15 October 2021: Original Paper
Intraoperative Low-Dose Dexmedetomidine Administration Associated with Reduced Hepatic Ischemia-Reperfusion Injury in Pediatric Deceased Liver Transplantation: A Retrospective Cohort Study
Liang Zhang1ABCDEF, Na Li1BEF, Ling-Li Cui1BF, Fu-Shan Xue1ADFG*, Zhi-Jun Zhu234ADFGDOI: 10.12659/AOT.933354
Ann Transplant 2021; 26:e933354






Abstract
BACKGROUND: Dexmedetomidine (DEX) attenuates hepatic ischemia-reperfusion injury (HIRI) in adult liver transplantation (LT), but its effects on postoperative liver graft function in pediatric LT remain unclear. We sought to investigate whether intraoperative DEX administration was associated with improved liver graft function in pediatric LT recipients. It was hypothesized that DEX administration was associated with reduced HIRI and improved liver graft function.
MATERIAL AND METHODS: From November 2015 to May 2020, 54 deceased pediatric LT recipients were categorized into a control group and a DEX group. Intraoperatively, the DEX group received an additional infusion of DEX at 0.4 µg/kg/h from incision to the end of the operation in comparison with the control group. Preoperative, intraoperative, and postoperative data were reviewed. Postoperative liver enzyme levels and HIRI severity were assessed and compared. Independent risk factors for HIRI were determined by multivariate logistic regression analysis using a stepwise forward conditional method.
RESULTS: We enrolled 28 and 26 patients in the DEX and control groups, respectively. Patients in the DEX group exhibited a reduced incidence of moderate-to-severe HIRI (88.5% vs 60.7%, P=0.020) and decreased level of serum alanine aminotransferase (median [interquartile range]: 407 [230-826] vs 714 [527-1492] IU/L, P=0.048) compared with the controls. Binary logistic analysis revealed that longer cold ischemia time (odds ratio [OR]=1.006; 95% confidence interval [CI]=1.000-1.013; P=0.044) and intraoperative DEX use (OR=0.198; 95% CI=0.045-0.878; P=0.033) were independent predictors for moderate-to-severe HIRI.
CONCLUSIONS: Intraoperative low-dose DEX administration was associated with a lower incidence of moderate-to-severe HIRI in pediatric deceased LT. However, further studies are needed to confirm our results and elucidate the underlying mechanisms.
Keywords: Dexmedetomidine, Liver Transplantation, Pediatrics, Child, Humans, Liver
Background
Hepatic ischemia-reperfusion injury (HIRI), an inevitable event during liver transplantation (LT), may further trigger early allograft dysfunction or even primary nonfunction [1,2]. Previous studies have found that attenuating HIRI could improve post-LT liver graft function [3,4]. Although numerous strategies to mitigate HIRI have been assessed in animal models [5], current therapeutic opinions are still limited in clinical practice.
Dexmedetomidine (DEX) is a selective alpha-2-adrenoceptor agonist with sedative, analgesic, sympatholytic, and anti-inflammatory properties, widely introduced to pediatric practice [6]. Previous animal experiments have demonstrated that DEX can protect against HIRI in conditions of partial hepatectomy [7,8]. A recent observational study revealed that DEX alleviates HIRI in adult living-donor LT [9]. However, few studies have focused on the association between intraoperative DEX administration and the severity of HIRI in the setting of pediatric LT. Therefore, we hypothesized that intraoperative DEX use is associated with better liver graft function in pediatric deceased LT.
In this retrospective cohort study, we sought to explore the effects of intraoperative low-dose DEX administration on the severity of HIRI and postoperative liver graft function in pediatric deceased LT.
Material and Methods
STUDY SUBJECTS:
This retrospective cohort study was performed at Beijing Friendship Hospital, which is one of the 3 largest pediatric LT centers in China. We included all pediatric patients of ages 16 years or younger who were consecutively scheduled to undergo deceased LT under anesthesia care by Dr. Liang Zhang from November 2015 to May 2020. Patients who underwent retransplantation, received anesthesia care from other anesthesiologists, or did not have complete data were excluded. The study protocol was conducted in accordance with the Declaration of Helsinki guidelines and its later amendments. Ethics approval (2020-P2-043-02) was provided by the Institutional Review Board of Beijing Friendship Hospital. Given the retrospective nature of this study, the requirement for patient consent was waived, and Dr. Liang Zhang was not blinded to the study protocol; however, data collectors were blinded, and whether a specific patient had been given DEX or not was also blinded to Dr. Liang Zhang.
ANESTHESIA PROTOCOL:
All the patients receiving the basic anesthesia protocol from our institution were described previously [10]. However, it was not until 2017 that the anesthetist-in-charge began to more liberally choose to administer DEX as an anesthetic adjuvant. As a result, patients were divided into one of the following 2 groups: the control group (standardized anesthesia protocol without intraoperative DEX) or the DEX group (standardized anesthesia protocol with intraoperative DEX administration). In the DEX group, DEX was administered by continuous infusion at 0.4 μg/kg/h without a loading dose from incision to the end of the operation to exert anti-inflammatory and sympatholytic effects.
SURGICAL TECHNIQUE:
For surgical procedures, a whole liver graft was anastomosed using the conventional technique, whereas a split or reduced-size liver graft was anastomosed following the modified piggy-back technique. During the anhepatic phase, the inferior vena cava was completely clamped in all cases without veno-venous bypass or temporary portocaval shunt.
OUTCOMES MEASURES:
The primary endpoints were the peak alanine aminotransferase (ALT), aspartate aminotransferase (AST), and lactic dehydrogenase (LDH) levels during the first week after LT and the severity of HIRI, which was assessed by Rahman’s criteria [11] based on the peak AST level within 24 h after LT (Mild HIRI, AST <1000 U/L; Moderate HIRI, AST 1000–5000 U/L; and Severe HIRI, AST >5000 U/L). Secondary outcomes included the peak blood urea nitrogen (BUN) and serum creatinine (Cr) levels during the first week after LT, the incidence of the severe postreperfusion syndrome (PRS) and acute kidney injury (AKI), and the durations of mechanical ventilation, intensive care unit (ICU) stay, and hospital stay. The extent of severe PRS and AKI were evaluated using the Peking criteria [10] and the Kidney Disease: Improving Global Outcomes (KDIGO) criteria [12].
STATISTICAL ANALYSIS:
Continuous variables are presented as the mean±standard deviation or median (interquartile range) and were compared using the
Results
BASELINE CHARACTERISTICS OF THE STUDY POPULATION:
A total of 54 patients who underwent pediatric deceased LT met the inclusion criteria (Figure 1). The patients were divided into 2 groups: the control group (n=26) and the DEX group (n=28). The median age of the entire cohort was 3.0 years (37.0% females), with biliary atresia (61.1%) as the most common indication. The basic characteristics of the 2 groups are listed in Table 1. No statistically significant differences were noted between the control and DEX groups with regard to age, sex, height, weight, graft type, graft weight, graft-to-recipient weight ratio, cold ischemia time (CIT), and the indication for LT (all P>0.05). However, the warm ischemia time (WIT) duration was significantly longer in the control group than in the DEX group (52±13 vs 43±10 min, P=0.004).
LIVER GRAFT FUNCTION ASSESSMENT AND OTHER CLINICAL OUTCOMES:
Postoperative peak serum ALT levels during the first week decreased significantly in the DEX group compared with the control group (median: 407 vs 714 IU/L, P=0.048). The peak AST and LDH levels in the DEX group were also reduced compared with the control group, but the differences were not statistically significant (median: 1378 vs 1735 IU/L, P=0.107; and median: 1677 vs 2350 IU/L, P=0.106, respectively). However, cohort analysis revealed that moderate-to-severe HIRI occurred less frequently in the DEX group than in controls (60.7% vs 88.5%, P=0.020) (Figure 2). The postoperative peak BUN and Cr levels within 7 days after LT were comparable between the DEX and control groups (median: 6.13 vs 5.33 mmol/L, P=0.082; and median: 35.6 vs 37.0 μmol/L, P=0.177, respectively). Furthermore, no statistically significant differences were identified between the 2 groups with respect to the occurrence of severe PRS and AKI, epinephrine requirement for severe PRS, and durations of mechanical ventilation, ICU stay, and hospital stay (all P>0.05) (Table 2).
ASSOCIATION BETWEEN DEXMEDETOMIDINE USE AND MODERATE-TO-SEVERE HIRI:
Univariate analyses revealed the potential risk factors associated with moderate-to-severe HIRI, including height (odds ratio [OR]=0.978; 95% confidence interval [CI]=0.952–1.004; P=0.097), Child score (OR=1.380; 95% CI=1.001–1.901; P=0.049), CIT (OR=1.006; 95% CI=1.000–1.013; P=0.035), and intraoperative DEX use (OR=0.202; 95% CI=0.049–0.836; P=0.027). Multivariate logistic analysis revealed that intraoperative DEX use (OR=0.198; 95% CI=0.045–0.878; P=0.033) and CIT (OR=1.006; 95% CI=1.000–1.013; P=0.044) were independent predictors of moderate-to-severe HIRI (Table 3). The multiple regression coefficient of determination was 0.255.
Discussion
This retrospective study demonstrates that intraoperative use of DEX was significantly associated with improved post-LT liver graft function following pediatric deceased LT. Patients who received low-dose DEX treatment exhibit significantly deceased postoperative peak levels of serum ALT and a reduced incidence of moderate-to-severe HIRI. To the best of our knowledge, this study is the first to assess the hepatoprotective effect of DEX in pediatric deceased LT. Finally, our results confirm that DEX exerts protective effects against HIRI in pediatric deceased LT recipients.
As one of the critical challenges during LT, HIRI is strongly associated with increased morbidity and mortality in the post-LT period [5,13]. Generally, the severity of HIRI during LT is assessed by postoperative peak serum transaminase levels [11,14,15]. Despite being the subject of intense study and development efforts over the past 2 decades, current effective therapeutic opinions for HIRI in LT are limited in clinical practice. Currently, pharmacological agents to attenuate HIRI in the setting of clinical LT include N-acetylcysteine [16,17], nitric oxide [18], rifaximin [19], L-alanyl-glutamine [20], prostaglandin E1 [21], and omega-3 fatty acids [22]. However, none of these agents have been shown to reduce HIRI-associated morbidity and mortality in clinical studies.
DEX, an alpha-2-adrenergic agonist with sedative, anxiolytic, sympatholytic, and analgesic properties, has been increasingly used in both pediatric clinical trials and routine clinical practice. Animal experiments and clinical studies have revealed that DEX has protective effects against heart [23], lung [24], brain [25], and kidney [26] ischemia-reperfusion injuries. In accordance with our present findings, previous studies demonstrated the hepatoprotective effect of DEX in hepatectomy and LT. In the setting of hepatectomy, Zhang et al [27] and Wang et al [28] indicated that pre-pump administration of DEX exerted a protective effect against HIRI in their randomized controlled trials, while Fayed and colleagues [9] reported that an intraoperative infusion of DEX at 0.8 μg/kg/h exerted hepatoprotective effects against HIRI in adult living-donor LT.
The identification of independent predictors associated with moderate-to-severe HIRI could provide insight into postoperative liver graft function recovery. Similar to the present results, CIT was typically the most frequent risk factor for developing delayed graft function following deceased LT [29–31]. The possible reason for the association of CIT and postoperative liver graft function recovery involved cell damage in the cold ischemic phase of HIRI [5]. It has been previously reported that the pathophysiology of HIRI in this ischemic phase is due to oxidative stress damage, lipid metabolism disorders, inflammation response, and intracellular calcium overload [5,13]. Therefore, normothermic machine perfusion focusing on the shortening of CIT in clinical LT had the potential to emerge as one of the most promising approaches to alleviate HIRI in LT using marginal liver grafts [32].
The exact mechanism of the protective effects of DEX against HIRI following LT is still unclear. In animal models of partial hepatectomy and LT, both Wang et al [8] and Lv et al [7] indicated that DEX treatment ameliorated HIRI via suppression of the TLR4/NF-κB pathway. In contrast, Chen and colleagues [33] demonstrated that the acceleration of HIRI in NLRC5 knockout mice could be inhibited by DEX pretreatment through NF-κB suppression, Nrf2 promotion, and Caspase-3 suppression. In clinical studies, both Wang et al [27] and Zhang et al [28] attributed the liver and intestinal protection of DEX after hepatectomy to its anti-inflammatory effects. In contrast, Fayed et al [9] emphasized that DEX exerted protective effects against HIRI during adult living-donor LT by suppressing ICAM-1. Given that inflammation is a key process during the reperfusion phase, the hepatoprotective effects of DEX are possibly related to its anti-inflammatory properties.
Evidence regarding the safety of the off-label use of DEX in children [6] and LT recipients [34,35] remains limited. Potential adverse effects include bradycardia, hypertension, hypotension, elevated blood glucose, decreased serum potassium concentration, interaction with tacrolimus, and drug accumulation [6,35–37]. Although there were concerns of potential risks of delayed awakening and extubation due to the accumulation of DEX in patients with impaired liver function, no studies [9,38], including ours, have demonstrated any increase in the durations of mechanical ventilation, ICU stay, and hospital stay. This could be because the infusion rate and total dose of DEX in our study were lower than those of previous reports [9,27,28,35,38,39]. We used a dose of 0.4 μg/kg/h for approximately 8 h without a loading dose, and DEX infusion was well tolerated by the patients, without noticeable adverse effects attributable to the infusion. Whether a higher dose of DEX infusion could exert a better hepatoprotective effect or delay the awakening and extubation following pediatric LT remains a focus of future research.
The present study has several limitations. First, this was a retrospective study with a relatively small sample size; thus, a potential inherent difference in WIT existed between the 2 groups, making the study prone to possible selection bias. Second, the generalizability of the results is subject to the fact that all the participants were from a single institution and were treated by the same surgical and anesthesia team. Third, we did not note any serious adverse drug reactions due to DEX administration. Nevertheless, further studies are needed to assess the potential adverse effects of DEX in the pediatric population. Finally, the dose-dependent effects of DEX on HIRI and the underlying mechanisms should be elucidated in future studies.
Conclusions
Our study revealed 2 independent predictors of moderate-to-severe HIRI in pediatric deceased LT: the duration of CIT and intraoperative use of DEX. Moreover, intraoperative low-dose DEX administration exerted a protective effect against HIRI. Further studies are needed to further elucidate the underlying mechanisms.
Figures
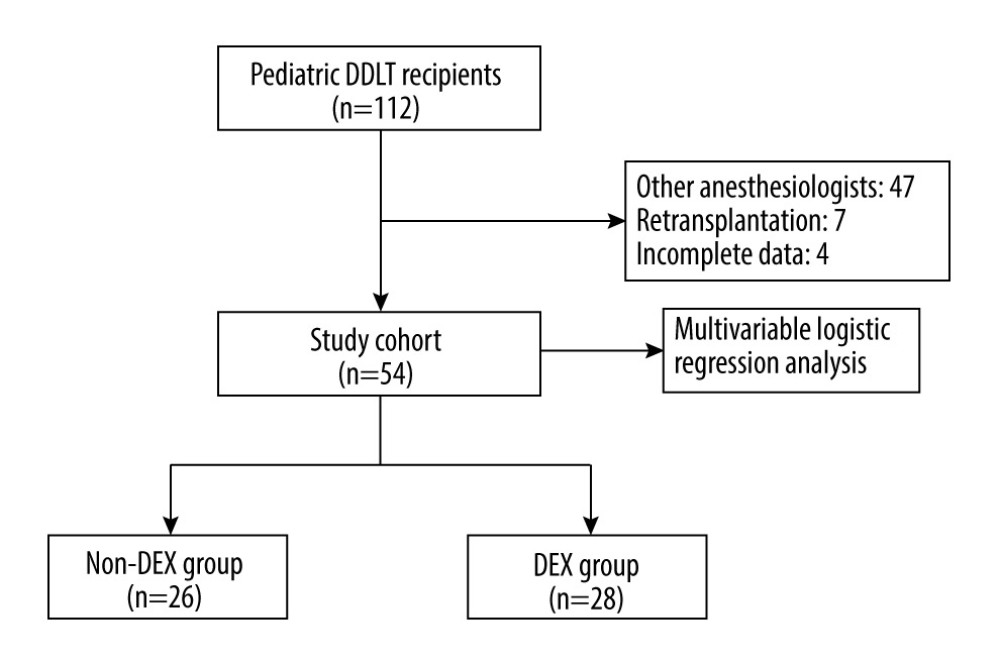 Figure 1. Patient and analysis flowchart. DEX – dexmedetomidine; DDLT – deceased donor liver transplantation. Adobe Photoshop CS6 (Adobe Systems Software Ireland, Ltd.).
Figure 1. Patient and analysis flowchart. DEX – dexmedetomidine; DDLT – deceased donor liver transplantation. Adobe Photoshop CS6 (Adobe Systems Software Ireland, Ltd.). 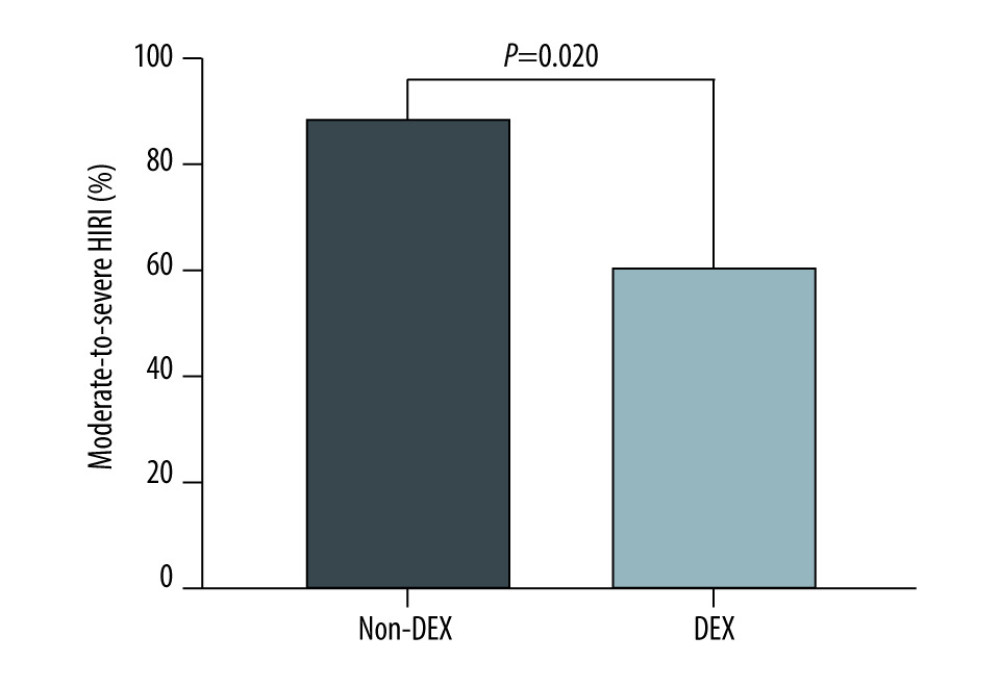 Figure 2. Intraoperative use of dexmedetomidine is associated with a reduced incidence of moderate-to-severe hepatic ischemia-reperfusion injury in pediatric deceased liver transplantation. DEX – dexmedetomidine; HIRI – hepatic ischemia-reperfusion injury. GraphPad Prism 5 (GraphPad Software, Inc., San Diego, CA, USA).
Figure 2. Intraoperative use of dexmedetomidine is associated with a reduced incidence of moderate-to-severe hepatic ischemia-reperfusion injury in pediatric deceased liver transplantation. DEX – dexmedetomidine; HIRI – hepatic ischemia-reperfusion injury. GraphPad Prism 5 (GraphPad Software, Inc., San Diego, CA, USA). References
1. Friedman BH, Wolf JH, Wang L, Serum cytokine profiles associated with early allograft dysfunction in patients undergoing liver transplantation: Liver Transpl, 2012; 18(2); 166-76
2. Neves DB, Rusi MB, Diaz LG, Primary graft dysfunction of the liver: Definitions, diagnostic criteria and risk factors: Einstein (Sao Paulo), 2016; 14(4); 567-72
3. Nickkholgh A, Maluf D, Emerging graft protective strategies in clinical liver transplantation: Expert Rev Gastroenterol Hepatol, 2017; 11(7); 623-31
4. Zhai Y, Petrowsky H, Hong JC, Ischaemia-reperfusion injury in liver transplantation – from bench to bedside: Nat Rev Gastroenterol Hepatol, 2013; 10(2); 79-89
5. Rampes S, Ma D, Hepatic ischemia-reperfusion injury in liver transplant setting: Mechanisms and protective strategies: J Biomed Res, 2019; 33(4); 221-34
6. Sottas CE, Anderson BJ, Dexmedetomidine: The new all-in-one drug in paediatric anaesthesia?: Curr Opin Anaesthesiol, 2017; 30(4); 441-51
7. Lv M, Zeng H, He Y, Dexmedetomidine promotes liver regeneration in mice after 70% partial hepatectomy by suppressing NLRP3 inflammasome not TLR4/NFκB: Int Immunopharmacol, 2018; 54; 46-51
8. Wang Y, Wu S, Yu X, Dexmedetomidine protects rat liver against ischemia-reperfusion injury partly by the α2A-adrenoceptor subtype and the mechanism is associated with the TLR4/NF-κB pathway: Int J Mol Sci, 2016; 17(7); 995
9. Fayed NA, Sayed EI, Saleh SM, Effect of dexmedetomidine on hepatic ischemia-reperfusion injury in the setting of adult living donor liver transplantation: Clin Transplant, 2016; 30(4); 470-82
10. Zhang L, Tian M, Xue F, Diagnosis, incidence, predictors and management of postreperfusion syndrome in pediatric deceased donor liver transplantation: A single-center study: Ann Transplant, 2018; 23; 334-44
11. Rahman S, Davidson BR, Mallett SV, Early acute kidney injury after liver transplantation: Predisposing factors and clinical implications: World J Hepatol, 2017; 9(18); 823-32
12. KDIGO AKI Work Group, KDIGO clinical practice guideline for acute kidney injury: Kidney Int Suppl, 2012; 17; 1-138
13. Jiménez-Castro MB, Cornide-Petronio ME, Gracia-Sancho J, Inflammasome-mediated inflammation in liver ischemia-reperfusion injury: Cells, 2019; 8(10); 1131
14. Rosen HR, Martin P, Goss J, Significance of early aminotransferase elevation after liver transplantation: Transplantation, 1998; 65(1); 68-72
15. Tokodai K, Lannsjö C, Kjaernet F, Association of post-reperfusion syndrome and ischemia reperfusion injury with acute kidney injury after liver transplantation: Acta Anaesthesiol Scand, 2020; 64(6); 742-50
16. Thies JC, Teklote J, Clauer U, The efficacy of N-acetylcysteine as a hepatoprotective agent in liver transplantation: Transpl Int, 1998; 11(Suppl 1); S390-92
17. Hilmi IA, Peng Z, Planinsic RM, N-acetylcysteine does not prevent hepatorenal ischaemia-reperfusion injury in patients undergoing orthotopic liver transplantation: Nephrol Dial Transplant, 2010; 25(7); 2328-33
18. Fukazawa K, Lang JD, Role of nitric oxide in liver transplantation: Should it be routinely used?: World J Hepatol, 2016; 8(34); 1489-96
19. Ito T, Nakamura K, Kageyama S, Impact of rifaximin therapy on ischemia/reperfusion injury in liver transplantation: A propensity score-matched analysis: Liver Transpl, 2019; 25(12); 1778-89
20. Barros MA, Vasconcelos PR, Souza CM, L-alanyl-glutamine attenuates oxidative stress in liver transplantation patients: Transplant Proc, 2015; 47(8); 2478-82
21. Bharathan VK, Chandran B, Gopalakrishnan U, Perioperative prostaglandin e1 infusion in living donor liver transplantation: A double-blind, placebo-controlled randomized trial: Liver Transpl, 2016; 22(8); 1067-74
22. Zhu XH, Wu YF, Qiu YD, Liver-protecting effects of omega-3 fish oil lipid emulsion in liver transplantation: World J Gastroenterol, 2012; 18(42); 6141-47
23. Gong Z, Ma L, Zhong YL, Myocardial protective effects of dexmedetomidine in patients undergoing cardiac surgery: A meta-analysis and systematic review: Exp Ther Med, 2017; 13(5); 2355-61
24. Jiang L, Li L, Shen J, Effect of dexmedetomidine on lung ischemia-reperfusion injury: Mol Med Rep, 2014; 9(2); 419-26
25. Jiang L, Hu M, Lu Y, The protective effects of dexmedetomidine on ischemic brain injury: A meta-analysis: J Clin Anesth, 2017; 40; 25-32
26. Bellos I, Iliopoulos DC, Perrea DN, Pharmacological interventions for the prevention of acute kidney injury after pediatric cardiac surgery: A network meta-analysis: Clin Exp Nephrol, 2019; 23(6); 782-91
27. Wang ZX, Huang CY, Hua YP, Dexmedetomidine reduces intestinal and hepatic injury after hepatectomy with inflow occlusion under general anaesthesia: A randomized controlled trial: Br J Anaesth, 2014; 112(6); 1055-64
28. Zhang Y, Liu M, Yang Y, Dexmedetomidine exerts a protective effect on ischemia-reperfusion injury after hepatectomy: A prospective, randomized, controlled study: J Clin Anesth, 2020; 61; 109631
29. Ito T, Naini BV, Markovic D, Ischemia reperfusion injury and its relationship with early allograft dysfunction in liver transplant patients: Am J Transplant, 2021; 21(2); 614-25
30. Bastos-Neves D, Salvalaggio PRO, Almeida MD, Risk factors, surgical complications and graft survival in liver transplant recipients with early allograft dysfunction: Hepatobiliary Pancreat Dis Int, 2019; 18(5); 423-29
31. Ali JM, Davies SE, Brais RJ, Analysis of ischemia/reperfusion injury in time-zero biopsies predicts liver allograft outcomes: Liver Transpl, 2015; 21(4); 487-99
32. Nasralla D, Coussios CC, Mergental H, A randomized trial of normothermic preservation in liver transplantation: Nature, 2018; 557(7703); 50-56
33. Chen Z, Ding T, Ma CG, Dexmedetomidine (DEX) protects against hepatic ischemia/reperfusion (I/R) injury by suppressing inflammation and oxidative stress in NLRC5 deficient mice: Biochem Biophys Res Commun, 2017; 493(2); 1143-50
34. Soleimanpour H, Nia KS, Sanaie S, Use of dexmedetomidine in liver disease: A systematic review and meta-analysis: Hepat Mon, 2019; 19(10); e98530
35. Enomoto Y, Kudo T, Saito T, Prolonged use of dexmedetomidine in an infant with respiratory failure following living donor liver transplantation: Paediatr Anaesth, 2006; 16(12); 1285-88
36. Stiehl SR, Squires JE, Bucuvalas JC, Tacrolimus interaction with dexmedetomidine – a case report: Pediatr Transplant, 2016; 20(1); 155-57
37. Damian MA, Hammer GB, Elkomy MH, Pharmacokinetics of dexmedetomidine in infants and children after orthotopic liver transplantation: Anesth Analg, 2020; 130(1); 209-16
38. Lee H, Yang SM, Chung J, Effect of perioperative low-dose dexmedetomidine on postoperative delirium after living-donor liver transplantation: A randomized controlled trial: Transplant Proc, 2020; 52(1); 239-45
39. Ni C, Masters J, Zhu L, Study design of the DAS-OLT trial: A randomized controlled trial to evaluate the impact of dexmedetomidine on early allograft dysfunction following liver transplantation: Trials, 2020; 21(1); 582
Figures
Figure 1. Patient and analysis flowchart. DEX – dexmedetomidine; DDLT – deceased donor liver transplantation. Adobe Photoshop CS6 (Adobe Systems Software Ireland, Ltd.).Figure 2. Intraoperative use of dexmedetomidine is associated with a reduced incidence of moderate-to-severe hepatic ischemia-reperfusion injury in pediatric deceased liver transplantation. DEX – dexmedetomidine; HIRI – hepatic ischemia-reperfusion injury. GraphPad Prism 5 (GraphPad Software, Inc., San Diego, CA, USA). Tables
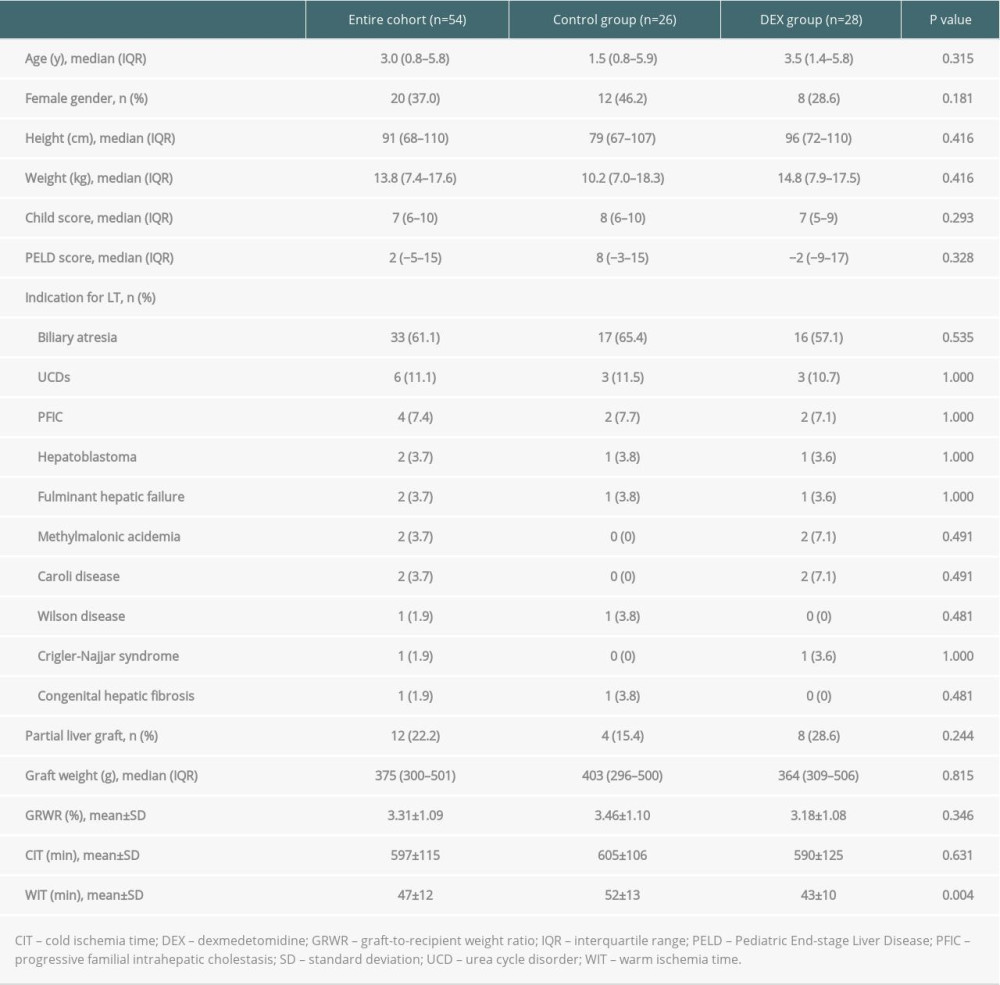 Table 1. Patients’ characteristics.
Table 1. Patients’ characteristics.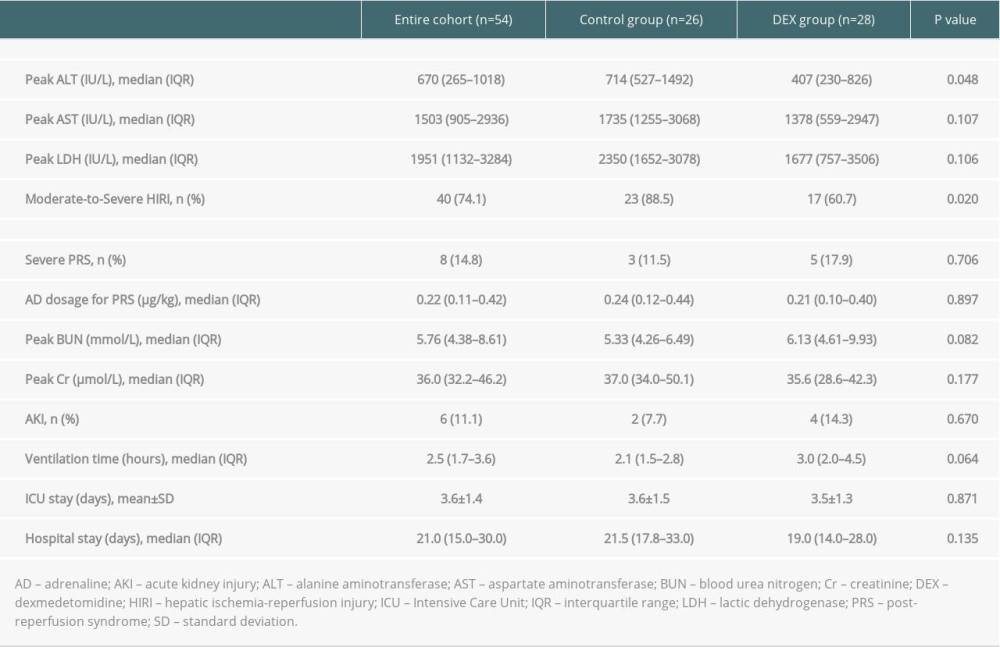 Table 2. Comparison of study outcomes between the control group and the DEX group.
Table 2. Comparison of study outcomes between the control group and the DEX group.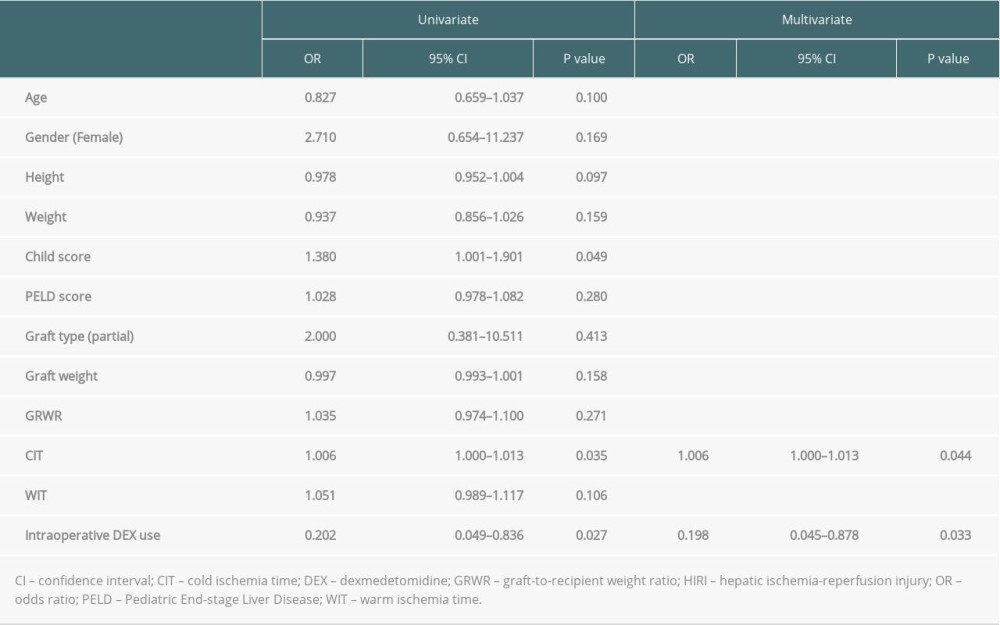 Table 3. Risk factors of moderate-to-severe HIRI in pediatric deceased donor liver transplantation.Table 1. Patients’ characteristics.Table 2. Comparison of study outcomes between the control group and the DEX group.Table 3. Risk factors of moderate-to-severe HIRI in pediatric deceased donor liver transplantation.
Table 3. Risk factors of moderate-to-severe HIRI in pediatric deceased donor liver transplantation.Table 1. Patients’ characteristics.Table 2. Comparison of study outcomes between the control group and the DEX group.Table 3. Risk factors of moderate-to-severe HIRI in pediatric deceased donor liver transplantation. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988