand the living donor pool. However, due to the small sample size, single-center design, and lack of long-term (>1 year) follow-up data, further multicenter studies with extended follow-up are needed to validate these results.
Figures
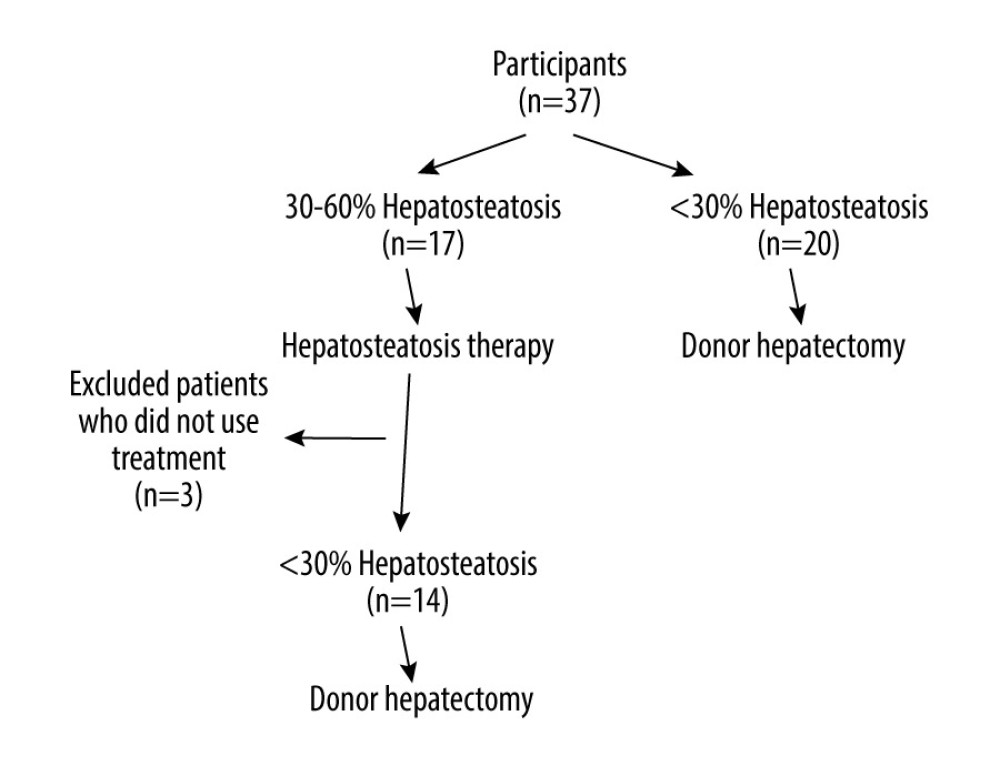 Figure 1. Patients and control group (Figure created using Microsoft Word 365, version 16.96).
Figure 1. Patients and control group (Figure created using Microsoft Word 365, version 16.96). 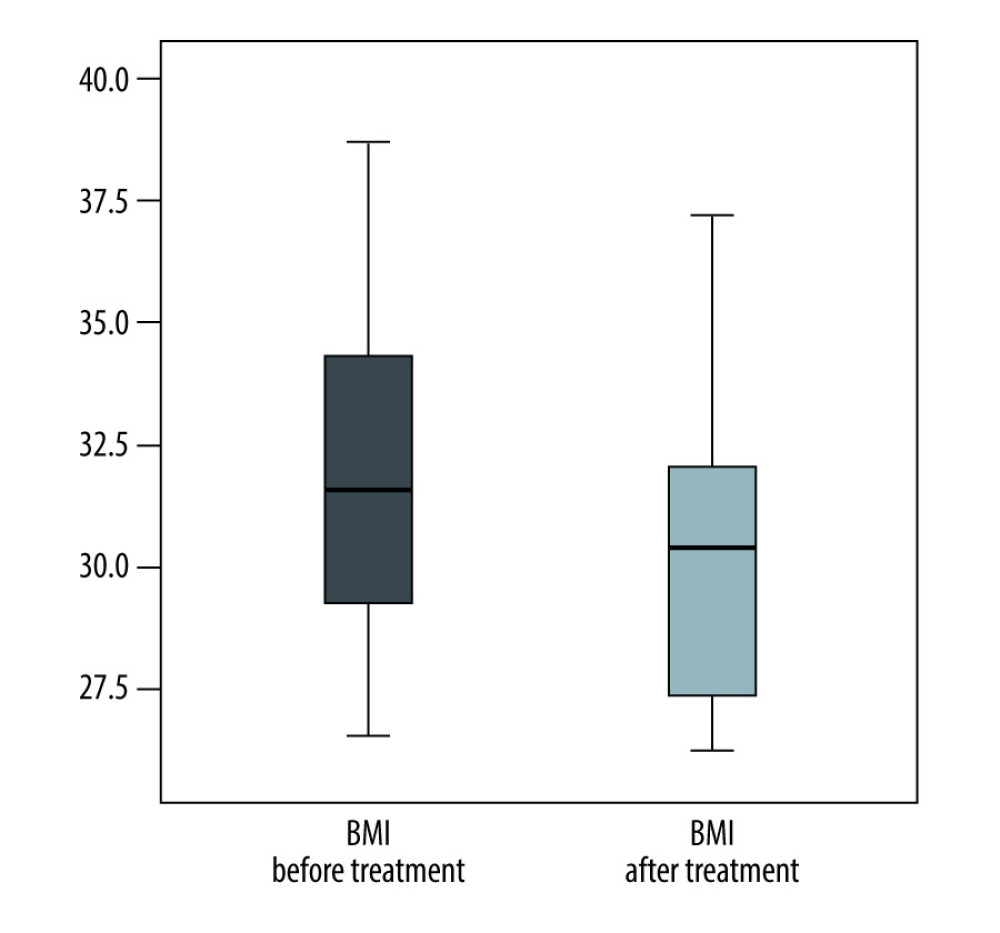 Figure 2. BMI difference after treatment in 30–60% liver steatosis group (Figure created using IBM SPSS Statistics, version 22.0).
Figure 2. BMI difference after treatment in 30–60% liver steatosis group (Figure created using IBM SPSS Statistics, version 22.0). 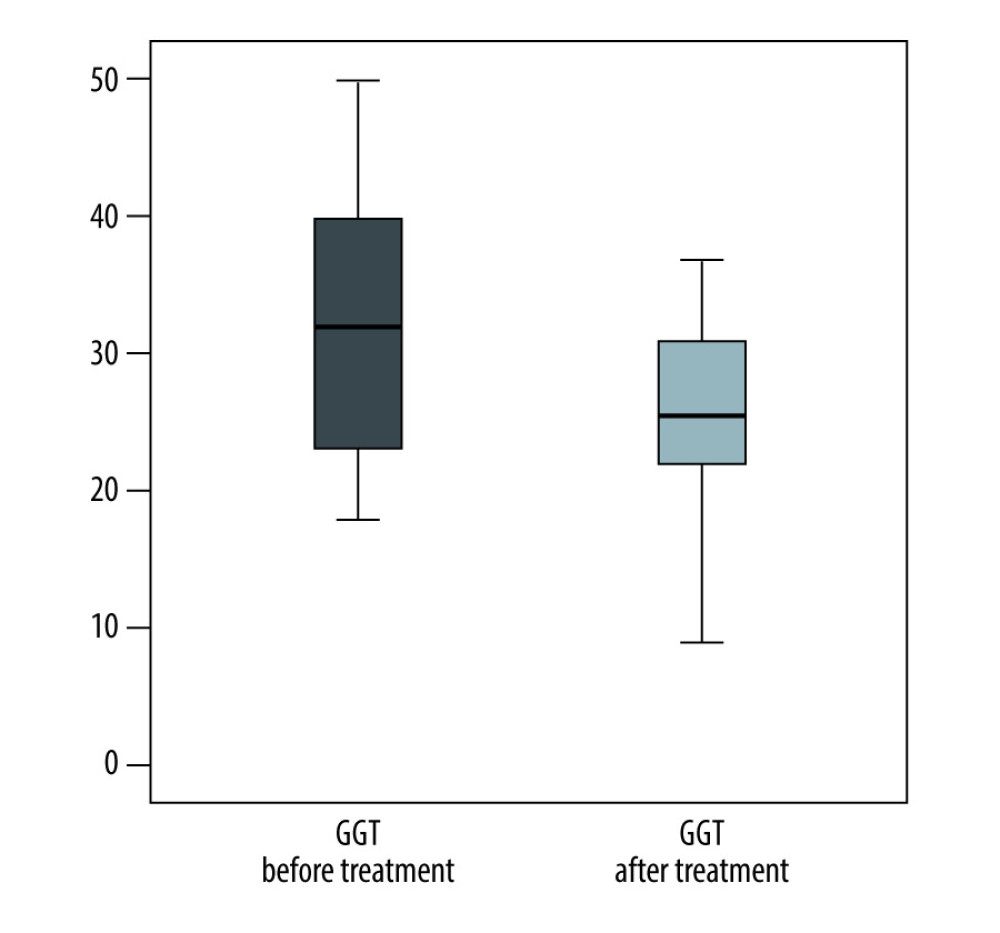 Figure 3. GGT difference after treatment in 30–60% liver steatosis group (Figure created using IBM SPSS Statistics, version 22.0).
Figure 3. GGT difference after treatment in 30–60% liver steatosis group (Figure created using IBM SPSS Statistics, version 22.0). References
1. Roubil JG, Martins PN, Babak M, Resolution of severe graft steatosis before living-donor liver transplant after 86 pounds of weight loss: Exp Clin Transplant, 2022; 20(9); 874-77
2. Kaplan A, Rosenblatt R, Samstein B, Brown RS, Can living donor liver transplantation in the United States reach its potential?: Liver Transpl, 2021; 27(11); 1644-52
3. Turgeon NA, Sollinger HW, Fernandez LA, Hepatic steatosis and liver transplantation: Current Opinion in Organ Transplantation, 2004; 9(2); 123-29
4. Chu MJ, Dare AJ, Phillips AR, Bartlett AS, Donor hepatic steatosis and outcome after liver transplantation: A systematic review: J Gastrointest Surg, 2015; 19(9); 1713-24
5. Younossi ZM, Golabi P, Paik JM, The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): A systematic review: Hepatology, 2023; 77(4); 1335-47
6. Kleiner DE, Brunt EM, Van Natta M, Design and validation of a histological scoring system for nonalcoholic fatty liver disease: Hepatology, 2005; 41(6); 1313-21
7. Tien C, Remulla D, Kwon Y, Emamaullee J, Contemporary strategies to assess and manage liver donor steatosis: A review: Curr Opin Organ Transplant, 2021; 26(5); 474-81
8. Angele MK, Rentsch M, Hartl WH, Effect of graft steatosis on liver function and organ survival after liver transplantation: Am J Surg, 2008; 195(2); 214-20
9. Deroose JP, Kazemier G, Zondervan P, Hepatic steatosis is not always a contraindication for cadaveric liver transplantation: HPB (Oxford), 2011; 13(6); 417-25
10. Doyle MM, Vachharajani N, Wellen JR, Short-and long-term outcomes after steatotic liver transplantation: Arch Surg, 2010; 145(7); 653-60
11. Linares I, Hamar M, Selzner N, Selzner M, Steatosis in liver transplantation: Current limitations and future strategies: Transplantation, 2019; 103(1); 78-90
12. Vogel AS, Roediger R, von Ahrens D, The impact of metabolic health and obesity on liver transplant candidates and recipients: Life (Basel), 2024; 14(6); 685
13. Mantovani A, Dalbeni A, Treatments for NAFLD: State of art: Int J Mol Sci, 2021; 22(5); 2350
14. Eshraghian A, Fattahi MR, Mansourian M, Noninvasive estimation of hepatic steatosis by controlled attenuation parameter in living donor liver transplant: Exp Clin Transplant, 2022; 20(7); 674-79
15. Mortele KJ, Cantisani V, Troisi R, Preoperative liver donor evaluation: Imaging and pitfalls: Liver Transpl, 2003; 9(9); S6-14
16. Noujaim HM, de Ville de Goyet J, Montero EF, Expanding postmortem donor pool using steatotic liver grafts: A new look: Transplantation, 2009; 87(6); 919-25
17. Verran D, Kusyk T, Painter D, Clinical experience gained from the use of 120 steatotic donor livers for orthotopic liver transplantation: Liver Transpl, 2003; 9(5); 500-5
18. Zhang QY, Zhang QF, Zhang DZ, The impact of steatosis on the outcome of liver transplantation: A meta-analysis: Biomed Res Int, 2019; 2019; 3962785
19. Siriwardana RC, Chan SC, Chok KS, Effects of donor steatosis on liver biochemistry and significance of body mass index in predicting steatosis: HPB (Oxford), 2012; 14(9); 619-24
20. Soin AS, Chaudhary RJ, Pahari H, Pomfret EA, A worldwide survey of live liver donor selection policies at 24 centers with a combined experience of 19 009 adult living donor liver transplants: Transplantation, 2019; 103(2); e39-e47
21. Samaha C, Chaaban H, Simsek C, Practice patterns and considerations in liver transplantation from living donors with high BMI: A review: Hepatol Forum, 2023; 4(3); 145-49
22. Moon D, Lee S, Hwang S, Resolution of severe graft steatosis following dual-graft living donor liver transplantation: Liver Transpl, 2006; 12(7); 1156-60
Figures
Figure 1. Patients and control group (Figure created using Microsoft Word 365, version 16.96).Figure 2. BMI difference after treatment in 30–60% liver steatosis group (Figure created using IBM SPSS Statistics, version 22.0).Figure 3. GGT difference after treatment in 30–60% liver steatosis group (Figure created using IBM SPSS Statistics, version 22.0). Tables
 Table 1. Characteristics of study groups (n).
Table 1. Characteristics of study groups (n). Table 2. Preoperative biochemical parameters.
Table 2. Preoperative biochemical parameters. Table 3. Pre-treatment and post-treatment data of patients treated for hepatosteatosis.
Table 3. Pre-treatment and post-treatment data of patients treated for hepatosteatosis. Table 4. Postoperative laboratory parameters (peak levels).
Table 4. Postoperative laboratory parameters (peak levels). Table 5. Liver volumes.Table 1. Characteristics of study groups (n).Table 2. Preoperative biochemical parameters.Table 3. Pre-treatment and post-treatment data of patients treated for hepatosteatosis.Table 4. Postoperative laboratory parameters (peak levels).Table 5. Liver volumes.
Table 5. Liver volumes.Table 1. Characteristics of study groups (n).Table 2. Preoperative biochemical parameters.Table 3. Pre-treatment and post-treatment data of patients treated for hepatosteatosis.Table 4. Postoperative laboratory parameters (peak levels).Table 5. Liver volumes. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988