12 March 2024: Original Paper
Use of LCP-Tacrolimus (LCPT) in Kidney Transplantation: A Delphi Consensus Survey of Expert Clinicians
Alexander WisemanDOI: 10.12659/AOT.943498
Ann Transplant 2024; 29:e943498






Abstract
BACKGROUND: LCPT (Envarsus XR®) is a common once-daily, extended-release oral tacrolimus formulation used in kidney transplantation. However, there are minimal evidence-based recommendations regarding optimal dosing and treatment in the de novo and conversion settings.
MATERIAL AND METHODS: Using Delphi methodology, 12 kidney transplantation experts with LCPT experience reviewed available data to determine potential consensus topics. Key statements regarding LCPT use were generated and disseminated to the panel in an online Delphi survey. Statements were either accepted, revised, or rejected based on the level of consensus, perceived strength of evidence, and alignment with clinical practice. Consensus was defined a priori as ≥75% agreement.
RESULTS: Twenty-three statements were generated: 14 focused on de novo LCPT use and 9 on general administration or LCPT conversion use. After 2 rounds, consensus was achieved for 11/14 of the former and 7/9 of the latter statements. In a de novo setting, LCPT was recognized as a first-line option based on its safety and efficacy compared to immediate-release tacrolimus. In particular, African Americans and rapid metabolizer populations were identified as preferred for first-line LCPT therapy. In a conversion setting, full consensus was achieved for converting to LCPT to address neurological adverse effects related to immediate-release tacrolimus and for the time required (approximately 7 days) for steady-state LCPT trough levels to be reached.
CONCLUSIONS: When randomized clinical trials do not replicate current utilization patterns, the Delphi process can successfully generate consensus statements by expert clinicians to inform clinical decision-making for the use of LCPT in kidney transplant recipients.
Keywords: Delphi Technique, Kidney Transplantation, Tacrolimus, Humans, Black or African American, Clinical Decision-Making
Background
Formulations of tacrolimus in combination with other immunosuppressants are used in the overwhelming majority of kidney transplant recipients for the prevention of organ rejection [1,2]. After the initial approval of FK506 (Prograf) for kidney transplantation in 1997, several tacrolimus formulations have been studied and approved for use. Most recently, once-daily preparations of tacrolimus have gained United States (US) Food and Drug Administration (FDA) indications for use, both in the de novo setting and for conversion from twice-daily preparations in clinically stable patients following kidney transplantation [3,4]. Potential advantages of once-daily preparations include lower pill burden, greater adherence, and the potential to modify adverse effect profiles associated with pharmacokinetic differences [5–9].
LCPT (Envarsus XR® tablets [Life-Cycle Pharma Tacrolimus], Veloxis Pharmaceuticals, Cary, North Carolina) is a once-daily formulation used to prevent rejection in both de novo kidney transplant patients and patients converted from immediate-release tacrolimus (IR-Tac) formulations [3]. Unlike IR-Tac formulations such as twice-daily Prograf® capsules (Astellas Pharma, Inc., Tokyo, Japan) and once-daily Astagraf XL® capsules (Astellas Pharma, Inc., Tokyo, Japan), once-daily LCPT has been shown to have a smoother, lower-peak pharmacokinetic profile [10–12]. In addition, LCPT maintains target trough levels and avoids the higher peak levels associated with these other tacrolimus formulations [13]. The efficacy of the LCPT extended-release delivery system [14] has been demonstrated in difficult-to-treat patient types, such as rapid metabolizers [15].
Clinical guidelines in kidney transplantation published by KDIGO (Kidney Disease: Improving Global Outcomes) in 2009 recommend using tacrolimus as the first-line calcineurin inhibitor combined with other immunosuppressants for the initial treatment and long-term maintenance of kidney transplantation patients [16]. These guidelines also include recommendations for immunosuppressive therapy to help reduce the cost of these drugs, monitor immunosuppression, and prevent, detect, and treat non-adherence [16]. However, these KDIGO guidelines have not been updated since newer tacrolimus formulations have become available. While phase III data defined the safety and efficacy of LCPT, these studies were performed during an era in which induction therapy evolved away from nondepleting to depleting antibody therapy [2].
Transplant clinicians lack randomized clinical trial data guiding the real-world use of LCPT, and uncertainty remains on how best to use LCPT in kidney transplantation. For instance, the recommended starting dose for LCPT of 0.14 mg/kg is higher than that of IR-Tac since it was decided prior to the FDA decision to lower the recommended starting dose of IR-Tac, and acceptance of this dose among prescribers is unknown [3,17]. Furthermore, the reason(s) for conversion to LCPT and the ideal candidates for LCPT therapy have not been established.
Given these gaps in published data, and the lack of additional randomized controlled trials to address these unresolved issues, a need exists to reach a clinical consensus on best practices for the use of once-daily LCPT in kidney transplantation in a real-world setting. The objective of this study was to address this need by developing a consensus document on the use of LCPT in kidney transplantation using the Delphi process. The Delphi process is an established structured technique to aid consensual group decision-making by experts based on feedback, in the absence of data from robust clinical studies [18,19]. This consensus document aims to inform decision-making for clinicians considering the use of LCPT, educate clinicians on best practices around the use of LCPT in kidney transplantation, and increase awareness of LCPT.
Material and Methods
DEVELOPMENT OF THE DELPHI PANEL QUESTIONNAIRE:
In January 2022, as part of the unblinded preparation phase of the Delphi panel survey of LCPT use in kidney transplantation (Figure 1), panelists viewed pre-recorded data selected by the panel co-chairs that summarized the available clinical evidence. The recordings covered relevant studies evaluating the pharmacokinetics [13,27–30], pharmacogenetics [30], dosing [31], and efficacy and safety of LCPT [27–29,32]. Following review, topics for which consensus was needed were identified and agreed upon by the panel co-chairs (AW and SB) and study team (Evidera). These topics included: important unresolved questions of the scientific community related to the use of LCPT in kidney transplantation, LCPT in the de novo setting, LCPT in the conversion setting, rating the quality of evidence for LCPT, and special populations (eg, rapid metabolizers, the elderly, African Americans), adverse effects (eg, neurologic, impaired glucose tolerance), and adherence concerns. A pre-meeting survey for all panel members was collected based on these topics, forming the basis of future discussion. A workshop was convened where findings from the survey were shared, and panelists explained the rationale behind their survey responses and debated topics raised in the discussion. Workshops provide a valuable way to raise issues for consideration and are a common part of the Delphi process in many studies [9,21]. Our workshop resulted in the development of the Delphi panel questionnaire.
DELPHI PANEL SURVEY:
The execution phase of the Delphi panel survey of LCPT use in kidney transplantation consisted of 3 blinded rounds, 2 survey rounds, and 1 interpretation/consolidation and consensus round (Figure 1). Round 1 of the Delphi panel survey consisted of 12 open-ended online survey questions and was completed by panelists between April 12–23, 2022. Round 2 consisted of 6 open-ended and 18 close-ended online survey questions and was completed between July 28–August 15, 2022, following an additional email round for consensus on 1 statement. Consensus for a statement was achieved when ≥75% (at least 9 of 12 panelists) responded “agree strongly” or “agree with reservation.” Panelists with reservations could explain what these were in detail using an open dialogue box in the survey, and these comments were considered in the revision of statements. Other options available included “disagree strongly,” “disagree,” and “undecided.”
Results
DEVELOPMENT OF THE DELPHI PANEL QUESTIONNAIRE:
The panel of 12 experienced clinicians, with an average of 19.4±6.6 years in practice, consisted of 9 nephrologists, 2 pharmacists, and 1 surgeon. Eleven of the 12 panelists were from centers that transplanted over 100 transplants per year, and the collective transplant volume of the centers represented by the panelists was ~10% of the number of transplants performed annually in the US. Panelists were in clinical leadership positions at their institutions and spent over half their time (53%) on direct patient or transplant-related care and approximately a quarter (23%) on research. The primary practice setting was an academic teaching hospital for 10 out of 12 panelists and a non-academic teaching hospital for the remaining 2. Individual assessments of the quality of evidence for LCPT are shown in Table 1 for special populations and in Table 2 for adverse effects. Ten panelists felt there were more unresolved questions about LCPT to be addressed in a de novo setting than in a conversion setting.
DELPHI PANEL SURVEY:
Based on the post-workshop memorandum and identified topics of interest, a total of 23 statements for consensus were generated for round 1 and categorized by setting – de novo versus conversion – and by topic: (1) clinical use of LCPT, (2) general dosing guidelines, and (3) challenges to using LCPT. Fifteen of the original statements were statements addressing the de novo setting, 7 were statements addressing the conversion setting, and 1 original statement addressed both settings.
In round 1, consensus was achieved for 9/15 statements on the clinical use of LCPT, and 2/4 statements on general dosing guidelines 2/4 statements on challenges to using LCPT (Figure 2, Tables 3, 4). No further revision was carried out on 5 statements from round 1: 3 statements were dropped due to a sizeable lack of consensus, weak evidence, and/or poor alignment of the statement with clinical practice, and 2 statements were merged to create a new statement in round 2. In round 2, a total of 6 modified statements from round 1 were administered to panelists. Consensus was achieved for all 6 statements: 3/3 statements on the clinical use of LCPT, 1/1 for general dosing guidelines, and 2/2 statements on challenges to using LCPT (Figure 2, Tables 3, 4).
The final recommendations on the use of LCPT (Envarsus XR®) in kidney transplantation are summarized in Table 5. Consensus was achieved on the use of LCPT in kidney transplantation for 12 de novo setting statements, 6 conversion setting statements, and 1 statement common to both settings.
Discussion
Delphi methodology is a proven research tool that can generate consensus recommendations in a more rigorous, unbiased manner than other methods when robust clinical trial data are not available. Using Delphi methodology, US clinical experts in kidney transplantation reached consensus on many aspects of the clinical use, use challenges, and general dosing associated with LCPT in kidney transplantation in both de novo and conversion settings. The findings of this Delphi consensus survey will help to fill knowledge gaps and provide guidance regarding utilization of once-daily LCPT in kidney transplantation in a real-world setting, particularly in the de novo setting.
Outstanding issues identified by panelists at the outset of the study included the initial dosing of LCPT as maintenance immunosuppressive medication in both de novo and conversion settings, methods for monitoring and achieving therapeutic levels using LCPT (especially in the context of interpatient variability), and agreement about logistical issues and suggestions for ways to address them (eg, treatment protocols, formulary listings, and impact on pharmacist time/resources). Our study has successfully addressed many of these areas with new consensus statements. Guidance regarding initial dosing of LCPT in the de novo setting with concurrent depleting antibody therapy (Table 3, Statements 8 and 10), and weight-based dosing considerations in the de novo setting (Table 3, Statement 8a), are important real-world issues that prior published data have not adequately addressed. Indications for conversion (eg, neurological adverse effects, patient subtypes) were critically considered based on existing data, and the Delphi panel was able to reach a consensus in providing recommendations for and against the use of LCPT (Table 4).
Expert opinion can supplement other forms of data derived from randomized multicenter trials, meta-analyses, or single-center published experiences and provide guidance for future areas needing study and attention. Several panelists noted the importance of demonstrating the value of LCPT compared with IR-Tac, beyond that which has been shown previously [10,28,29]. Several outcomes were highlighted for potential future study, including long-term survival, cost-effectiveness, glomerular filtration rate (GFR), and biomarkers, including donor-specific antibody (DSA). Other outcomes included associations of endpoints of area under the curve (AUC)/trough levels, patient-relevant outcomes including adherence, and quality-of-life assessments.
In addition to identifying the benefits of LCPT, panelists also acknowledged challenges with changing institution-specific treatment protocols or formulary listings for immunosuppressants. Often, institutional inertia is driven by a lack of experience using novel agents (here, LCPT). Providing guidance for initial dosing and monitoring in the de novo setting should assist in addressing clinical concerns regarding use, but additional logistical and institutional barriers exist. Some panelists mentioned the need for demonstrable benefits to make the change in mindset worthwhile. An existing challenge regarding the inclusion of LCPT in formularies is the absence of non-renal transplant indications.
Our study found that the quality of published evidence supporting the use of LCPT for special patient populations LCPT varied (Table 1). Care was taken evaluating the transplant literature, as separate concepts are sometimes intermingled; for instance, race, high immunologic risk, and rapid metabolism. For rapid metabolizers and African Americans, the quality of evidence was generally considered moderate-to-high, while for the elderly, the quality of evidence was considered low-to-moderate. The quality of evidence for other patient populations ranged from very low to moderate. Further research in these patient populations will be of value. It is uncertain whether dose requirements of LCPT differ for patients with gastric motility concerns (eg, diabetes and gastroparesis) due to a lack of evidence. In several cases, the lack of data to support the statements identified for consensus did not permit panelists to ratify certain statements despite their clinical importance (Figure 2).
Regarding the use of LCPT to address specific adverse effects, our study found a general lack of quality evidence (Table 2). The quality of evidence for neurological adverse effects was perceived to be the highest, with panelists’ ratings varying from low to high. The quality of evidence for adherence concerns was considered to be low-to-moderate, for impaired glucose tolerance it was very low-to-moderate, and for other adverse effects it was very low-to-low. Overall, the panelists found consensus in the recommendation for the use of LCPT in the setting of neurocognitive adverse effects for patients on an IR-Tac-based regimen.
Delphi methodology is a valuable tool for reaching consensus in areas of clinical management that lack sufficient data, but it is not without weaknesses. Disadvantages of Delphi methodology include variation in methods due to a lack of universally acknowledged guidelines, a lack of definition of what constitutes an “expert,” the small size of expert panels, and difficulties ensuring anonymity is guaranteed. To address these concerns, this study identified experts as clinicians with experience in treating kidney transplantation. It included panelists from different clinical backgrounds with attention to different geographic areas and practices, to provide additional expertise. Pros and cons exist for having clinical experience in LCPT. It might be perceived that panelists without personal clinical experience in LCPT are preferable as they would assess evidence on LCPT more objectively. However, it could be argued that panelists with experience using LCPT possess real-world insights that those without experience lack.
Although total anonymity was not maintained during the study as panelists met during the workshop, the workshop was not used to discuss consensus but to develop statements, and this type of workshop is a common feature in Delphi studies [9,21]. Following the development of consensus statements, the survey was conducted online, so panelists were unaware of any individual’s specific feedback. The wide variation in panelists’ assessments of priorities and of the strength of the literature should allay concerns of the scientific community about potential conflicts of interest and facilitate the acceptance of consensus statements generated by the study.
Conclusions
The Delphi process generated consensus statements by expert clinicians to inform clinical decision-making for the use of LCPT in de novo kidney transplant recipients and to guide the optimal use of LCPT in conversion kidney transplant recipients. These consensus statements provide a real-world guide to using LCPT in kidney transplantation, especially in a de novo setting, for which guidance is currently lacking. The consensus statements are particularly relevant to clinical practice, based on the clinical expertise of the panelists and the structured approach provided by Delphi methodology for developing and evaluating consensus statements.
Data Availability Statement
Data from this study are available from the corresponding author, Dr Alexander Wiseman, upon request.
Figures
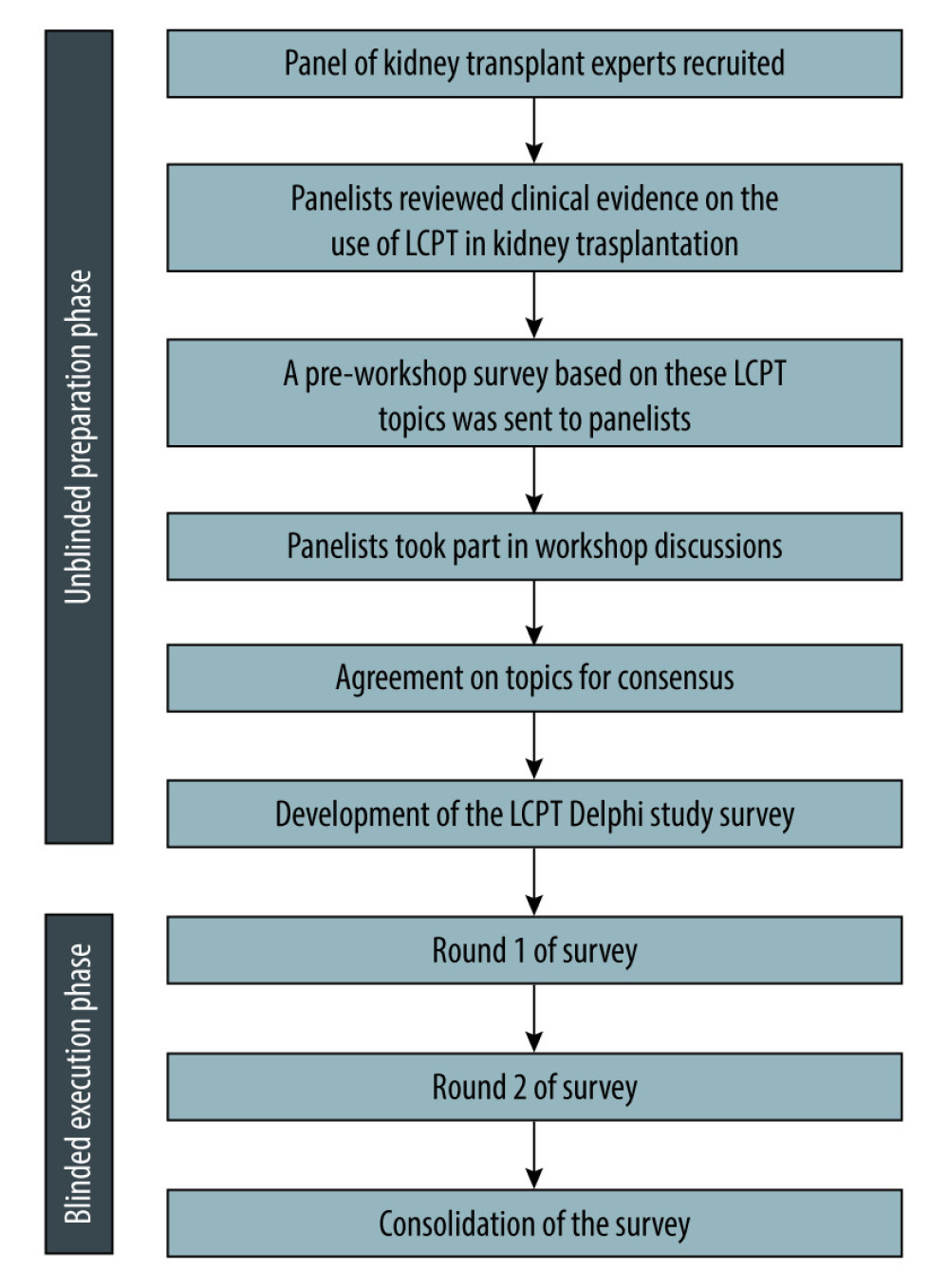 Figure 1. Delphi study flow chart. Software used for the creation of the figure: PowerPoint (version 2310, Microsoft). LCPT – once-daily extended-release oral tacrolimus.
Figure 1. Delphi study flow chart. Software used for the creation of the figure: PowerPoint (version 2310, Microsoft). LCPT – once-daily extended-release oral tacrolimus. 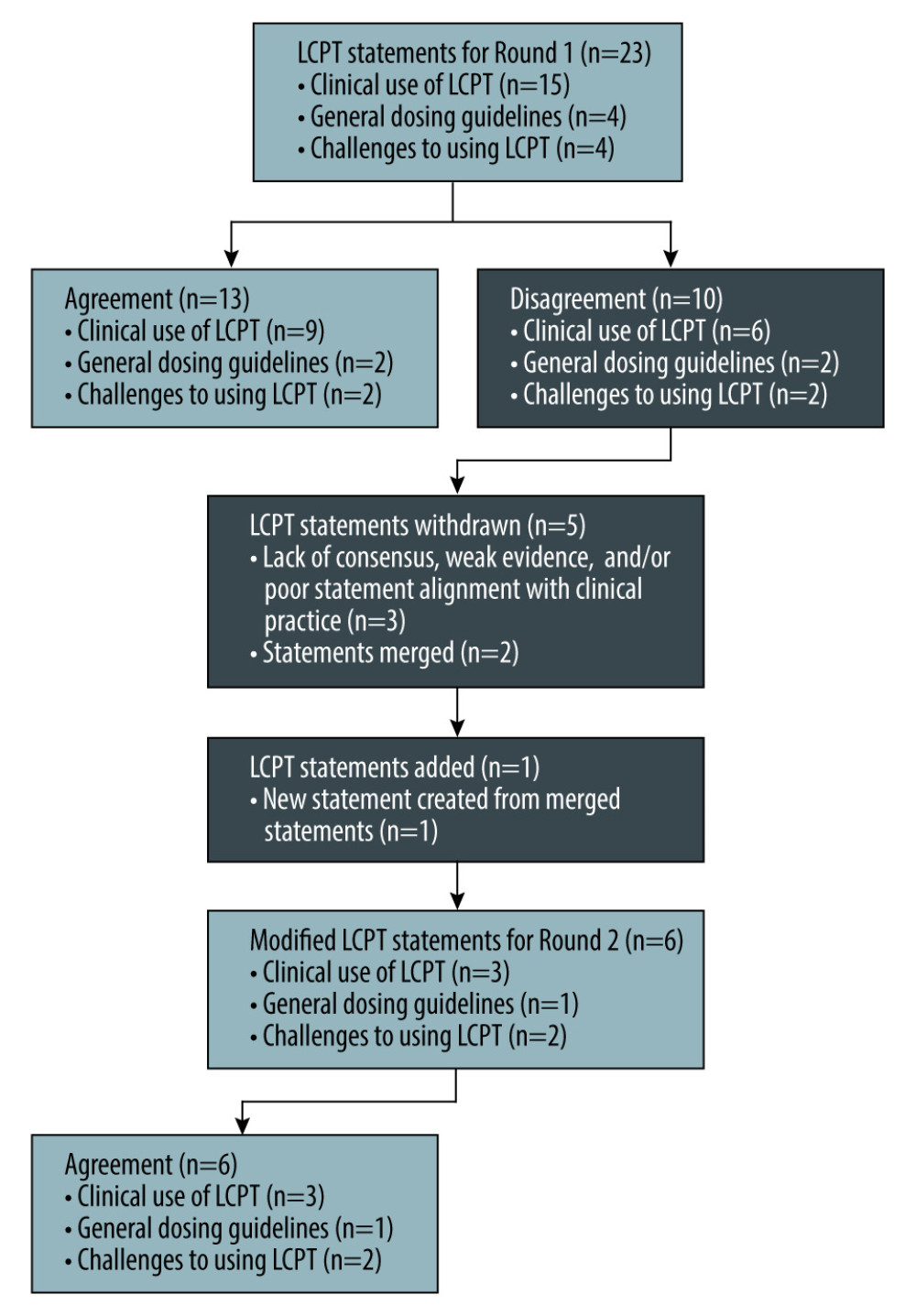 Figure 2. LCPT consensus statement flow chart. Software used for the creation of the figure: PowerPoint (version 2310, Microsoft). LCPT – once-daily extended-release oral tacrolimus.
Figure 2. LCPT consensus statement flow chart. Software used for the creation of the figure: PowerPoint (version 2310, Microsoft). LCPT – once-daily extended-release oral tacrolimus. Tables
Table 1. Quality of published evidence: patient populations for LCPT.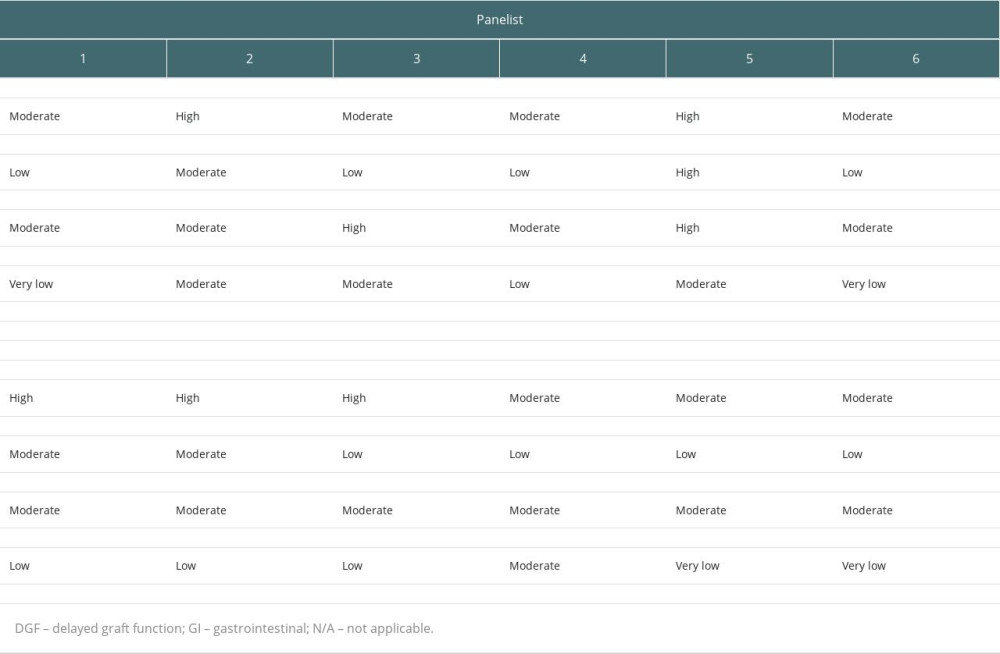 Table 2. Quality of published evidence: adverse effects with LCPT.
Table 2. Quality of published evidence: adverse effects with LCPT.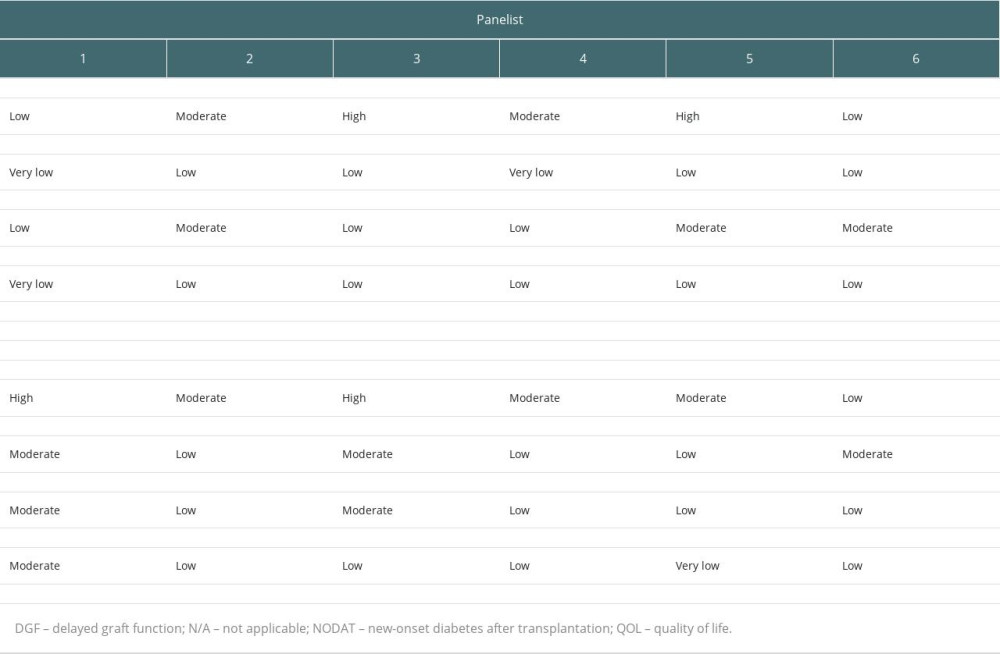 Table 3. Delphi statement progression, LCPT (Envarsus XR®) use in a de novo setting.
Table 3. Delphi statement progression, LCPT (Envarsus XR®) use in a de novo setting.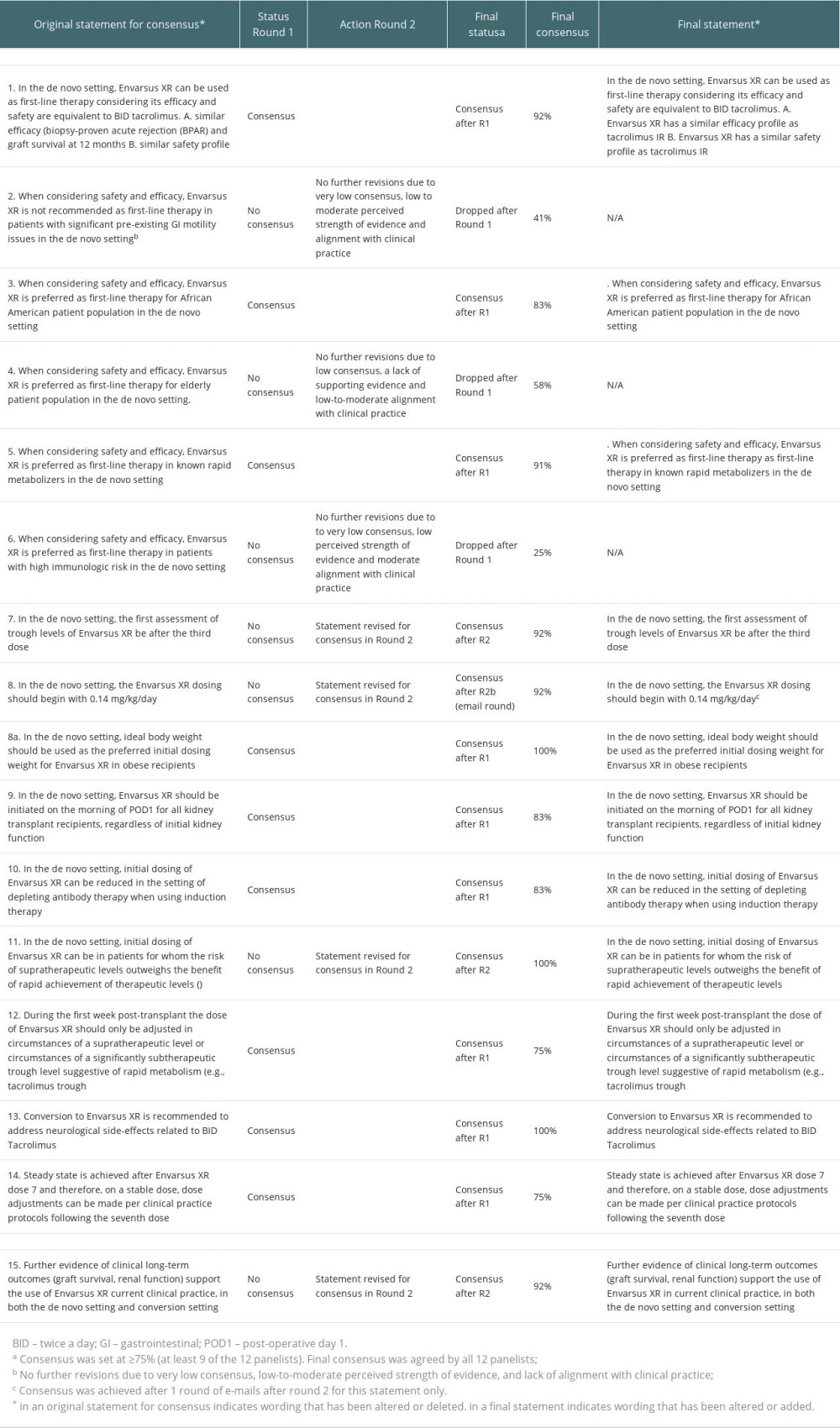 Table 4. Delphi statement progression, LCPT (Envarsus XR®) use in a conversion setting.
Table 4. Delphi statement progression, LCPT (Envarsus XR®) use in a conversion setting.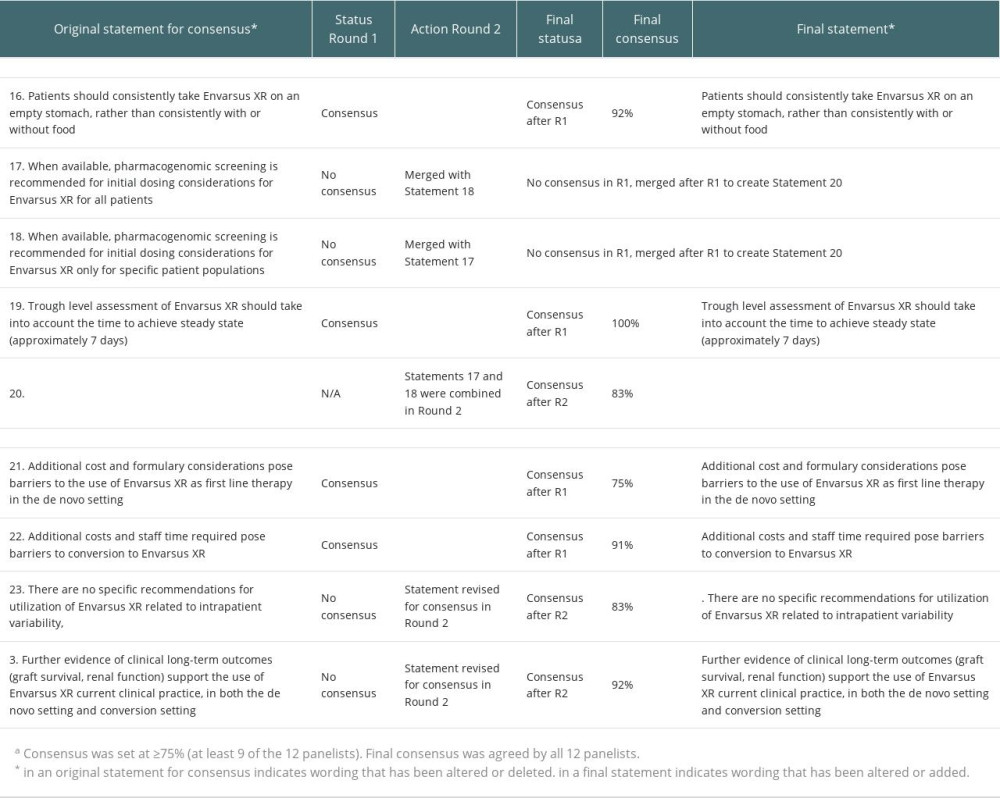 Table 5. Final recommendations on the use of LCPT (Envarsus XR®) in kidney transplantation.
Table 5. Final recommendations on the use of LCPT (Envarsus XR®) in kidney transplantation.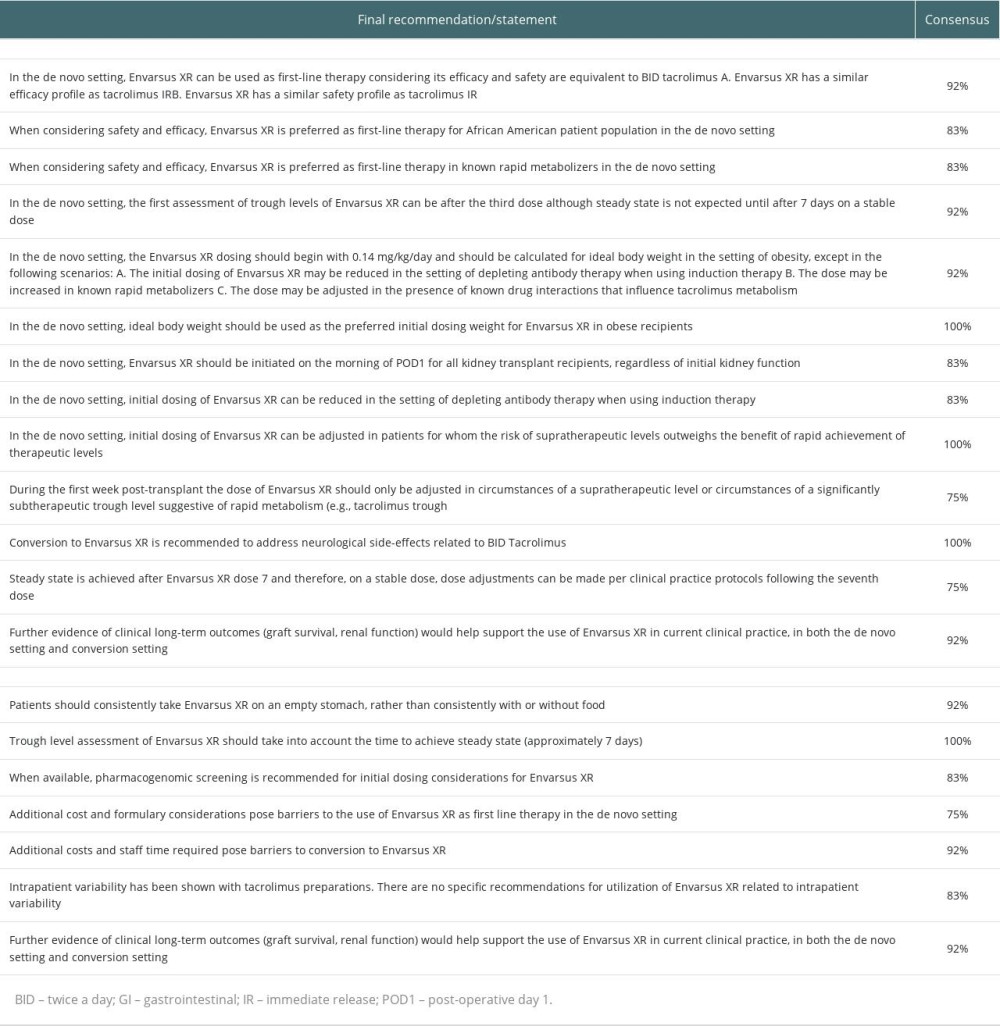
References
1. Philosophe B, Leca N, West-Thielke PM, Evaluation of flexible tacrolimus drug concentration monitoring approach in patients receiving extended-release once-daily tacrolimus tablets: J Clin Pharmacol, 2018; 58(7); 891-96
2. Lentine KL, Smith JM, Miller JM, OPTN/SRTR 2021 Annual Data Report: Kidney: Am J Transplant, 2023; 23(2 Suppl 1); S21-S120
3. US Food and Drug Administration, 2015 https://www.envarsusxr.com/images/1188/envarsus-xr-pi-and-patient-medication-guide.pdf
4. US Food and Drug Administration, 2015 https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/204096s003s004lbl.pdf
5. Tremblay S, Alloway RR, Clinical evaluation of modified release and immediate release tacrolimus formulations: AAPS J, 2017; 19(5); 1332-47
6. Sabbatini M, Garofalo G, Borrelli S, Efficacy of a reduced pill burden on therapeutic adherence to calcineurin inhibitors in renal transplant recipients: An observational study: Patient Prefer Adherence, 2014; 8; 73-81
7. Valente G, Rinaldi L, Sgambato M, Piai G, Conversion from twice-daily to once-daily tacrolimus in stable liver transplant patients: Effectiveness in a real-world setting: Transplant Proc, 2013; 45(3); 1273-75
8. Kuypers DR, Peeters PC, Sennesael JJ, Improved adherence to tacrolimus once-daily formulation in renal recipients: A randomized controlled trial using electronic monitoring: Transplantation, 2013; 95(2); 333-40
9. Nelson J, Alvey N, Bowman L, Consensus recommendations for use of maintenance immunosuppression in solid organ transplantation: Endorsed by the American College of Clinical Pharmacy, American Society of Transplantation, and the International Society for Heart and Lung Transplantation: Pharmacotherapy, 2022; 42(8); 599-633
10. Bunnapradist S, Rostaing L, Alloway RR, LCPT once-daily extended-release tacrolimus tablets versus twice-daily capsules: A pooled analysis of two phase 3 trials in important de novo and stable kidney transplant recipient subgroups: Transpl Int, 2016; 29(5); 603-11
11. Oberbauer R, Bestard O, Furian L, Optimization of tacrolimus in kidney transplantation: New pharmacokinetic perspectives: Transplant Rev (Orlando), 2020; 34(2); 100531
12. Brunet M, van Gelder T, Asberg A, Therapeutic drug monitoring of tacrolimus-personalized therapy: Second consensus report: Ther Drug Monit, 2019; 41(3); 261-307
13. Tremblay S, Nigro V, Weinberg J, A steady-state head-to-head pharmacokinetic comparison of all FK-506 (Tacrolimus) formulations (ASTCOFF): An open-label, prospective, randomized, two-arm, three-period crossover study: Am J Transplant, 2017; 17(2); 432-42
14. Grinyó JM, Petruzzelli S, Once-daily LCP-Tacro MeltDose tacrolimus for the prophylaxis of organ rejection in kidney and liver transplantations: Expert Rev Clin Immunol, 2014; 10(12); 1567-79
15. Tan T, Bunnapradist S, Comparing the pharmacokinetics of extended-release tacrolimus (LCP-TAC) to immediate-release formulations in kidney transplant patients: Expert Opin Drug Metab Toxicol, 2021; 17(10); 1175-86
16. Kidney Disease: Improving Global Outcomes Transplant Work Group, KDIGO clinical practice guideline for the care of kidney transplant recipients: Am J Transplant, 2009; 9(Suppl 3); S1-155
17. US Food and Drug Administration, 2012 https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/050709s031lbl.pdf
18. Dalkey NC: Delphi (P-3704), 1967; 1-10, Santa Monica, CA, RAND Corporation
19. Hsu C, Sandford BA, The Delphi Technique: Making sense of consensus: Practical Assessment, Research, and Evaluation, 2007 https://scholarworks.umass.edu/pare/vol12/iss1/10
20. Antonini A, Stoessl AJ, Kleinman LS, Developing consensus among movement disorder specialists on clinical indicators for identification and management of advanced Parkinson’s disease: A multi-country Delphi-panel approach: Curr Med Res Opin, 2018; 34(12); 2063-73
21. Johnson DA, Katz PO, Armstrong D, The safety of appropriate use of over-the-counter proton pump inhibitors: an evidence-based review and Delphi consensus: Drugs, 2017; 77(5); 547-61
22. Afrouzian M, Kozakowski N, Liapis H, Delphi: A democratic and cost-effective method of consensus generation in transplantation: Transpl Int, 2023; 36; 11589
23. Habbous S, Barnieh L, Litchfield K, A RAND-modified Delphi on key indicators to measure the efficiency of living kidney donor candidate evaluations: Clin J Am Soc Nephrol, 2020; 15(10); 1464-73
24. Sautenet B, Tong A, Manera KE, Developing consensus-based priority outcome domains for trials in kidney transplantation: A multinational Delphi survey with patients, caregivers, and health professionals: Transplantation, 2017; 101(8); 1875-86
25. Shrestha P, Van Pilsum Rasmussen SE, King EA, Defining the ethical considerations surrounding kidney transplantation for frail and cognitively impaired patients: A Delphi study of geriatric transplant experts: BMC Geriatr, 2022; 22(1); 566
26. Tonkin-Crine S, Pruthi R, Taylor DM, Assessing consensus between UK renal clinicians on listing for kidney transplantation: A modified Delphi study: Transplant Direct, 2018; 4(5); e343
27. Rostaing L, Bunnapradist S, Grinyó JM, Novel once-daily extended-release tacrolimus versus twice-daily tacrolimus in de novo kidney transplant recipients: Two-year results of phase 3, double-blind, randomized trial: Am J Kidney Dis, 2016; 67(4); 648-59
28. Budde K, Bunnapradist S, Grinyo JM, Novel once-daily extended-release tacrolimus (LCPT) versus twice-daily tacrolimus in de novo kidney transplants: One-year results of Phase III, double-blind, randomized trial: Am J Transplant, 2014; 14(12); 2796-806
29. Bunnapradist S, Ciechanowski K, West-Thielke P, Conversion from twice-daily tacrolimus to once-daily extended release tacrolimus (LCPT): The phase III randomized MELT trial: Am J Transplant, 2013; 13(3); 760-69
30. Trofe-Clark J, Brennan DC, West-Thielke P, Results of ASERTAA, a randomized prospective crossover pharmacogenetic study of immediate-release versus extended-release tacrolimus in African American kidney transplant recipients: Am J Kidney Dis, 2018; 71(3); 315-26
31. Cibrik D, West-Thielke P, Patel SJ, LCP-tacrolimus (LCPT; Envarsus XR) dosing considerations in de novo kidney transplant recipients: Am J Transplant, 2019; 19(Suppl 3); 5-1167 Abstract 527
32. Langone A, Steinberg SM, Gedaly R, Switching STudy of Kidney TRansplant PAtients with Tremor to LCP-TacrO (STRATO): An open-label, multicenter, prospective phase 3b study: Clin Transplant, 2015; 29(9); 796-805
Figures
Figure 1. Delphi study flow chart. Software used for the creation of the figure: PowerPoint (version 2310, Microsoft). LCPT – once-daily extended-release oral tacrolimus.Figure 2. LCPT consensus statement flow chart. Software used for the creation of the figure: PowerPoint (version 2310, Microsoft). LCPT – once-daily extended-release oral tacrolimus. Tables
Table 1. Quality of published evidence: patient populations for LCPT.Table 2. Quality of published evidence: adverse effects with LCPT.Table 3. Delphi statement progression, LCPT (Envarsus XR®) use in a de novo setting.Table 4. Delphi statement progression, LCPT (Envarsus XR®) use in a conversion setting.Table 5. Final recommendations on the use of LCPT (Envarsus XR®) in kidney transplantation.Table 1. Quality of published evidence: patient populations for LCPT.Table 2. Quality of published evidence: adverse effects with LCPT.Table 3. Delphi statement progression, LCPT (Envarsus XR®) use in a de novo setting.Table 4. Delphi statement progression, LCPT (Envarsus XR®) use in a conversion setting.Table 5. Final recommendations on the use of LCPT (Envarsus XR®) in kidney transplantation. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988