20 August 2021: Original Paper
Color Doppler Ultrasound and Hemodynamics for Evaluating Graft Dysfunction in Recurrent Immunoglobulin A Nephropathy
Jin Zhang12ABCDEF, Guo-Dong Chen2ABCEF, Jiang Qiu2AFG*, Yang Tan3ABCD, Guo-Chang Liu1AFG, Li-Zhong Chen2AG, Wei Jia1ABD, Wen Fu1ABD, Chang-Xi Wang2AGDOI: 10.12659/AOT.931736
Ann Transplant 2021; 26:e931736






Abstract
BACKGROUND: The aim of this study was to investigate the diagnostic and prognostic utility of color Doppler ultrasound for graft dysfunction in recurrent immunoglobulin A nephropathy (IgAN).
MATERIAL AND METHODS: We selected a series of 78 biopsies diagnostic of recurrent IgAN following living-donor transplantation from July 2004 to January 2019. Based on Lee’s classification, Doppler parameters in different degrees of histopathological injury were retrospectively analyzed.
RESULTS: The 4-year cumulative graft survival rate after biopsy was 66.3%, and the difference among the Kaplan-Meier curves of Lee’s classification (P<0.01) was significant. Doppler parameters showed that echo enhancement, decreasing blood flow distribution, decreasing end-diastolic velocity (EDV) of the main renal artery (MRA), segmental renal atery (SRA) and interlobar renal artery (IRA), and an elevated resistance index (RI) of the arcuate renal artery (ARA) were significantly different among grades I-V of Lee’s classification (P<0.05). Logistic multivariate analysis indicated that echo enhancement (HR 13.6, 95% CI 2.7-68.4) and decreasing EDV of the SRA (HR 1.1 for a 1-cm/s, 95% CI 1.0-1.2) were independent predictors of severe injury (IV-V). The ROC curve fitted by echo enhancement and decreasing EDV of the SRA had an area under the curve of 0.87. The cutoff was 17.5 cm/s (decreasing EDV of the SRA) without echo enhancement. The sensitivity and specificity were 72.2% and 91.7%, respectively.
CONCLUSIONS: Color Doppler ultrasound successfully evaluated the graft dysfunction in recurrent IgAN; a decreasing EDV of the SRA indicated severe histopathological injury and poor prognosis.
Keywords: Agalactoimmunoglobulin A1, Primary Graft Dysfunction, Ultrasonography, Doppler, Glomerulonephritis, IGA, Hemodynamics, Kidney, Ultrasonography, Doppler, Color
Background
With the improved survival of renal allografts following transplantation, recurrent renal disease is considered an important cause of graft dysfunction, which is the second and the third leading cause of death-censored and uncensored graft failure, respectively [1].
As the most common recurrent renal disease [2,3], immunoglobulin A nephropathy (IgAN) has been reported to recur in 33% (9% to 61%) of recipients, occurred frequently in living-donor transplantation, and indicated a risk of graft failure [4,5]. A protocol biopsy after transplantation has been recommended to detect recurrence and disease progression for patients with a high risk of recurrence, but its safety and adequacy have been criticized due to related complications [6]. To investigate non-invasive methods for evaluating the graft dysfunction of recurrent IgAN, we assessed the diagnostic value of color Doppler ultrasound.
Material and Methods
SAMPLE COLLECTION:
A series of 78 patients with recurrent IgAN following living transplantation from July 2004 to January 2019 at our center were diagnosed by biopsies of native and renal allografts. The biopsies of renal allografts were performed from June 2007 to September 2019, with specimens including 65 indication biopsies and 13 protocol biopsies. Cases with comorbid chronic rejection, calcineurin inhibitor (CNI) toxicity damage, or BK virus-associated nephropathy (BKVAN) were excluded. The specimens were derived from 17 women and 61 men (mean age 34.3±9.5 years).
The patients underwent color Doppler ultrasound for renal allografts at 1, 7, and 14 days after transplantation and every 3 months during follow-up, performed in Guangzhou Women’s and Children’s Medical Center (Guangzhou, China) and the First Affiliated Hospital of Sun Yat-sen University (Guangzhou, China). We simultaneously recorded 24-h urinary protein, estimated glomerular filtration rate (eGFR) (estimated by the Chronic Kidney Disease Epidemiology collaboration [CKD-EPI] equation), and other clinical indexes. Table 1 lists the clinical indexes and therapeutic regimens for patients after recurrence.
This retrospective analytical study was approved by the Regional Ethics Committee of our center. All patients signed informed consent forms, and no interventions were performed as part of this study.
ULTRASONIC DIAGNOSIS AND BIOPSY OF RECURRENT IGAN:
The ultrasonic diagnosis was performed with an Aplio 500 color Doppler ultrasound machine and convex probes (Toshiba, Japan). At the times of the lowest serum creatinine (sCr) level and the biopsy diagnosis, the following ultrasound data were recorded by 2 trained, double-blinded sonographers:
A needle biopsy with an 18-gauge needle (Bard, USA) was guided by ultrasonography. Each sample was stained with hematoxylin-eosin and periodic acid-Schiff. Immunofluorescence were performed using polyclonal antibodies against IgA, IgG, IgM, C3, C4D, and C1q. According to 2012 KDIGO clinical practice guideline for glomerulonephritis, we defined a diagnosis of IgAN as IgA positivity deposited in the mesangial area of immunofluorescence staining, a similar feature caused by lupus nephritis, hepatitis B virus-associated glomerulonephritis, or other diseases with a clear etiology excluded [8]. The degree of histopathological injury was categorized as grade I–V based on Lee’s classification [9].
STATISTICAL ANALYSIS:
To test the prognostic predictive value of Lee’s classification, we analyzed the 4-year cumulative graft survival rate after biopsy. The graft survival curves were created by Kaplan-Meier Estimator, and comparisons among grades I–V of Lee’s classification were performed using the log-rank test.
Based on Lee’s classification, we compared the Doppler parameters among different degrees of histopathological injury. Variables were compared by the Kruskal-Wallis test and the chi-squared test, and
Logistic multivariate analysis was used to explore the significance of ultrasonic and hemodynamic factors related to histopathological injury and to investigate the diagnostic value of these predictive factors. The sensitivity and specificity of each factor were evaluated by a receiver operating characteristic (ROC) curve, and
The data were analyzed using the software package IBM SPSS Statistics version 22.0.
Results
After a mean follow-up of 3.3±1.7 years, 44 patients finished the 4-year observation period, and graft failure occurred in 16 patients; we defined this endpoint as the return to routine dialysis for more than 3 months. The 4-year cumulative graft survival rate after biopsy was 66.3%. The log-rank test suggested that the difference among the Kaplan-Meier curves of Lee’s classification (
We observed that echo enhancement (
Logistic univariate and multivariate analyses indicated that echo enhancement (hazard ratio [HR] 13.6, 95% confidence interval [CI] 2.7–68.4), and decreasing EDV of the SRA (HR 1.1 for a 1 cm/s, 95% CI 1.0–1.2) were independent predictors of severe injury (Table 4, Figure 2). The ROC curves of echo enhancement and decreasing EDV of the SRA had area under the curve (AUC) values of 0.76 and 0.77, respectively. The ROC fitted by these 2 indexes had an AUC of 0.87 (Figure 3), an ideal cutoff point of 17.5 cm/s (decreasing EDV of the SRA) without echo enhancement, and sensitivity and specificity of 72.2% and 91.7%, respectively (Table 5).
Discussion
Color Doppler ultrasound is widely used to detect graft dysfunction [10,11]. Early research [12] showed that it is possible to detect acute rejection 5 days after transplantation. Sharma et al [11] analyzed 6017 ultrasonic scans performed in 614 patients with 462 episodes of acute rejection from 1992 to 2000, and reported that a >10% increase over the previous ‘best’ RI had a sensitivity of 60% and a specificity of 90% for the diagnosis of acute rejection. Dugo et al [13] found that ultrasound showed typical hypoechoic lesions with irregular edges in the cortex of BKVAN patients, suggesting that ultrasound can be useful for the non-invasive diagnosis of BKVAN when combined with blood and urine screening tests. Cano et al [14] reviewed the literature from the past 10 years and concluded that an elevated RI is an early predictor of histologically relevant chronic allograft nephropathy. The application of novel techniques like contrast-enhanced ultrasound (CEUS) and shear-wave elastography (SWE), to a large extent, improved the diagnostic value of ultrasound. Elec et al [15] conducted a cross-sectional study of the early post-transplantation period and found that patients with delayed graft function showed lower values for wash-out area under the curve and wash-in and wash-out area under the curve in CEUS, which may be useful to diagnose delayed graft function. Using SWE, Bolboaca et al [16] identified the differences among stable graft function and graft dysfunction. It has been demonstrated that the cortical tissue stiffness provided significantly higher values for patients with graft dysfunction as compared to patients with stable function. However, its utility in recurrent renal disease remains unknown.
Recent studies confirmed that recurrent IgAN reduced the long-term graft survival [5,17]. These conclusions were inconsistent with early research suggesting that it had a benign prognosis with little impact on graft function [18], especially in patients with continuous hematuria or proteinuria. Although a decreased eGFR or severe proteinuria as the initial symptom were considered as predictive factors of graft failure [19,20], these initial symptoms are not common in recurrent IgAN, and only 17 patients (21.8%) presented an early increase in sCr in this series. Ortiz et al [21] found that histopathological injury occurred in half of early recurrent IgAN patients without abnormalities in urinalysis, which means clinically silent patients may have severe histopathological injury on biopsy.
The evaluation criteria of Lee’s classification, based on and recommended for East Asian patients, include glomerular sclerosis and mesangial proliferation, crescent formation, interstitial inflammation, and tubular atrophy (IF/TA). In a previous study, we confirmed the predictive value of this classification in IgAN in renal allografts [19]. Our findings indicate that patients with grade IV–V injury may have a significant risk of graft failure, which is completely consistent with that used in native IgAN [9]. Moreover, an abnormal echo and blood flow have been observed in patients with severe histopathological injury; timely therapy and prevention of risk factors for graft failure could be performed according to these ultrasonic characteristics, and repeated protocol biopsies could be avoided for recurrent IgAN patients.
The histopathological injury of IgAN is manifested as IgA, complement C3, C1q, and their immune complex deposited in the mesangial area, which leads to glomerular mesangial proliferation and endocapillary hypercellularity. The basement membrane is fragmented and absent when it invades the proliferative mesangial matrix, resulting in segment glomerular sclerosis and cellular/fibrocellular crescent formation with IF/TA. Echo enhancement, which denotes glomerulosclerosis and interstitial fibrosis, is a typical feature of graft dysfunction, as it appears in chronic glomerulonephritis [22]. Echo enhancement occurred in 16 cases (20.5%) in this series and in 11 cases (68.7%) of severe injury; this result indicates an excellent specificity of 91.7% and a lower sensitivity of 61.1%. In recent studies, the echo intensity (EI) was measured as a quantitative parameter to detect renal ischemia-reperfusion and parenchyma lesions [23,24]. Considering the slow and concealed disease progression, we support the use of the EI combined with hemodynamic indexes to improve the sensitivity of graft dysfunction in further studies.
Hemodynamic indexes such as EDV and RI have been confirmed to be valuable markers for graft function and related vascular complications; early research [25] suggested that renal disease can be diagnosed when RI >0.65 in the IRA. Cano et al [14] found that when RI equals 1 (absent end-diastolic flow) in the first weeks after transplantation, it is associated with acute tubular necrosis and impaired renal graft recovery. Kolonko et al [26] concluded that high RI in SRA in the very early post-transplantation period predicts worse graft function and an increased risk of all-cause graft failure, including patient death, in the 5-year follow-up period. In contrast, Maarten et al [27] showed that recipients with higher RI had higher mortality than the risk of graft failure, and it was not associated with histopathological injury. Similar to the result of Kolonko et al, we found that the RI was <0.7 in most cases with good graft function and normal biopsy. Considering that the baseline level after transplantation might be influenced by medicine and donor vascular factors, we suggest that the hemodynamic change in the period from the lowest sCr level to biopsy is more significant than a single scan in evaluating graft function. In severe cases, we noted that the hemodynamic changes in SRA had more significance than in IRA and ARA, which is inconsistent with the initial histopathological changes of IgAN, characterized by myointimal thickening in arterioles (IRA, ARA, and interlobular renal artery). These features of SRA and its superior arteries were rare in patients with mild injury, whose histopathological changes were mostly limited to the IRA and its inferior arteries. Thus, hemodynamic changes indicate severe injury and poor prognosis when they progress to SRA, and they could be a valuable marker to detect the graft dysfunction of recurrent IgAN.
Our study demonstrated that Doppler parameters can be used to evaluate the graft dysfunction of recurrent IgAN. We aimed to provide non-invasive methods to help patients avoid repeated protocol biopsies, but all of the above results were obtained based on diagnostic biopsies for recurrent IgAN, which could not be replaced by clinical and ultrasonic diagnosis. Ultrasound cannot differentiate pathological types of graft dysfunction. In addition, the ultrasound results could be influenced by handlers’ skill and experience. Further studies and a longer-term follow-up are required to verify their diagnostic values.
Conclusions
With the non-invasive methods of color Doppler ultrasound, we successfully evaluated graft dysfunction. A decreasing EDV of the SRA indicates severe histopathological injury and poor prognosis. Thus, repeated protocol biopsies can be avoided for recurrent IgAN patients.
Figures
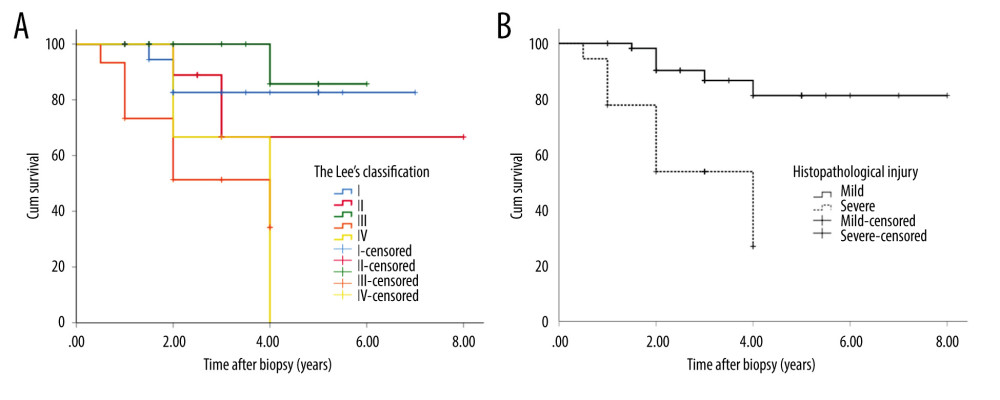 Figure 1. Kaplan-Meier curves of Lee’s classification (A) and histopathological injury (B) (SPSS Statistics, 22.0, IBM).
Figure 1. Kaplan-Meier curves of Lee’s classification (A) and histopathological injury (B) (SPSS Statistics, 22.0, IBM). 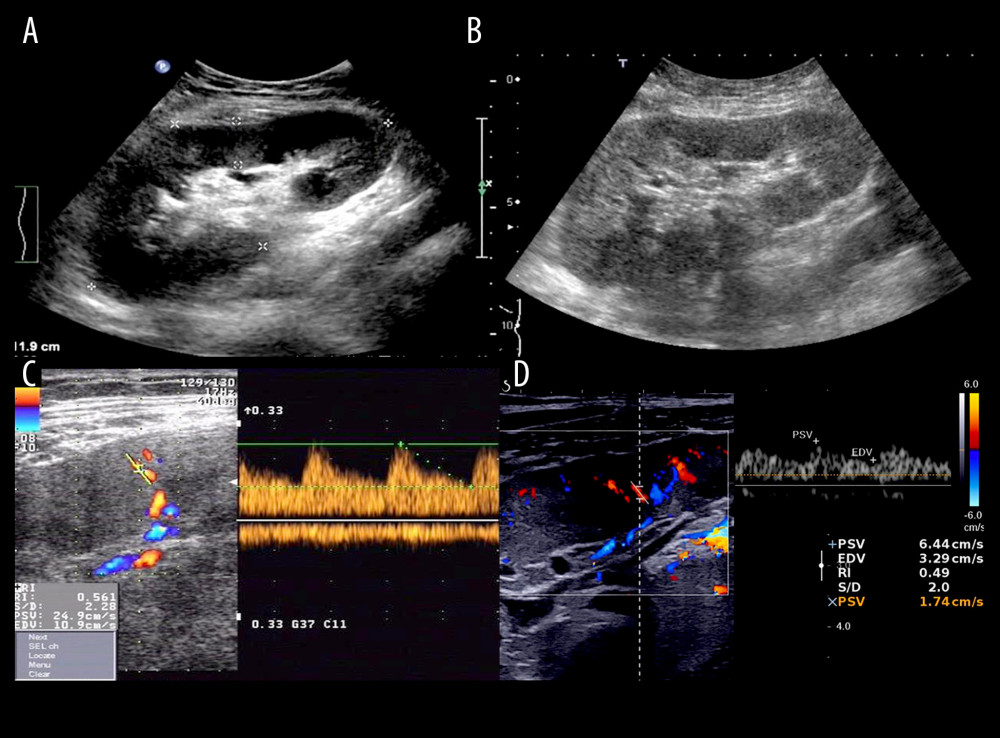 Figure 2. Ultrasonic characteristics of recurrent IgAN: ultrasound showed equal echo of the renal parenchyma in mild injury (Lee’s II) (A) by contrast with echo enhancement in severe injury (Lee’s IV) (B); hemodynamics showed markedly decreasing EDV of the SRA in severe injury (Lee’s IV) (D) proceeded from mild injury (Lee’s II) (C) (Photoshop, 21.1, Adobe).
Figure 2. Ultrasonic characteristics of recurrent IgAN: ultrasound showed equal echo of the renal parenchyma in mild injury (Lee’s II) (A) by contrast with echo enhancement in severe injury (Lee’s IV) (B); hemodynamics showed markedly decreasing EDV of the SRA in severe injury (Lee’s IV) (D) proceeded from mild injury (Lee’s II) (C) (Photoshop, 21.1, Adobe). 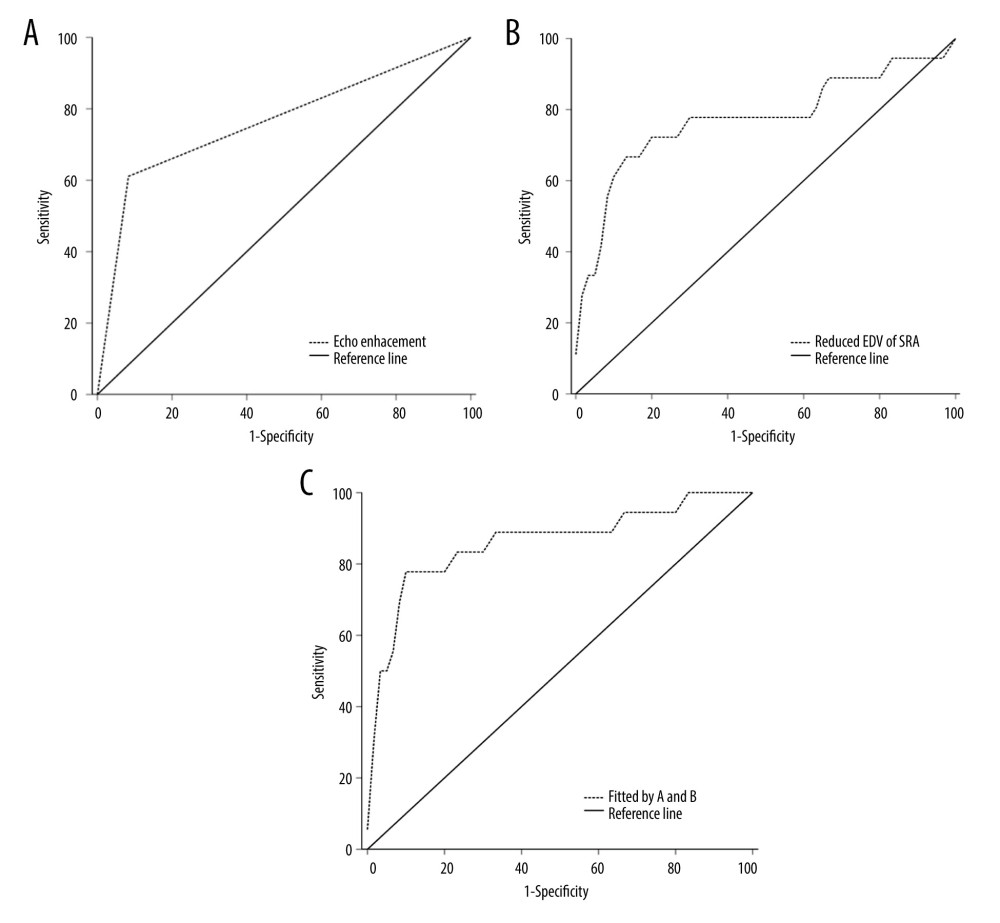 Figure 3. ROC curves: echo enhancement (A), decreasing EDV of the ARA (B) and fitted by the above two (C) (SPSS Statistics, 22.0, IBM).
Figure 3. ROC curves: echo enhancement (A), decreasing EDV of the ARA (B) and fitted by the above two (C) (SPSS Statistics, 22.0, IBM). Tables
Table 1. Baseline characteristics of the recipients and donors.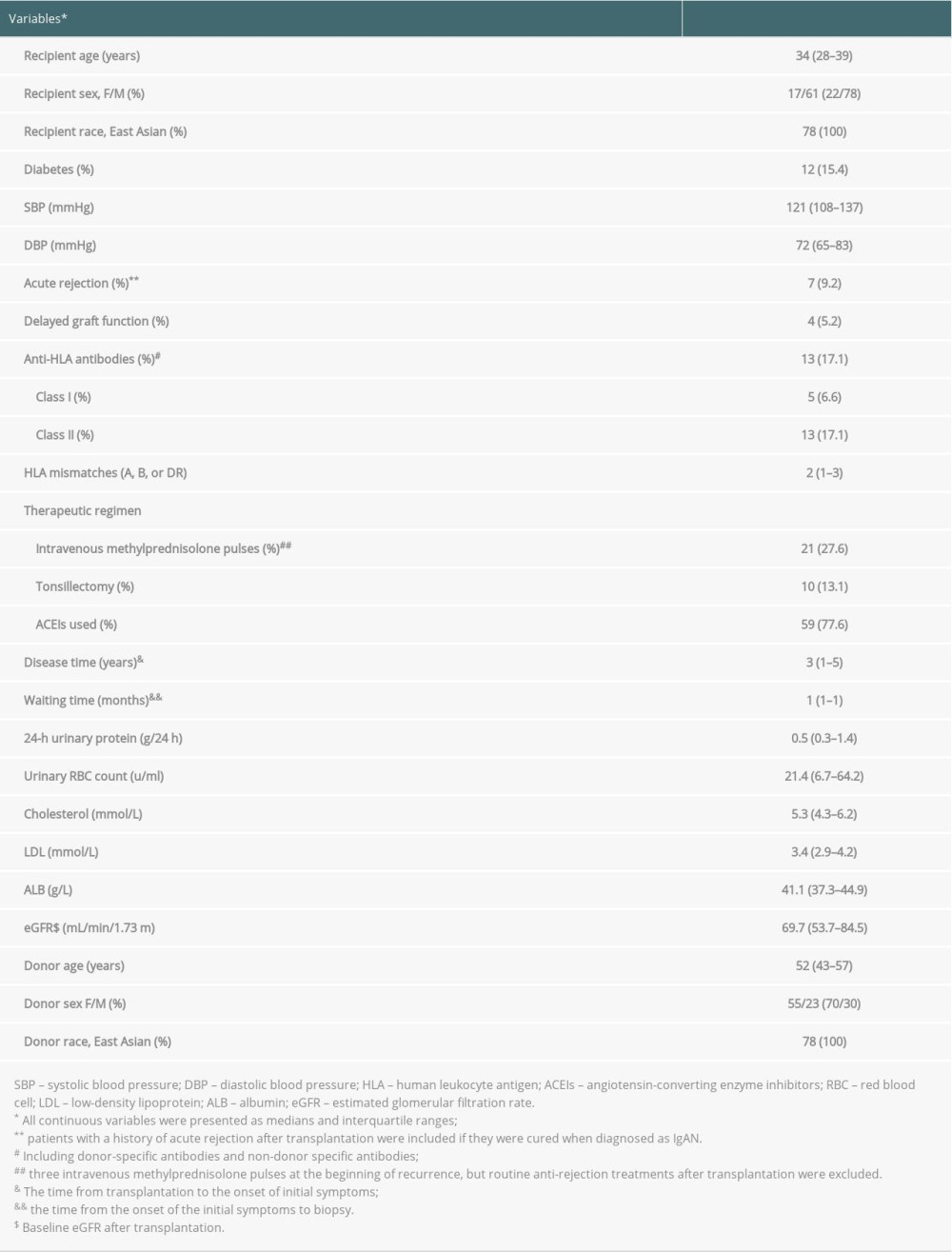 Table 2. The 4-year graft cumulative survival rate after biopsy diagnosis of Lee’s classification and histopathological injury.
Table 2. The 4-year graft cumulative survival rate after biopsy diagnosis of Lee’s classification and histopathological injury. Table 3. Color Doppler ultrasonic and hemodynamic indexes (based on Lee’s classification).
Table 3. Color Doppler ultrasonic and hemodynamic indexes (based on Lee’s classification).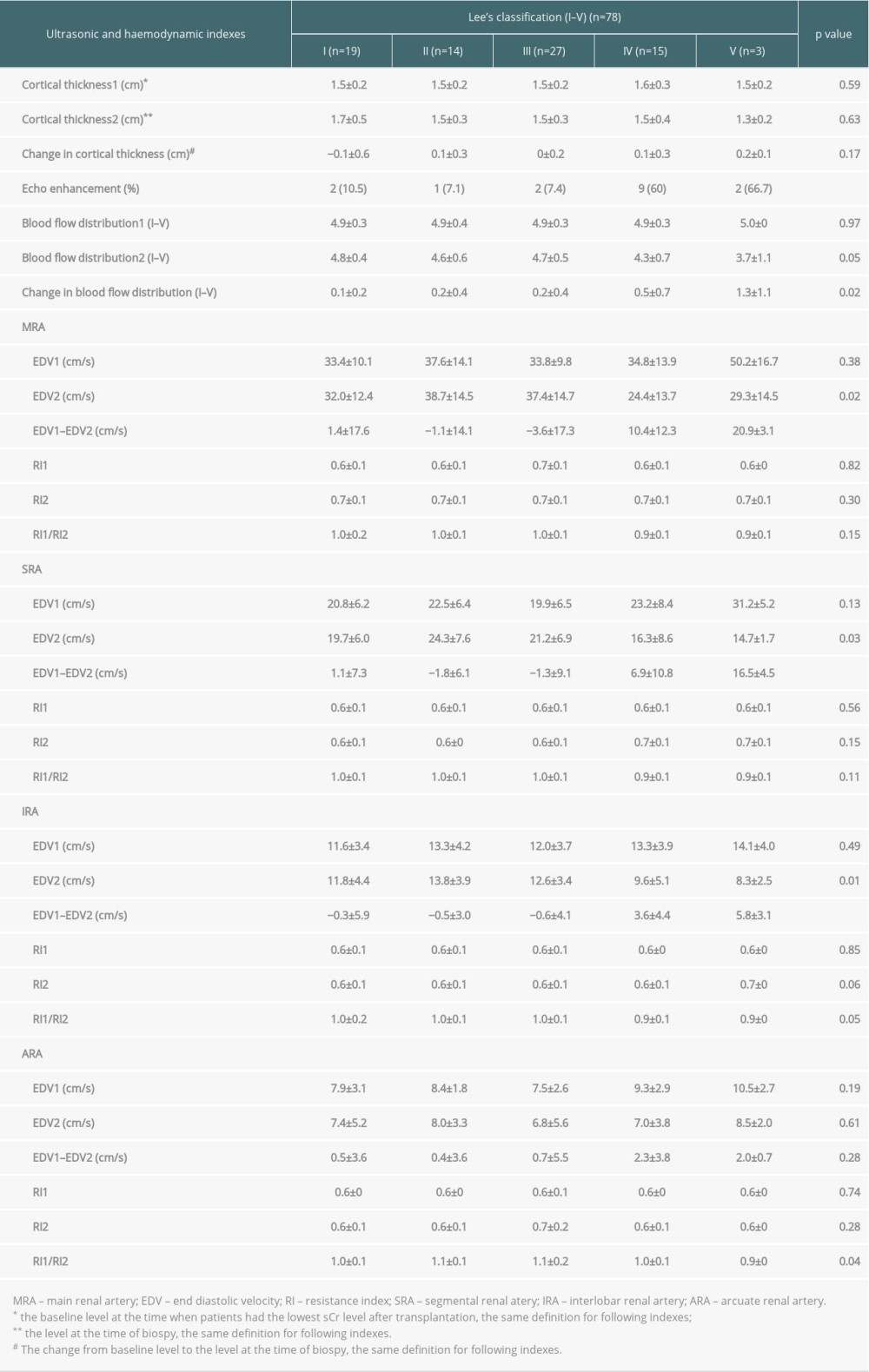 Table 4. Predictive factors related to histopathological injury in recurrent IgAN.
Table 4. Predictive factors related to histopathological injury in recurrent IgAN.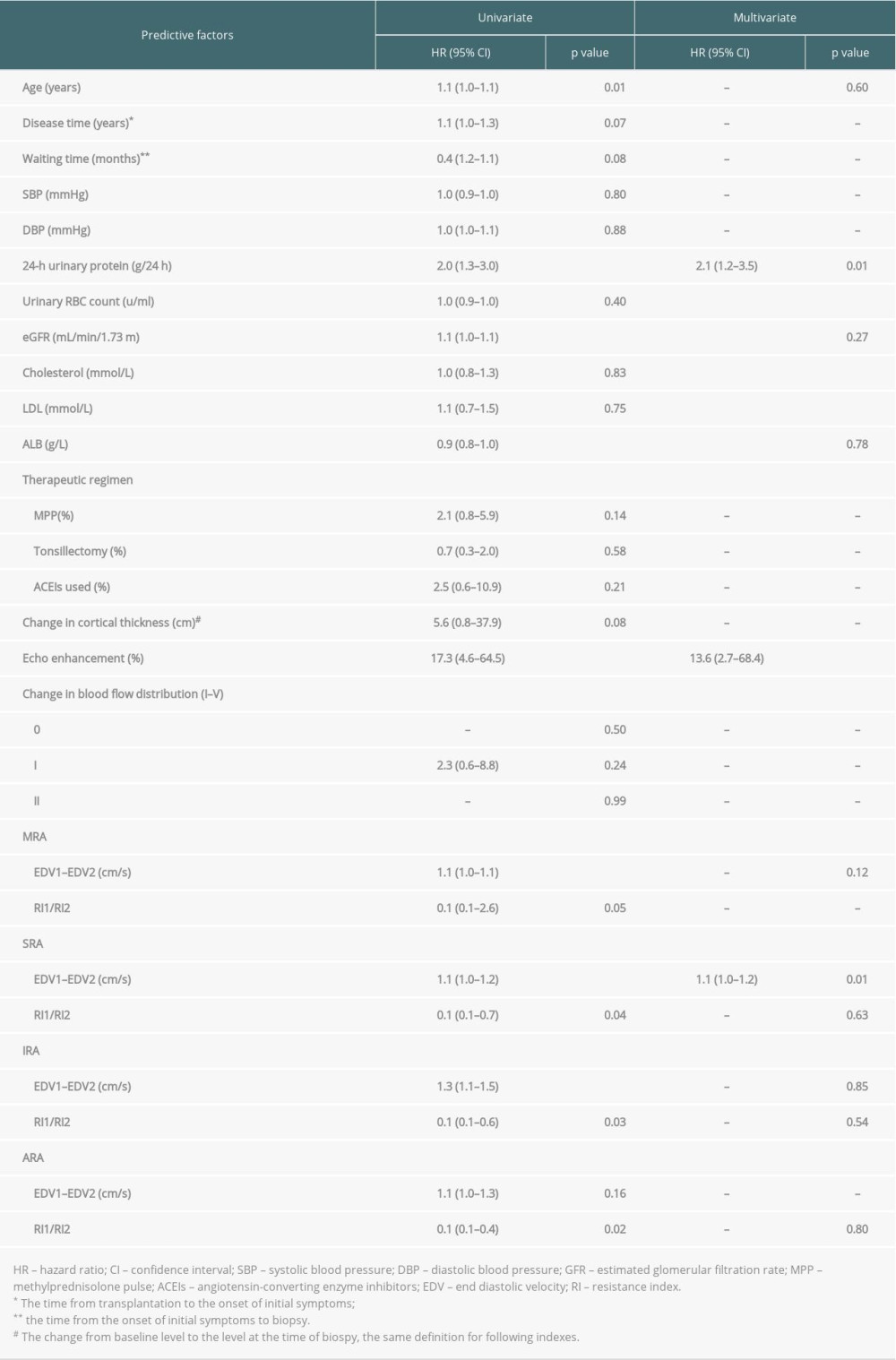 Table 5. Ultrasonic indexes in predicting of severe histopathological injury in recurrent IgAN.
Table 5. Ultrasonic indexes in predicting of severe histopathological injury in recurrent IgAN.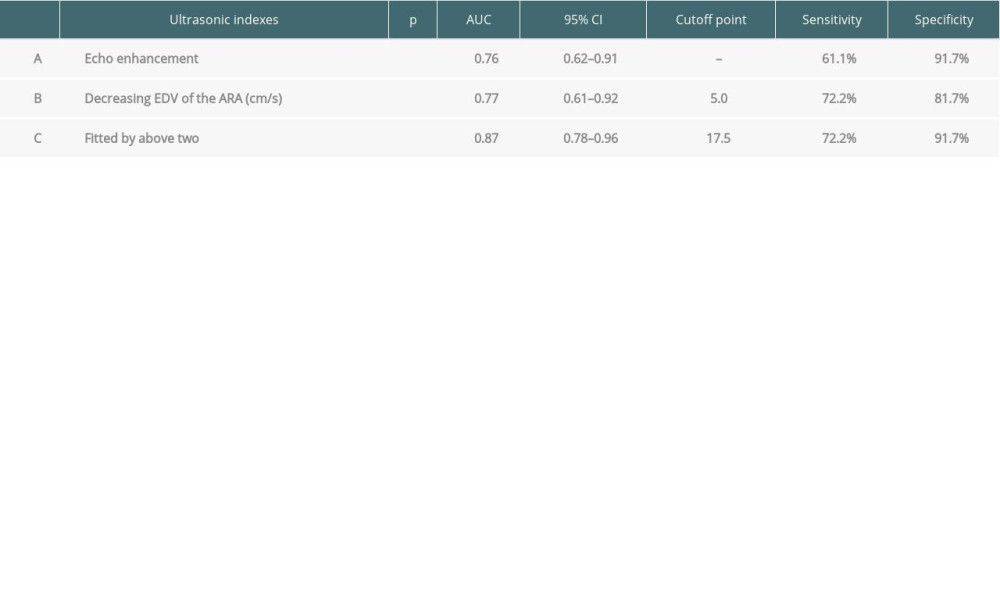
References
1. Briganti EM, Russ GR, McNeil JJ, Risk of renal allograft loss from recurrent glomerulonephritis: N Engl J Med, 2002; 347; 103-9
2. Ponticelli C, Glassock RJ, Posttransplant recurrence of primary glomerulonephritis: Clin J Am Soc Nephrol, 2010; 5; 2363-72
3. Zhang J, Qiu J, Chen GD, Etiological analysis of graft dysfunction following living kidney transplantation: A report of 366 biopsies: Ren Fail, 2018; 40; 219-25
4. Di Vico MC, Messina M, Recurrent IgA nephropathy after renal transplantation and steroid withdrawal: Clin Transplant, 2018; 32; e13207
5. Floege J, Gröne HJ, Recurrent IgA nephropathy in the renal allograft: Not a benign condition: Nephrol Dial Transplant, 2013; 28; 1070-73
6. Schwarz A, Gwinner W, Hiss M, Safety and adequacy of renal transplant protocol biopsies: Am J Transplant, 2005; 5; 1992-96
7. Abe M, Akaishi T, Miki T, Influence of renal function and demographic data on intrarenal Doppler ultrasonography: PLoS One, 2019; 14; e0221244
8. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerulonephritis Work Group, KDIGO clinical practice guideline for glomerulonephritis: Kidney Int Suppl, 2012; 2; 139-274
9. Lee SM, Rao VM, Franklin WA, IgA nephropathy: Morphologic predictors of progressive renal disease: Hum Pathol, 1982; 13; 314-22
10. Hanssen O, Erpicum P, Lovinfosse P: Clin Kidney J, 2017; 10; 97-105
11. Sharma AK, Rustom R, Evans A, Utility of serial Doppler ultrasound scans for the diagnosis of acute rejection in renal allografts: Transpl Int, 2004; 17; 138-44
12. Merkus JW, Hoitsma AJ, van Asten WN, Doppler spectrum analysis to diagnose rejection during posttransplant acute renal failure: Transplantation, 1994; 58; 570-76
13. Dugo M, Mangino M, Meola M, Ultrasound findings of BK polyomavirus-associated nephropathy in renal transplant patients: J Nephrol, 2017; 30; 449-53
14. Cano H, Castañeda DA, Patiño N, Resistance index measured by Doppler ultrasound as a predictor of graft function after kidney transplantation: Transplant Proc, 2014; 46; 2972-74
15. Elec FI, Elec AD, Bolboaca S, Contrast-enhanced ultrasonography in the initial evaluation of the kidney graft function: A pilot study: Med Ultrason, 2020; 22; 1-7
16. Bolboac , Elec , Muntean , Shear-wave elastography variability analysis and relation with kidney allograft dysfunction: A single-center study: Diagnostics, 2020; 10; 41
17. Nijim S, Vujjini V, Alasfar S, Recurrent IgA nephropathy after kidney transplantation: Transplant Proc, 2016; 48; 2689-94
18. Berger J, Recurrence of IgA nephropathy in renal allografts: Am J Kidney Dis, 1988; 12; 371-72
19. Zhang J, Chen GD, Qiu J, Graft failure of IgA nephropathy in renal allografts following living donor transplantation: Predictive factor analysis of 102 biopsies: BMC Nephrol, 2019; 20; 446
20. Cabral DB, De Sandes-Freitas TV, Medina-Pestana JO, Clinical features, treatment and prognostic factors of post-transplant Immunoglobulin A nephropathy: Ann Transpl, 2018; 23; 166-75
21. Ortiz F, Gelpi R, Koskinen P, IgA nephropathy recurs early in the graft when assessed by protocol biopsy: Nephrol Dial Transplant, 2012; 27; 2553-58
22. Mostbeck GH, Kain R, Mallek R, Duplex Doppler sonography in renal parenchymal disease. Histopathologic correlation: J Ultrasound Med, 1991; 10; 189-94
23. Li L, Wang ZG, Jing XX, Experimental study on video frequency method of UTC control targeted contrast imaging of renal ischemia-reperfusion: Chin J Med Imaging Technol, 2006; 22; 650-52
24. Tuma J, Novakova B, Schwarzenbach HR, Image analysis in the differential diagnosis of renal parenchyma lesions: Ultraschall Med, 2011; 32; 286-92
25. Platt JF, Rubin JM, Ellis JH, Distinction between obstructive and nonobstructive pyelocaliectasis with duplex Doppler sonography: Am J Roentgenol, 1989; 153; 997-1000
26. Kolonko A, Chudek J, Zejda JE, Wiecek A, Impact of early kidney resistance index on kidney graft and patient survival during a 5-year follow-up: Nephrol Dial Transplant, 2012; 27; 1225-31
27. Maarten , Naesens , Line , Intrarenal resistive index after renal transplantation: N Engl J Med, 2013; 369; 1797-806
Figures
Figure 1. Kaplan-Meier curves of Lee’s classification (A) and histopathological injury (B) (SPSS Statistics, 22.0, IBM).Figure 2. Ultrasonic characteristics of recurrent IgAN: ultrasound showed equal echo of the renal parenchyma in mild injury (Lee’s II) (A) by contrast with echo enhancement in severe injury (Lee’s IV) (B); hemodynamics showed markedly decreasing EDV of the SRA in severe injury (Lee’s IV) (D) proceeded from mild injury (Lee’s II) (C) (Photoshop, 21.1, Adobe).Figure 3. ROC curves: echo enhancement (A), decreasing EDV of the ARA (B) and fitted by the above two (C) (SPSS Statistics, 22.0, IBM). Tables
Table 1. Baseline characteristics of the recipients and donors.Table 2. The 4-year graft cumulative survival rate after biopsy diagnosis of Lee’s classification and histopathological injury.Table 3. Color Doppler ultrasonic and hemodynamic indexes (based on Lee’s classification).Table 4. Predictive factors related to histopathological injury in recurrent IgAN.Table 5. Ultrasonic indexes in predicting of severe histopathological injury in recurrent IgAN.Table 1. Baseline characteristics of the recipients and donors.Table 2. The 4-year graft cumulative survival rate after biopsy diagnosis of Lee’s classification and histopathological injury.Table 3. Color Doppler ultrasonic and hemodynamic indexes (based on Lee’s classification).Table 4. Predictive factors related to histopathological injury in recurrent IgAN.Table 5. Ultrasonic indexes in predicting of severe histopathological injury in recurrent IgAN. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988