08 January 2021: Original Paper
Amniotic Fluid Transplantation Alleviates Hematopoietic Deficits in Experimental Rat Aplastic Anemia
Libin Liang1BC, Xiaojun Wang1B, Mingming Li1B, Luyang Qin2B, Xinglong Tong1ACDEF*DOI: 10.12659/AOT.928047
Ann Transplant 2021; 26:e928047






Abstract
BACKGROUND: Hematopoietic stem cell (HSC) transplantation is the most effective therapy for hematopoietic impairment. However, maintenance and self-renewal of HSCs in culture is still a central focus of HSC research. It is known that amniotic fluid contains a heterologous population of stem cells (AFSCs) and nutrients as well as various types of growth factors. We hypothesize that AFSCs may be expanded in vitro in pure amniotic fluid.
MATERIAL AND METHODS: Amniotic fluid with transparent appearance was harvested at embryo age of 13.5–15.5 days in rats and was placed in a cell culture CO₂ incubator. The cell number in the amniotic fluid was counted before and after culture of amniotic fluid. Then, the effect of amniotic fluid transplantation on 5-fluorouracil combined with busulfan induced-rat aplastic anemia was investigated.
RESULTS: We found that after a short time (about 30 min) culture, the number of AFSCs expanded more than 100-fold. Flow cytometry showed that there was a population of cells expressing hematopoietic markers CD45 and CD34 in addition to a higher proportional of mesenchymal stem cells (MSCs) markers CD29 and CD90. Transplantation of the expanded AFSCs possessed significant therapeutic effect in toxic chemicals induced-aplastic anemia rats, manifested by decreasing animal mortality and alleviating the reduction of the 3 lineages of hematopoietic cells in blood.
CONCLUSIONS: Our observation for the first time demonstrates that amniotic fluid is an excellent medium for stem cells to maintain “stemness” proliferation and provides novel evidence to support the potential use of in vitro-expanded AFSCs for the treatment of hematopoietic disorders.
Keywords: Amniotic Fluid, Hematopoiesis, Hematopoietic Stem Cells, Transplantation, Anemia, Aplastic
Background
Hematopoietic stem cell (HSC) transplantation has been considered as an ideal option for hematopoietic diseases including leukemia, aplastic anemia, hematological immunodeficiency, and severe hematopoietic system damage caused by cytotoxic agents and radiation [1]. HSCs are mainly isolated from bone marrow, peripheral blood, and umbilical cord blood cells. Based on the potential clinical applications of HSCs for hematopoietic diseases, many scholars have been trying to culture and expand HSCs
It has become quite clear that amniotic fluid contains different types of stem cells (AFSCs), including multipotent stem cells, mesenchymal stem cells (MSCs), and HSCs, which can express hematopoietic stem cell markers, CD45+/high, CD34+/low, and sca-1/low [3]. Previous experiments by our group and others have found that amniotic fluid contains a certain amount of protein, glucose, and complete inorganic ions, and little fat [4,5]. We assumed that the nutritional composition of amniotic fluid can provide complete support for cellular proliferation [6]. In addition, amniotic fluid is rich in various growth factors [7]. It could be speculated that amniotic fluid provides the signaling required for stem cells to maintain their undifferentiated status [3]. Indeed, it has been reported that a serum-free medium containing 25% amniotic fluid and stem cell factor provides a growth milieu for culture of adult mouse bone marrow HSCs [8]. However, it is still not known if it is possible to expand AFSCs
Material and Methods
ANIMALS:
Sprague-Dawley rats (weighing 220–250 g) were purchased from Vital River Laboratories (Beijing, China), and were housed under pathogen-free conditions and fed a standard rat chow with free access to water and food. All animal care and experimental procedures were approved by the Animal Care and Ethics Committee of Hebei Medical University.
AMNIOTIC FLUID COLLECTION:
Male and female rat were fed and housed in the same cage. Embryo age was defined relative to the morning of vaginal plug discovery (E0.5). The maternal rats were anesthetized with sodium pentobarbital (35 mg·kg−1) and amniotic fluid samples were harvested carefully with a syringe fitted with a 22-gauge needle under aseptic conditions. The amount of amniotic fluid in the amniotic cavity was limited before embryonic days E13.5. The appearance of amniotic fluid was somewhat cloudy over embryonic days E15.5. Therefore, the amniotic fluid at E13.5, E14.5, and E15.5 was used in the study and the appearance of amniotic fluid samples was light-yellow transparent liquid.
BIOCHEMICAL DETERMINATION:
The amniotic fluid samples (2 ml) were taken from rats at E13.5, E14.5, and E15.5. The biochemical components and the levels of organic substances, including total protein, glucose, triglycerides, and cholesterol, in those amniotic fluid samples were quantified using an automatic biochemical analyzer (Hitachi 7180, Japan). Growth factors, including insulin-like growth factor-1, transforming growth factor beta 1, basic fibroblast growth factor-2, vascular endothelial growth factor, and epidermal growth factor, in amniotic fluid of all gestational ages were detected using ELISA kits (Elabscience Biotechnology Co., Ltd., China) according to the manufacturer’s instructions.
:
The amniotic fluid samples were taken from rats at E13.5, E14.5, and E15.5 and the cell number in the amniotic fluid was counted using a cell counting board. The morphology of the cells was observed under a microscope. The amniotic fluid was then placed in a cell culture CO2 incubator. About 30 min later, the cell number was counted again to measure cell expansion. Meanwhile, the precipitated cells were fixed and stained. The ultrastructure of the cells was observed under an electron microscope (Hitachi electron microscope H-600, Japan).
FLOW CYTOMETRY ANALYSIS:
Flow cytometry (BD FACSCalibur flow cytometer, US) was used to determine HSCs markers (CD45, CD34) and MSCs markers (CD29, CD90). All antibodies used for flow cytometry analysis were from Abcom.
EXPERIMENTAL DESIGN FOR AMNIOTIC FLUID TRANSPLANTATION:
A previous report has shown that 5-fluorouracil combined with busulfan can impair the hematopoietic stem cells and resulted in irreversible aplastic anemia in rats [9]. Therefore, aplastic anemia in rats was induced by 5-fluorouracil combined with busulfan in this study to investigate the effect of amniotic fluid transplantation on hematopoietic impairment. Adult rats were randomly divided into a control group and a transplantation group each, with 10 males and 10 females in each group. All rats were i.p. injected with 5-fluorouracil (150 mg/kg) (Tianjin Jinyao Pharmaceutical Co., Ltd., China) and 5 days later were p.o. treated with busulfan (15 mg/kg) (MedChemExpress, U.S) once a week for 2 times. One week later, rats were transplanted with amniotic fluid through intravenous injection at 1 ml. The control group was injected with the same amount of saline. Animal physical appearance and mortality were observed daily. Venous blood samples were taken from the inner canthus of the eye to perform hematological analysis at 3 time points: before and after toxic chemicals, and after amniotic fluid transplantation (Figure 1). The hematological parameters, including the number of red blood cell (RBC), white blood cell (WBC), hemoglobin (HGB), platelet (PLT), reticulocyte (RET), neutrophil granulocyte (NET), lymphocyte (LYMPH), and monocytes (MONO), were measured by an automated hematology analyzer (SYSMEX XT2000, Japan). In addition, at 6 months the surviving rats were killed under deep anesthesia, and femoral bone marrow and spleen tissue were removed and subjected to histopathological examination.
To obtain sufficient amniotic fluid for transplantation, 10~12 maternal rats at E13.5, E14.5, and E15.5 days were used for the therapeutic observation study. All of the amniotic fluid at the same day was collected into a single container, some of which was subjected to flow cytometry analysis. Three kinds of amniotic fluid were transplanted to observe the therapeutic effect on aplastic anemia in rat model to define the component underlying the therapeutic role: (1) fresh amniotic fluid; (2) amniotic fluid cultured
STATISTICAL ANALYSIS:
All data are presented as Mean±SD. Data analysis and statistics was carried out using Origin 8.6 software (OriginLab Corporation, USA). Group comparisons were performed with ANOVA with Dunnett’s post hoc tests. The differences were considered significant at
Results
BIOCHEMICAL COMPONENTS AND GROWTH FACTORS IN RAT AMNIOTIC FLUID:
We first measured the biochemical components of rat amniotic fluid. The levels of proteins, triglyceride, glucose, and electrolytes (Table 1) were similar to those in the human amniotic fluid, as we previously reported [5]. In addition, several growth factors were detected, including insulin-like growth factor-1, transforming growth factor beta-1, basic fibroblast growth factor-2, vascular endothelial growth factor, and epidermal growth factor (Table 2).
:
Fresh amniotic fluid contained small round undifferentiated cells (Figure 2A). Cell counting showed that there were 4.2×104/ml small round cells. Cell culture in pure amniotic fluid induced massive cell proliferation. About 30 min later, there were 4.5×106/ml cells, meaning cells were expanded by more than 100 times. The small round cells were the dominant cell type in amniotic fluid (Figure 2B), indicating an undifferentiated state. However, when amniotic fluid cells were cultured in low-sugar DMEM medium (20% fetal bovine serum), the cells grew adherently with long spindle shapes (Figure 2C), showing a trend of differentiation. Furthermore, we observed the ultrastructure of amniotic fluid cells under electron microscopy. The cellular nucleus of fresh amniotic fluid cells was large, the nuclear chromatin was located under the nuclear membrane, there was less cytoplasm and fewer organelles in the cytoplasm, and there were abundant ribosomes (Figure 2D). After 30 min of amniotic fluid culture in vitro, the cell morphology was similar to that in fresh amniotic fluid, except that the cytoplasm was a little more abundant and the organelles in the cytoplasm were increased, and thus showed a decreased ratio of nucleus to plasma (Figure 2E). However, when the expanded cells covered the culture surface over 80%, the nucleus of the cells became smaller and many autophagosomes were seen in the cytoplasm (Figure 2F), suggesting that the cells were damaged. Based on this observation, we chose this cell density (about 30 min of culture in the pure amniotic fluid) as a proper cell culture condition for cell expansion in vitro.
FLOW CYTOMETRY ANALYSIS OF AMNIOTIC FLUID STEM CELLS:
The amniotic fluid samples from different embryonic days E13.5, E14.5, and E15.5 were cultured in vitro. About 30 min later, amniotic fluid cells were harvested to detect the specific markers of MSCs and HSCs. Figure 3 shows the expression levels of stem cell markers on the different embryonic days by flow cytometry analysis. It revealed that expanded cells in pure amniotic fluid culture contained a high proportion of CD29 (40.3–53.6%) and CD90 (34.7–44.6%) cells, indicating that MSCs were abundant in amniotic fluid. The expression of hematopoietic markers CD45 and CD34 was also identified. The expression of CD45 varied from 32.5% at E13.5 to 22.0% at E15.5, and CD34 displayed a relative lower expression levels with 5.13% at E13.5 and 1.8% at E15.5. The results demonstrated the presence of HSCs in expanded stem cells. In addition, the expression pattern of both CD45 and CD34 showed a trend of higher expression rate at earlier gestational age, suggesting more abundance of HSCs in amniotic fluid at earlier stages of gestation.
EFFECT OF AMNIOTIC FLUID TRANSPLANTATION ON TOXIC CHEMICALS-INDUCED-APLASTIC ANEMIA:
Next, we investigated if amniotic fluid transplantation had a therapeutic effect on toxic chemicals-induced-aplastic anemia in rats. A previous report has shown that 5-fluorouracil combined with busulfan could impair the hematopoietic stem cells and resulted in an irreversible aplastic anemia in rats [9]. Consistent with the report cited above, the present study found that all animals displayed decreased activity and the appearance became pale after applied with busulfan. Some animals died within 1 week after busulfan, with a mortality of about 40% (Figure 4). The dying animals showed bleeding at the mouth, eyes, nose, and anus. Most of the model control group rats died within 30 days, with a mortality rate of 92%. The blood cell count of the aplastic anemia rats revealed a dramatic reduction of erythroid, myeloid, and lymphoid cells compared to pre-treatment (see below). We first observed the effect of fresh amniotic fluid transplantation through intravenous injection at 1 ml. It was found that there was no difference in the animal mortality between the control group (87.5%) and transplanted group (82.5%), indicating that fresh amniotic fluid had no therapeutic effect. Then, we investigated the effectiveness of cultured amniotic fluid. As shown in Figure 4, toxic chemicals induced similar mortality in the 2 groups of animals before transplantation. However, the transplantation of cultured amniotic fluid (about 4.5×106 stem cells per recipient) significantly decreased the mortality of animals at 2 weeks and 6 months after transplantation. Blood parameters analysis showed that the numbers of erythroid, myeloid, and lymphoid cells were significantly higher than those in the control rats (Table 3A). The experiment was repeated another 2 times (about 4.8×106/ml and 4.3×106/ml stem cells per recipient, respectively) and similar results of blood parameters analysis were obtained (Table 3B, 3C). Flow cytometry was repeated 3 times to determine the expression levels of hematopoietic markers CD45 and CD34 of cultured amniotic fluid (CD45: 32.4%, 29.7%, and 30.5% respectively; CD34: 5.12%, 1.27%, and 2.23%, respectively). Cultured amniotic fluid with low expression of HSCs markers (CD45 12.2%, CD34 1.2%) did not show any therapeutic effect on aplastic anemia rats (data not shown).
We next observed the histopathologic changes in hematopoietic tissues after amniotic fluid transplantation. H&E staining and histological examination of bone marrow showed that compared to normal healthy animals, there were significantly fewer hematopoietic cells in control aplastic anemia animals, while cultured amniotic fluid transplantation alleviated hematopoietic impairment (Figure 5A–5C). Meanwhile, splenic staining showed that compensatory extramedullary hematopoiesis was active in aplastic anemia animals, but there was no significant difference between amniotic fluid transplantation animals and normal control animals (Figure 5D–5F). Amniotic fluid contains not only stem cells, but also matrix fluid, in which there are various growth factors. To verify the possible involvement of matrix fluid components in the therapeutic effect, we observed the effect of the supernatant fraction of amniotic fluid cultured in vitro on aplastic anemia model animals using the same method. The results showed that transplantation of amniotic fluid supernatant fraction did not affect the mortality of aplastic anemia rats (data not shown).
Discussion
AMNIOTIC FLUID IS A GOOD MEDIUM FOR MAINTAINING “STEMNESS” PROLIFERATION OF STEM CELLS:
More and more experiments have shown that amniotic fluid contains many types of fetal-derived stem cells, including mesenchymal stem cells, pluripotent stem cells, and monopotent stem cells such as neural stem cells and liver stem cells. In 1993, Torricelli and coworkers first reported a subpopulation of hematopoietic progenitor cells in AF [10]. Subsequently, it was found that human and mouse amniotic fluid cells expressed hematopoietic stem cell markers CD45 and CD34, characterized by CD45/high and CD34/low [3]. The existence of stem cells in amniotic fluid, especially hematopoietic stem cells, may provide a new source of stem cells for the treatment of hematological diseases. To obtain enough cells for therapy, amniotic fluid stem cells (AFSCs) need to be extensively expanded. However, routine serum-containing or serum-free culture in vitro often accelerates the differentiation or apoptosis of hematopoietic stem cells and they lose their amplification ability. Therefore, it is very important to find a culture method to amplify hematopoietic stem cells in vitro. In this study, we observed a striking expansion of AFSCs in pure amniotic fluid of rats. It was found that the number of AFSCs was enlarged by about 100 times within 30 min. The morphology and ultrastructure of expanded cells were quite similar to AFSCs in freshly-collected amniotic fluid, indicating they were in an undifferentiated state. Flow cytometry showed that there was a population of cells expressing hematopoietic markers CD45 and CD34 in expanded AFSCs in addition to abundant expression of mesenchymal stem cells markers. The expression pattern was CD45+/high and CD34+/low, which is consistent with previous reports [3]. The result confirmed that there were hematopoietic stem cells in the amniotic fluid of rats. Our observation demonstrates that amniotic fluid is an excellent medium for stem cells to maintain “stemness” proliferation. A study has shown that human amniotic fluid contains more than 100 different growth and differentiation factors, some of which are known hematopoietic regulators [2]. Indeed, this study showed that as in human amniotic fluid, rat amniotic fluid contained protein, glucose, inorganic ions, and a variety of growth factors. We have postulated that amniotic fluid may act as a transporting pathway for signaling molecules and stem cells during amniote embryonic development [6]. The present results support the notion that the amniotic fluid, with various nutritional components and growth factors, may provide the requirements for stem cell proliferation as well as preservation of their undifferentiated status. A previous report has shown that serum-free medium containing 25% human amniotic fluid provides a growth milieu for adult mouse bone marrow HSC cultures, in which differentiation and apoptosis are downregulated and multipotency is maintained [8]. However, that study found that a concentration of human amniotic fluid >25% is toxic to the cells. The discrepancy may be due to the lack of a good balance between the requirements of HSCs growth and supply by human amniotic fluid in that experimental condition since the concentrations of signaling molecules in amniotic fluid show a dynamic pattern during embryonic development.
AFSCS TRANSPLANTATION CAN PRODUCE AN EFFECTIVE THERAPEUTIC EFFECT IN APLASTIC ANEMIA RATS:
Stem cell transplantation is an important method for the treatment of hematological diseases. We found that direct transplantation of freshly-collected amniotic fluid did not show any effect in aplastic anemia rats, although amniotic fluid contained a certain number of stem cells. Obviously, the limited number of AFSCs could not recover impaired hematopoietic function. Expanded AFSCs in pure amniotic fluid did show a significant therapeutic effect in aplastic anemia rats. The effectiveness was manifested by decreasing animal mortality, alleviating the reduction in the 3 lineages of hematopoietic cells. Bone marrow staining showed that the reduction of hematopoietic cells was reversed and spleen extramedullary hematopoiesis was alleviated accordingly. The supernatant of the amniotic fluid had no therapeutic effect, indicating that the therapeutic effect primarily came from the stem cells. It is known that aplastic anemia is characterized by a loss or dysfunction of HSCs [11]. We speculated that HSCs in the amniotic fluid engrafted in damaged bone marrow hematopoietic system to differentiate multiple lineages of hematopoietic cells. This was confirmed by our finding that expanded AFSCs did not show any effectiveness when there was a lower percentage of CD45+ cells (12.2% compared to more than 30%).
Another pathogenetic mechanism for aplastic anemia may involve an abnormal bone marrow microenvironment, which affects the proliferation, differentiation, and self-renewal of HSCs [11]. Increasing evidence has demonstrated that bone marrow mesenchymal stem cells (BMSCs) are an important component of the bone marrow microenvironment and play an important role in maintaining hematopoietic stem cells [12–14]. A study has shown that BMSCs promote the hematopoietic microenvironment for hematopoietic recovery after bone marrow transplantation [12]. In this study, a higher proportional of MSCs was found in the expanded AFSCs. Accordingly, MSCs in amniotic fluid may also contribute to the hematopoietic recovery. It is thus speculated that amniotic fluid transplantation may be as effective as bone marrow transplantation for the treatment of hematopoietic disorders, since the amniotic fluid contains different types of stem cells and so many growth factors, which may synergistically contribute to recover of damaged hematopoietic function. The histological examination showed that, compared to normal healthy animals, the percentage of bone marrow hematopoietic cells in aplastic anemia animals significantly decreased, while cultured amniotic fluid transplantation alleviated the hematopoietic impairment. Flow cytometry (repeated 3 times) determined the expression levels of hematopoietic markers CD45 and CD34 in cultured amniotic fluid (CD45: 32.4%, 29.7%, and 30.5% respectively; and CD34: 5.12%, 1.27%, and 2.23%, respectively). Above results indicated that HSCs in the amniotic fluid engrafted in the damaged bone marrow hematopoietic system to differentiate multiple lineages of hematopoietic cells. In addition, another pathogenetic mechanism for aplastic anemia may involve an abnormal bone marrow microenvironment, which affects the proliferation, differentiation, and self-renewal of HSCs [11]. A study has shown that bone marrow mesenchymal stem cells promote the hematopoietic microenvironment for hematopoietic recovery after bone marrow transplantation [12]. In this study, a higher proportional of MSCs was found in the expanded AFSCs. Accordingly, MSCs in amniotic fluid may also contribute to the hematopoietic recovery. It is thus speculated that amniotic fluid transplantation may be as effective as bone marrow transplantation for the treatment of hematopoietic disorders, since the amniotic fluid contains different types of stem cells and so many growth factors, which may synergistically contribute to recover damaged hematopoietic function. Moreover, we found that cultured amniotic fluid with low expression of HSCs markers (12.2% for CD45, 1.2% for CD34) did not show any therapeutic effect in aplastic anemia rats (data not shown). The result further confirmed the dominant role of HSCs in the hematopoietic recovery for aplastic anemia rats.
Conclusions
In summary, we for the first time uncovered a striking expansion of AFSCs when cultured
Figures
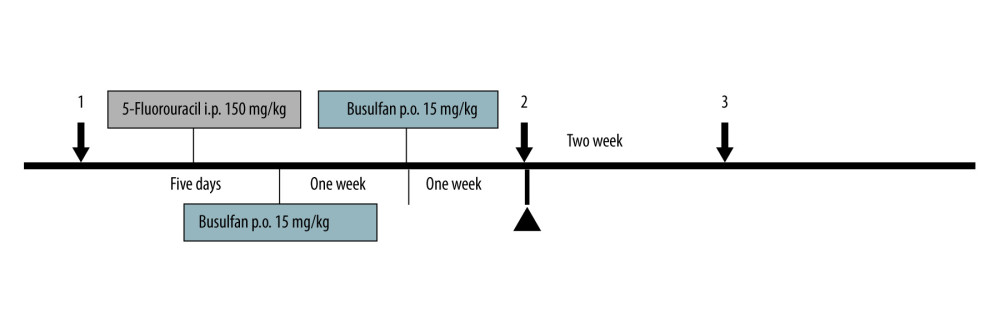 Figure 1. The schematic design for amniotic fluid transplantation. Black arrows represent the time points at which peripheral blood was obtained for analysis. Black triangle indicates the amniotic fluid (or saline as control) transplantation.
Figure 1. The schematic design for amniotic fluid transplantation. Black arrows represent the time points at which peripheral blood was obtained for analysis. Black triangle indicates the amniotic fluid (or saline as control) transplantation. 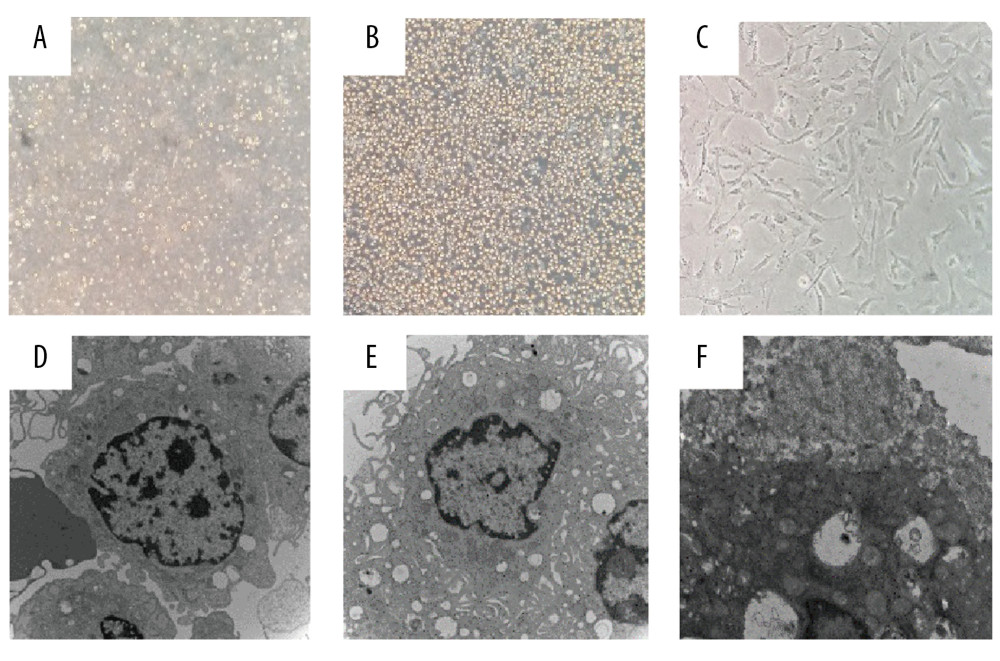 Figure 2. AFSCs in vitro expansion in pure amniotic fluid. (A) AFSCs in freshly-collected amniotic fluid (40×). (B) AFSCs in vitro cultured in pure amniotic fluid for 30 min (40×). (C) AFSCs cultured for 48 h in DMEM medium (20% serum) (40×). (D) Ultrastructure of AFSCs in freshly-collected amniotic fluid. (E) Ultrastructure of AFSCs after cultured in pure amniotic fluid. (F) Autophagosomes were observed in the cytoplasm when the expanded cells covered over 80% of the culture surface.
Figure 2. AFSCs in vitro expansion in pure amniotic fluid. (A) AFSCs in freshly-collected amniotic fluid (40×). (B) AFSCs in vitro cultured in pure amniotic fluid for 30 min (40×). (C) AFSCs cultured for 48 h in DMEM medium (20% serum) (40×). (D) Ultrastructure of AFSCs in freshly-collected amniotic fluid. (E) Ultrastructure of AFSCs after cultured in pure amniotic fluid. (F) Autophagosomes were observed in the cytoplasm when the expanded cells covered over 80% of the culture surface. 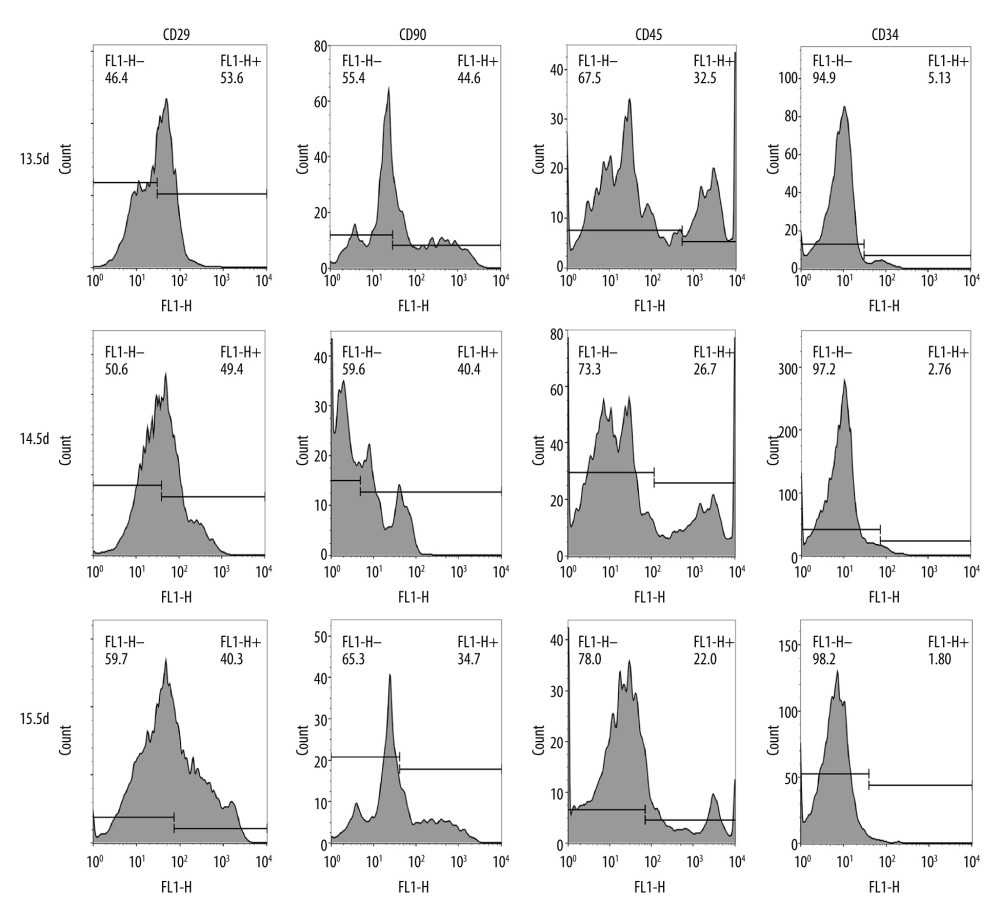 Figure 3. Results for flow cytometry analysis. Expression of MSCs (CD29 and CD90) and hematopoietic surface markers (CD45 and CD34) was detected in expanded AFSCs on different embryonic days.
Figure 3. Results for flow cytometry analysis. Expression of MSCs (CD29 and CD90) and hematopoietic surface markers (CD45 and CD34) was detected in expanded AFSCs on different embryonic days. 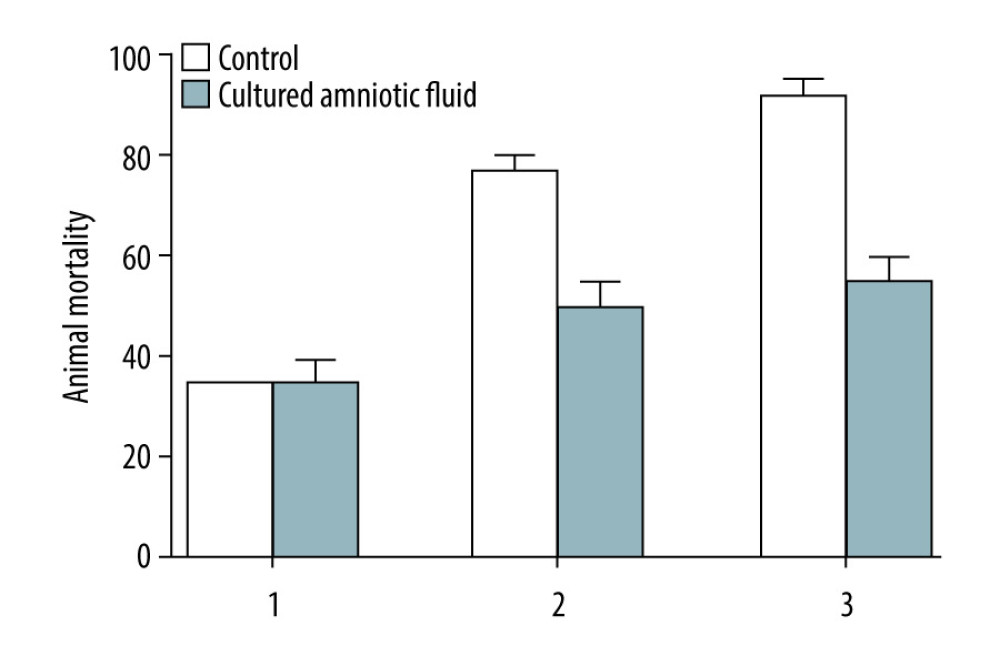 Figure 4. Effect of cultured amniotic fluid on mortality of aplastic anemia rats at different time points. 1 and 2 represent 1 week after the first dose and the second dose of busulfan, respectively, and 3 represents 2 weeks after amniotic fluid transplantation.
Figure 4. Effect of cultured amniotic fluid on mortality of aplastic anemia rats at different time points. 1 and 2 represent 1 week after the first dose and the second dose of busulfan, respectively, and 3 represents 2 weeks after amniotic fluid transplantation. 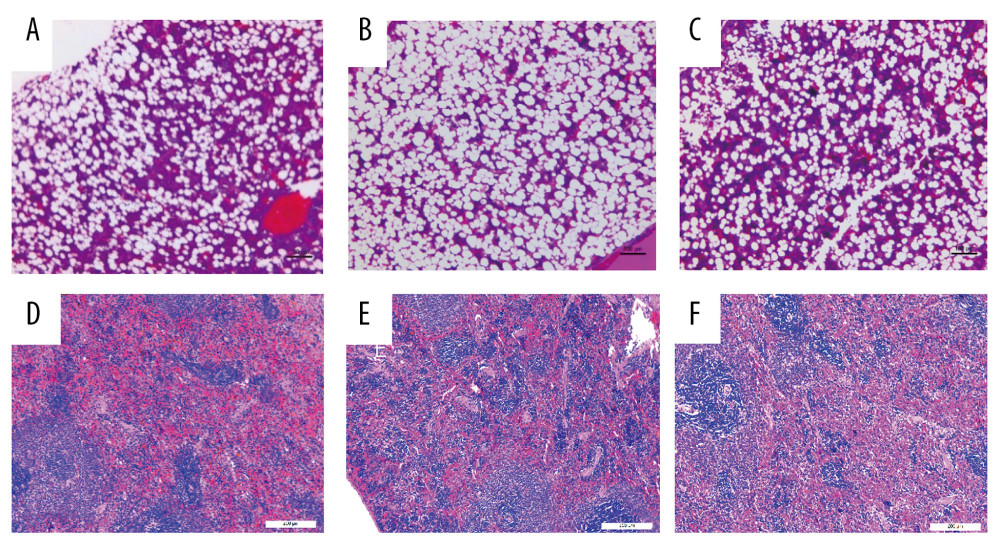 Figure 5. Histopathologic changes in bone marrow and splenic hematopoietic tissue after amniotic fluid transplantation. (A) Bone marrow from a normal healthy animal. (B) Bone marrow from an aplastic anemia rat; the hematopoietic cells significantly decreased compared to normal healthy animal. (C) Bone marrow from an aplastic anemia rat post amniotic fluid transplantation. The number of hematopoietic cells was very similar to that in healthy animals. (D) Splenic hematopoietic tissue from a normal healthy animal. (E) Splenic hematopoietic tissue from an aplastic anemia animal; compensatory extramedullary hematopoiesis was active. (F) Splenic hematopoietic tissue from an aplastic anemia rat after amniotic fluid transplantation; there was no obvious extramedullary hematopoiesis.
Figure 5. Histopathologic changes in bone marrow and splenic hematopoietic tissue after amniotic fluid transplantation. (A) Bone marrow from a normal healthy animal. (B) Bone marrow from an aplastic anemia rat; the hematopoietic cells significantly decreased compared to normal healthy animal. (C) Bone marrow from an aplastic anemia rat post amniotic fluid transplantation. The number of hematopoietic cells was very similar to that in healthy animals. (D) Splenic hematopoietic tissue from a normal healthy animal. (E) Splenic hematopoietic tissue from an aplastic anemia animal; compensatory extramedullary hematopoiesis was active. (F) Splenic hematopoietic tissue from an aplastic anemia rat after amniotic fluid transplantation; there was no obvious extramedullary hematopoiesis. Tables
Table 1. Measurement of components in rat amniotic fluid (AF). n=6, mean±SD.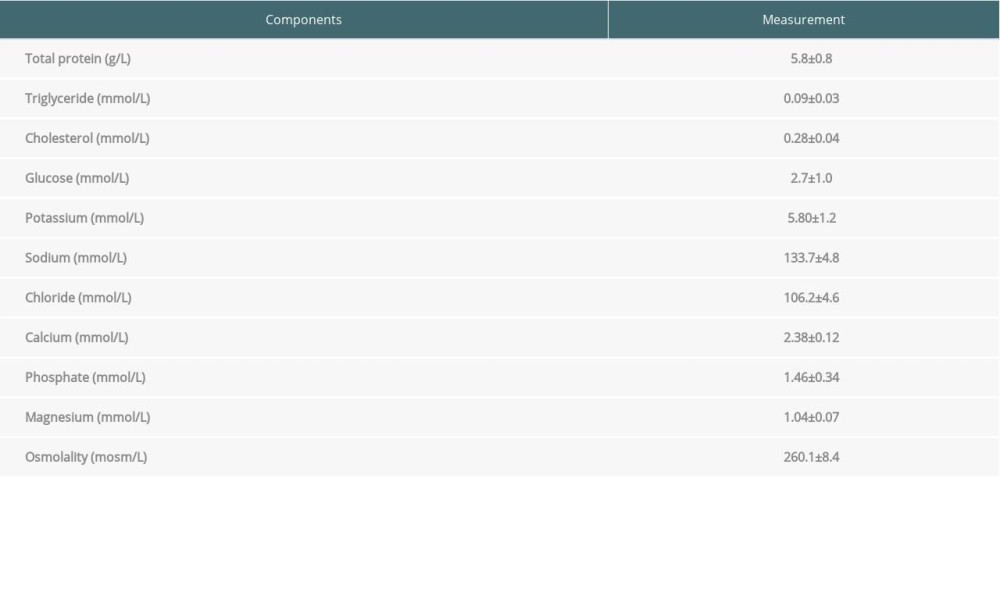 Table 2. Measurement of growth factors in rat amniotic fluid. n=6, mean±SD.
Table 2. Measurement of growth factors in rat amniotic fluid. n=6, mean±SD.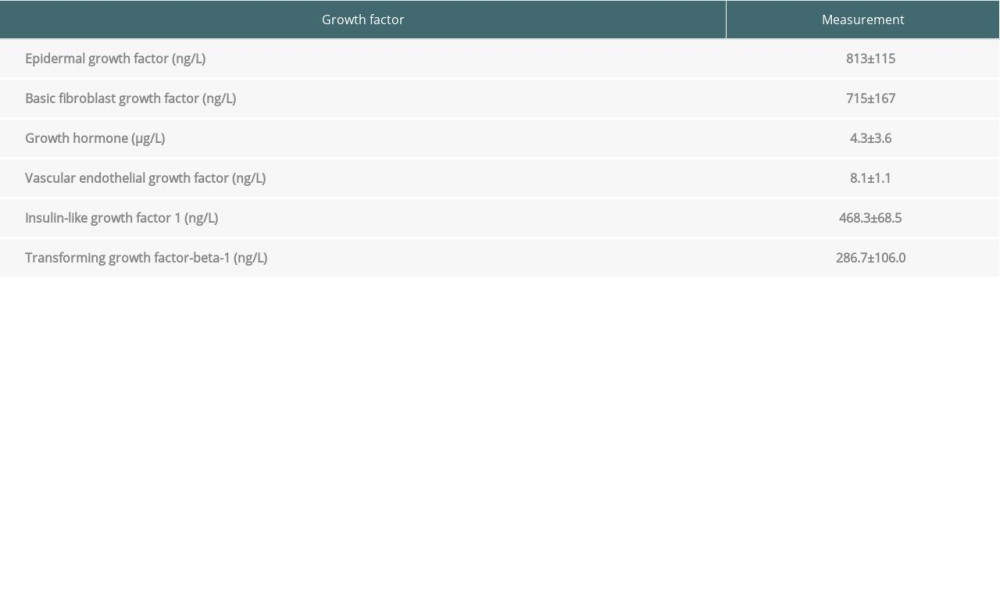 Table 3A. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD.
Table 3A. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD. Table 3B. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD.
Table 3B. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD. Table 3C. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD.
Table 3C. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD.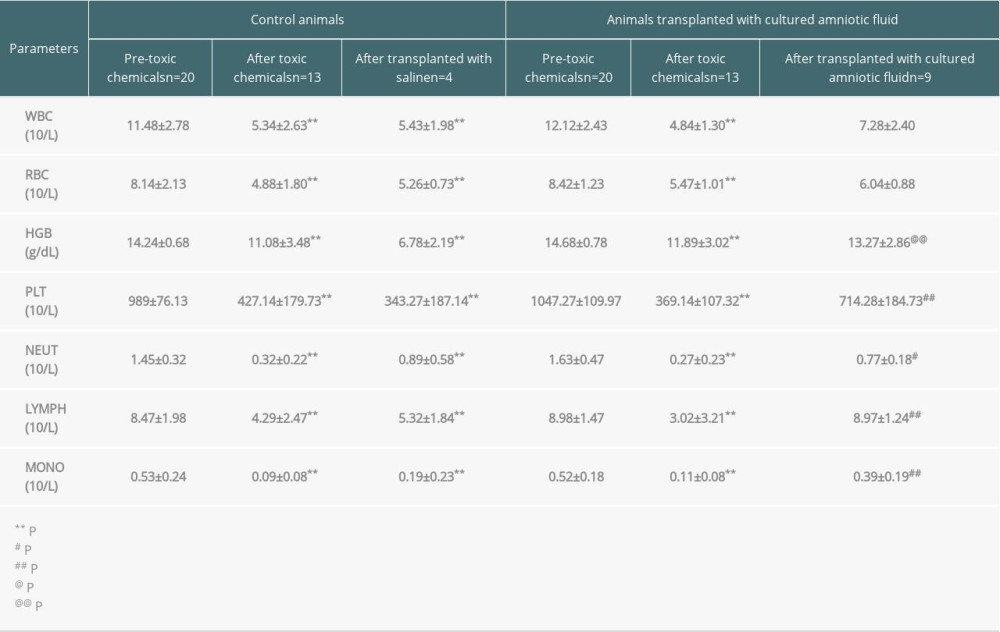
References
1. Copelan EA, Hematopoietic stem-cell transplantation: N Engl J Med, 2006; 354(17); 1813-26
2. Cho CK, Shan SJ, Winsor EJ, Diamandis EP, Proteomics analysis of human amniotic fluid: Mol Cell Proteomics, 2007; 6(8); 1406-15
3. Loukogeorgakis SP, De Coppi P, Concise review: Amniotic fluid stem cells: The known, the unknown, and potential regenerative medicine applications: Stem Cells, 2017; 35(7); 1663-73
4. Burdett P, Lizana J, Eneroth P, Bremme K, Proteins of human amniotic fluid. II. Mapping by two-dimensional electrophoresis: Clin Chem, 1982; 28(4 Pt 2); 935-40
5. Tong XL, Wang L, Gao TB, Potential function of amniotic fluid in fetal development – novel insights by comparing the composition of human amniotic fluid with umbilical cord and maternal serum at mid and late gestation: J Chin Med Assoc, 2009; 72(7); 368-73
6. Tong X, Amniotic fluid may act as a transporting pathway for signaling molecules and stem cells during the embryonic development of amniotes: J Chin Med Assoc, 2013; 76(11); 606-10
7. Blahovec J, Kostecka Z, Cavaille F, Insulin-like growth factor binding proteins and mitogenic activity of partially fractionated sheep amniotic fluid: Acta Vet Hung, 2001; 49(1); 65-70
8. Barria E, Mikels A, Haas M, Maintenance and self-renewal of long-term reconstituting hematopoietic stem cells supported by amniotic fluid: Stem Cells Dev, 2004; 13(5); 548-62
9. Zhao J, Chu J, Ding SA novel rat aplastic anemia model induced by 5-fluorouracil combined with busulfan: Zhonghua Xue Ye Xue Za Zhi, 2001; 22(4); 202-4 [in Chinese]
10. Torricelli F, Brizzi L, Bernabei PA: Ital J Anat Embryol, 1993; 98(2); 119-26
11. Wang L, Liu H, Pathogenesis of aplastic anemia: Hematology, 2019; 24(1); 559-66
12. Mendez-Ferrer S, Michurina TV, Ferraro F, Mesenchymal and haematopoietic stem cells form a unique bone marrow niche: Nature, 2010; 466(7308); 829-34
13. Szade K, Gulati GS, Chan CKF, Where hematopoietic stem cells live: The bone marrow niche: Antioxid Redox Signal, 2018; 29(2); 191-204
14. Wu J, Zhang W, Ran Q, The differentiation balance of bone marrow mesenchymal stem cells is crucial to hematopoiesis: Stem Cells Int, 2018; 2018 1540148
Figures
Figure 1. The schematic design for amniotic fluid transplantation. Black arrows represent the time points at which peripheral blood was obtained for analysis. Black triangle indicates the amniotic fluid (or saline as control) transplantation.Figure 2. AFSCs in vitro expansion in pure amniotic fluid. (A) AFSCs in freshly-collected amniotic fluid (40×). (B) AFSCs in vitro cultured in pure amniotic fluid for 30 min (40×). (C) AFSCs cultured for 48 h in DMEM medium (20% serum) (40×). (D) Ultrastructure of AFSCs in freshly-collected amniotic fluid. (E) Ultrastructure of AFSCs after cultured in pure amniotic fluid. (F) Autophagosomes were observed in the cytoplasm when the expanded cells covered over 80% of the culture surface.Figure 3. Results for flow cytometry analysis. Expression of MSCs (CD29 and CD90) and hematopoietic surface markers (CD45 and CD34) was detected in expanded AFSCs on different embryonic days.Figure 4. Effect of cultured amniotic fluid on mortality of aplastic anemia rats at different time points. 1 and 2 represent 1 week after the first dose and the second dose of busulfan, respectively, and 3 represents 2 weeks after amniotic fluid transplantation.Figure 5. Histopathologic changes in bone marrow and splenic hematopoietic tissue after amniotic fluid transplantation. (A) Bone marrow from a normal healthy animal. (B) Bone marrow from an aplastic anemia rat; the hematopoietic cells significantly decreased compared to normal healthy animal. (C) Bone marrow from an aplastic anemia rat post amniotic fluid transplantation. The number of hematopoietic cells was very similar to that in healthy animals. (D) Splenic hematopoietic tissue from a normal healthy animal. (E) Splenic hematopoietic tissue from an aplastic anemia animal; compensatory extramedullary hematopoiesis was active. (F) Splenic hematopoietic tissue from an aplastic anemia rat after amniotic fluid transplantation; there was no obvious extramedullary hematopoiesis. Tables
Table 1. Measurement of components in rat amniotic fluid (AF). n=6, mean±SD.Table 2. Measurement of growth factors in rat amniotic fluid. n=6, mean±SD.Table 3A. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD.Table 3B. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD.Table 3C. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD.Table 1. Measurement of components in rat amniotic fluid (AF). n=6, mean±SD.Table 2. Measurement of growth factors in rat amniotic fluid. n=6, mean±SD.Table 3A. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD.Table 3B. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD.Table 3C. Effect of cultured amniotic fluid transplantation on blood parameters. Data were expressed as mean±SD. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988