11 June 2024: Original Paper
Physical Activity Levels in Transplant Recipients
Marta Hreńczuk1ACDEF*, Ewelina WasińskaDOI: 10.12659/AOT.944101
Ann Transplant 2024; 29:e944101






Abstract
BACKGROUND: Physical activity is a key factor in improvement of quality of life. This study aimed to assess the extent of physical activity in solid-organ transplant recipients.
MATERIAL AND METHODS: The study involved 106 patients, mostly kidney (64.15%) and liver (28.30%) recipients, observed in a Warsaw transplant center. The study group was dominated by women (56.6%), mean age 49.25±14.09 years, the time since transplantation ranged from 1 month to 28 years, with a mean of 93.9±71.83 months. Recipients were educated about physical activity in the immediate post-transplant period and during follow-up visits. The study was conducted in early 2021 and used the long form of the International Physical Activity Questionnaire (IPAQ) validated for Polish patients, consisting of the of 5 parts – physical activity, professional work, travel, housework, recreation, and time spent sitting – containing a total of 27 questions in the main part of the questionnaire and 7 questions in the introductory part determining the typicality of the last 7 days.
RESULTS: More than half (57.5%) of the transplant recipients reported high levels of physical activity. Patients reported the highest mean physical activity in job-related physical activity (P<0.001). Patients also had high scores for walking and moderate-intensity physical activity, while the lowest mean scores were for leisure-time physical activity, total vigorous-intensity physical activity, and housework-related activity.
CONCLUSIONS: When undertaking physical activity, patients turn to activities that do not involve intense effort, are less physically demanding, and do not result in high energy expenditure. Employed patients had higher PA levels in all domains.
Keywords: Solid-Organ Transplant, Physical activity, International Physical Activity Questionnaire, Humans, Female, Male, Middle Aged, Exercise, adult, transplant recipients, Surveys and Questionnaires, Organ Transplantation, Quality of Life, Poland, Aged, Kidney Transplantation
Introduction
Today, there is a worldwide surge in the number of organ transplants. In 2021, there were 26 378 organ transplantations performed in the European Union, most of which were kidney (15 684) and liver (6483) transplants [1]. There were 1274 deceased donor organ transplants and 64 living donor organ transplants performed in Poland in 2021 [2].
Transplantation aims to improve overall well-being, allowing transplant recipients to resume daily physical, social, and psychological activities. Research on the quality of life in this patient group supports such improvements [3–7]. Physical activity (PA) is a key factor in improving quality of life. Therefore, the health benefits of PA apply not only to individuals who wish to stay healthy, but also individuals with a variety of chronic diseases and disorders, including organ transplant recipients. Robust physical activity after organ transplantation is an important determinant of long-term health [8]. The World Health Organization (WHO) defines physical activity as body movement caused by skeletal muscles that requires the expenditure of energy. PA involves not only professional or amateur participation in various sports or dance activities, but also any activity related to professional work, movement, housework, and recreation. PA levels vary depending on several factors, such as economic factors, social factors, overall health, occupation, and mode of daily transport, as well as environmental factors (eg, terrain) or sports infrastructure [9]. In transplant recipients, PA is crucial for disease prevention, particularly prevention of cardiovascular disease, obesity, or metabolic disorders. Regular physical activity has a long-term positive impact on recovery following various surgical procedures, including transplantation, giving people the opportunity to return to an active life with their families, in society, and in their professional life [10–12]. In the past 2 decades, technical and pharmacological advancements have substantially improved short-term survival after solid-organ transplantation [13], but their benefits on long-term outcomes have been somewhat disappointing [14]. Poor adoption of healthy lifestyle practices (eg, diet, physical activity) undoubtably affects long-term post-transplant physical and mental well-being. The analysis of the literature shows that many solid-organ transplant recipients lead a sedentary, physically inactive life [15–19]. Current recommendations for transplant recipients either refer to general guidelines of physical activity [20] or specifically recommend exercise training [21–24]. There are no general recommendations for leading an active life by organ recipients, nor is there an adequate description of how often, how long, how intensely, and what type of physical activity should be undertaken; therefore, the focus is on everyday activity, including activity related to professional work, traveling, housework, and recreation. Performing any activity that limits a sedentary lifestyle reduces mortality [25] and improves cardiovascular health [26,27], physical fitness [28], and health-related quality of life [29].
The aim of the present study was to assess the extent of physical activity in transplant recipients in 4 key dimensions of human life – work, transportation, housework, and leisure time – and to identify its socio-medical determinants.
Material and Methods
The study involved 106 patients, mostly kidney (64.15%) and liver (28.30%) recipients observed in a Warsaw transplant center and followed up in the outpatient transplant clinic of the Infant Jesus Clinical Hospital, University Clinical Center of the Medical University of Warsaw. Data were collected in February and March 2021. Participation in the study was anonymous and voluntary. The inclusion criteria were age 18 years, ability to complete the questionnaire independently, and verbal consent to participate in the study. The study was approved by the Bioethics Committee of the Medical University of Warsaw (AKBE/236/2020) and was conducted in accordance with the Declaration of Helsinki. It employed a diagnostic survey method and used the long form of the International Physical Activity Questionnaire (IPAQ). The questionnaire was adapted to Polish conditions and accepted by the IPAQ Committee as the official Polish version. In addition, we collected basic socio-demographic (eg, age, gender) and medical (eg, self-assessed current health status, organ type, time since transplantation) data. The IPAQ questionnaire comprises 27 questions categorized into 5 activity domains each containing detailed questions regarding vigorous-intensity activity, moderate-intensity activity, and walking, undertaken by the respondent in the preceding week and related to their work, transportation, housework, sports, and leisure activities. It also assesses the time spent sitting during weekdays (M–F) and weekends. Vigorous-intensity PA was defined as an activity resulting in very fast breathing and a very fast heartbeat (eg, carrying heavy objects, soil digging, aerobics, speed running, cycling at high speed). Moderate-intensity PA was defined as activity leading to slightly faster breathing and a slightly faster heartbeat (eg, carrying lighter objects, cycling at a normal pace, playing volleyball, or brisk walking). We analyzed job-related walking, walking outside (eg, going shopping, going to work), as well as leisure walking. The IPAQ questions make it possible to assess the total weekly energy expenditure, as well as the energy expenditure for each domain. Each type of PA was reported in units of MET-min/week (Metabolic Equivalent of Task), which is calculated by multiplying the coefficient assigned to each PA (vigorous-intensity: 8 MET; moderate-intensity: 4 MET; walking: 3.3 MET) by the number of days per week it was performed and its average duration in minutes per day [30]. Total PA was calculated for each domain by adding up moderate-intensity PA, vigorous-intensity PA, and walking (MET-min/week), and based on this, patients were assigned to one of 3 levels of PA (high, moderate, or low). High PA level requires 3 or more days of vigorous-intensity PA totalling at least 1500 MET-min/week; or 7 or more days of any combination of PA (walking, moderate-intensity PA, or vigorous-intensity PA) totalling more than 3000 MET-min/week. Moderate PA level requires 3 or more days of vigorous-intensity PA not shorter than 20 minutes per day; or 5 or more days of moderate-intensity PA or walking not shorter than 30 minutes per day; or 5 or more days of any combination of PA (walking, moderate-intensity PA, or vigorous-intensity PA) greater than 600 MET-min/week. Low PA level is not engaging in any PA or not meeting the requirements for moderate and high PA levels [31]. The classification and threshold criteria for a given PA level reflect current WHO health guidelines.
For the research results to be reliable, it was assumed that 105 people would participate in the study (so there were 30 respondents for each variable and a 15% excess of respondents was added). Statistical analyses were performed using the IBM SPSS Statistics 27 package. The Kolmogorov-Smirnov test was used to determine whether there was a relationship between the categorical IPAQ score – PA level (high, moderate, or low PA) – and the study variables. A series of cross-tabulations were performed together with the chi-square test of independence. In situations where the assumptions of the chi-square test of independence were violated, the Fisher-Freeman-Halton exact test was used instead. To further explore the relationship between employment and PA, we used Mann-Whitney U and Kruskal-Wallis tests to determine whether employment affects PA domains, as measured by a continuous measure of MET-minutes/week. A significance level of
Results
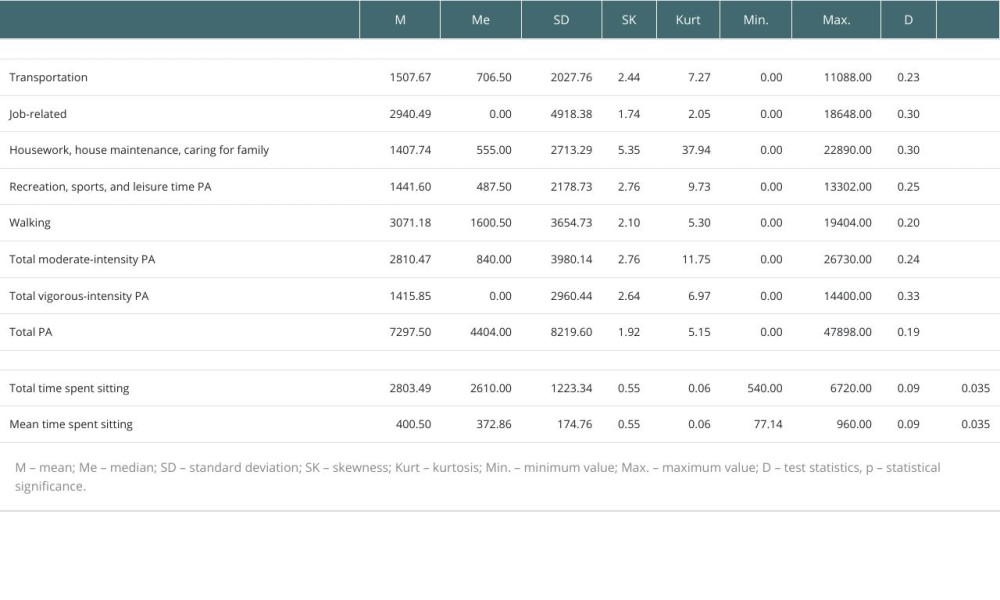
Of the 106 respondents, 60 (56.6%) were female and 46 (43.4%) were male. Respondents ranged in age from 24 to 78 years, with a mean age of 49.29 years (SD 14.09). The time since transplantation ranged from 1 month to 28 years, with a mean of 93.9 months (SD 71.83). In total, there were 68 (64.15%) respondents with a kidney transplant and 30 respondents with a liver transplant (28.30%). The remaining respondents (N=11, 10.38%) had a transplant of a different organ (lung, heart, pancreas). More than half of the respondents (N=55, 51.89%) reported having good health. There were 77 (72.64%) patients who reported having 1 or more chronic diseases. There were 57 (53.77%) employed transplant recipients, 20 (18.86%) respondents were retired, 25 (23.59%) did not work and received disability benefits, and 4 (3.78%) were unemployed. First, the basic descriptive statistics of the studied variables were analyzed together with the Kolmogorov-Smirnov distribution normality test. The test results were statistically significant for all variables, which means that their distribution deviates from the normal distribution. The highest mean PA was reported for job-related PA. Patients also reported high levels of walking and moderate-intensity PA, while the lowest mean scores were found for leisure-time PA, total vigorous-intensity PA, and household PA (Table 1).
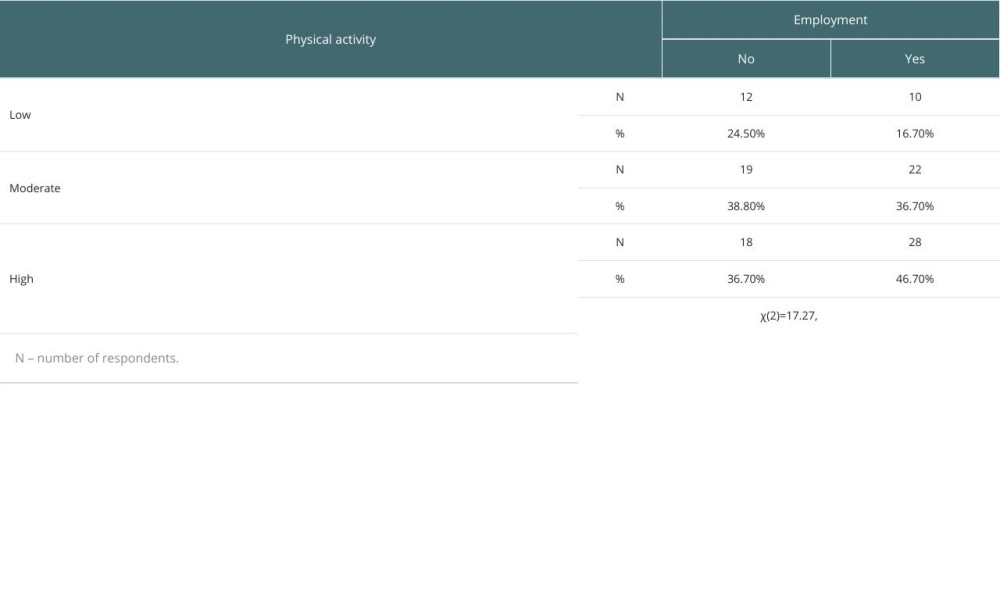
There were 61 (57.5%) respondents with high PA levels, 30 (28.3%) with moderate PA levels, and 15 (14.2%) with low PA levels. The analysis showed a statistically significant relationship only between employment and PA (
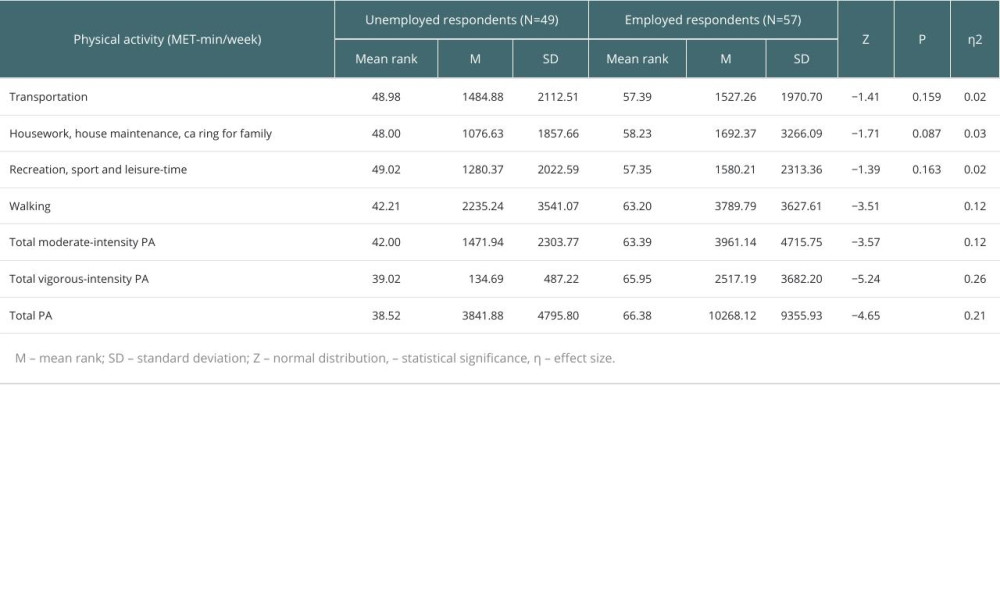
In further analysis of the relationship found between employment and physical activity, we tested whether employment affected PA levels in different domains, as measured by MET-minutes/week (Table 3). There were no statistically significant differences between the employed and unemployed respondents for activities related to transportation, housework, and leisure time. In contrast, we found that the employed respondents had statistically significantly higher PA levels related to walking, moderate-intensity PA, total moderate-intensity PA, vigorous-intensity PA, and total PA.
Discussion
Physical activity is an integral part of human life, but its intensity varies depending on many factors. The overall benefits of PA include reduced cardiovascular and cancer risk, as well as beneficial effects on metabolic, muscular, skeletal, digestive, reproductive, and mental health [32,33]. Regular moderate-intensity PA is also associated with lower rates of infection; however, the opposite effect was observed with strenuous exercise [34]. Research conducted on a cohort of 10 transplant recipients and 10 healthy controls suggests that that people after solid-organ transplantation are at increased risk for infection upon contact with a pathogen in the early aftermath of strenuous exercise [35]. The WHO recommends ≥150 minutes per week of moderate-intensity PA or ≥75 minutes per week of vigorous-intensity PA, or an equivalent combination of moderate- and vigorous-intensity aerobic PA [36].
Physical activity benefits people of all ages and health conditions, including those with chronic diseases [37,38]. PA can reduce risk factors for the development of conditions such as hypertension, obesity, and hyperlipidaemia, thereby slowing the progression of cardiovascular disease (CVD), which is a major cause of mortality in transplant recipients [10,11]. CVD risk factors include hypertension, diabetes, hyperlipidemia, smoking, diet, obesity, and a sedentary lifestyle or lack of regular physical activity. PA reduces many of these risk factors [39,40]. Corticosteroids, when used as part of immunosuppressive therapy, can also cause many adverse effects, including weight gain, osteoporosis, and sarcopenia [11,41,42].
The study participants demonstrated high levels of PA regardless of gender, age, transplanted organ, and time after transplantation. Van Adrichem et al [16] showed that factors significantly associated with lower PA included female gender, younger age, unemployment or retirement, and physical limitations, as well as low expectations and self-confidence. Transplant type had no significant effect on PA. A study by Kotarska et al [43] of 107 liver recipients also found no correlation between PA and age or gender, although there was a correlation between PA and time since transplantation. Both our own study and that of Kotarska et al [43] showed a correlation between employment and PA. Employed patients reported significantly higher activity in each domain as well as total PA as compared to the unemployed participants.
The total PA of the employed liver recipients was on average 5668.2±4787.0 MET-min/week, while it was 3797.9±1852.8 MET-min/week for the non-employed. In our study, the employed participants reported a total PA of 10268.12±9355.93 MET-min/week, while the total PA of the non-employed participants was 3841.88±4795.80 MET-min/week. This group also included recipients of retirement age, but age did not correlate with the level of physical activity, and the obtained results indicated that recipients who were not working were also highly physically active. Both studies show a particularly large discrepancy between the 2 groups of patients in terms of vigorous-intensity PA, especially in the employed transplant recipients. Masala et al [44] surveyed 54 Italian liver transplant recipients, also using the IPAQ questionnaire. The transplant recipients in the study reported an average total PA of 1413.0±2880.05 MET-min/week. The same study also included a control group of 108 respondents, with an average total PA of 1448.5±3719.01 MET-min/week. The study showed no significant differences between the study group and the control group, suggesting that transplant recipients have a similar PA as the general population. In comparison, the total PA was 7297.5±8219.6 MET-min/week in our study and 4497.1±3375.7 MET-min/week in the study by Kotarska et al [43], showing that Polish transplant recipients have a significantly higher total PA than Italian recipients. In contrast, in a study by Biernat and Piatkowska [45] on 2000 Poles at various stages of life, the average total PA of the Polish population was 2079.9±3293.5 MET-min/week. These findings may confirm that living in a different latitude, climate, or culture affects a person’s PA, leading to significant differences in PA regardless of health status. The difference may result from the understanding of, for example, physical activity. For example, in Poland, people go for walks for a specific purpose, including to maintain physical activity, while for Italians, “la passeggiata” (leisurely social walking) has little to do with a set goal or physical effort.
Further studies of physical activity in transplant recipients should be conducted in larger populations. Our study was also limited by its cross-sectional nature. The cross-sectional design limits the ability to establish causality, and longitudinal studies are needed. We studied the issue at a single point in time, which makes it impossible to assess the dynamics of change. The survey was questionnaire-based, and an objective and reliable PA assessment using questionnaires is difficult, as such tools have low reliability and accuracy [46]. First, the respondent may not answer honestly, which has a significant impact on the results. Second, it is impossible to verify whether the respondent actually does the type of activity indicated or to determine its frequency and duration. The subjective perception of one’s own activity is also of importance. Biernat et al [47] found that young adults tended to overestimate their activity when completing the IPAQ alone. Respondents may find it difficult to categorize the intensity of a particular activity they are assessing based on the symptoms listed, such as accelerated breathing or heart rate. As they have to use rather imprecise concepts, the data obtained are not very accurate. It seems that the presence of a trained interviewer during the completion of the questionnaire could be helpful. Biernat et al [47] used the short version of the IPAQ in their study, with some of the respondents completing it alone and others completing it with the interviewer. The way in which the questionnaire was administered was found to have a significant effect on the results obtained. In the group that completed the questionnaire alone, 80.5% of the respondents had a high level of physical activity compared to just over 23% in the other group. Given the studies cited above, this result should be treated with caution, as respondents are likely to overestimate their own PA. The recipients completed the survey questionnaire themselves, which may explain the good results.
A decline in physical activity is noticeable in patients by the time organ failure develops, and usually reaches its peak when end-stage organ failure occurs. However, transplantation does not always solve the problem of reduced physical activity due to frailty [48–51]. In the case of liver diseases, frailty is much more common in recipients who were transplanted due to metabolic dysfunction-associated steatotic liver disease (MASLD) [52]. Despite the return of function of previously ineffective organs, patients after the procedure still struggle with low circulatory and respiratory efficiency or muscle weakness causing rapid fatigue, which constitutes a barrier to physical activity. In the research of Lai et al, patients who exhibited frailty pre-transplant reported more difficulty with everyday activities (21% versus 10%) and were more likely to be unemployed or receive disability benefits 1 year after the transplant (38% versus 29%) than non-frail transplant recipients [52]. Reduced activity may also be caused by prolonged hospitalization, taking immunosuppressive drugs, and episodes of organ rejection. Patients may also suffer from nutritional deficiency caused by pre-transplant dietary recommendations, causing general malaise and weakness [51]. Further research on physical activity should be prospective and long-term, taking into account the previously mentioned variables and use, in addition to the survey questionnaire, other available methods, such as those indicated in the frailty assessment.
In our center, patients only receive recommendations about performing daily activities provided by doctors and nurses. Therefore, these activities were the subject of the study. There is an increasing number of studies indicating the need to educate recipients regarding recommended physical exercise and aerobic exercises and their importance for the recipient’s life and the functioning of the transplant. More and more often, the need for prehabilitation before transplantation is indicated, which includes physical activity, which may have therapeutic and preventive significance and be considered a non-pharmacological therapy. Unfortunately, we still know little about what exercises to recommend to recipients, how often and for how long, and what their actual impact is in this group of patients. Further research is needed.
Short-term patient survival after organ transplantation has improved significantly and the focus of research has shifted to long-term patient survival, also including the importance of PA for beneficial health outcomes. It is important to remember that PA is a preventive measure with a lower economic burden than pharmacotherapy and that it has beneficial effects in both the prevention and treatment of many diseases. Based on the present research and other reports, it is not clear what factors and mechanisms influence the physical activity undertaken by solid-organ transplant recipients. Moderate-intensity PA appears to be a good choice for transplant recipients, but further, larger-scale studies are needed, as well as and clinical evidence, to assess the impact of PA on graft survival and chronic disease prevention in this patient population.
References
1. https://www.statista.com/statistics/1204326/organ-transplantation-activity-in-the-eu/
2. https://www.poltransplant.org.pl/statystyka_2021.html
3. Åberg F, Quality of life after liver transplantation: Best Pract Res Clin Gastroenterol, 2020; 46–47; 101684
4. Rao S, Ghanta M, Moritz MJ, Constantinescu S, Long-term functional recovery, quality of life, and pregnancy after solid organ transplantation: Med Clin North Am, 2016; 100(3); 613-29
5. Dobbels F, De Bleser L, De Geest S, Fine RN, Quality of life after kidney transplantation: The bright side of life?: Adv Chronic Kidney Dis, 2007; 14; 370-78
6. Riess KJ, Haykowsky M, Lawrance R, Exercise training improves aerobic capacity, muscle strength, and quality of life in renal transplant recipients: Appl Physiol Nutr Metab, 2014; 39; 566-71
7. Kotarska K, Raszeja-Wyszomirska J, Wunsch E, Relationship between pretransplantation liver status and health-related quality of life after grafting: A single-center prospective study: Transplant Proc, 2014; 46(8); 2770-73
8. Dunn MA, Rogal SS, Duarte-Rojo A, Lai JC, Physical function, physical activity, and quality of life after liver transplantation: Liver Transpl, 2020; 26(5); 702-8
9. Złotkowska R, Skiba M, Mroczek A, Negative effects of physical activity and sports training: Hygeia Public Health, 2015; 50(1); 41-46
10. De Smet S, Van Craenenbroeck AH, Exercise training in patients after kidney transplantation: Clin Kidney J, 2021; 14(2); ii15-ii24
11. Sen A, Callisen H, Libricz S, Patel B, Complications of solid organ transplantation: Cardiovascular, neurologic, renal, and gastrointestinal: Crit Care Clin, 2019; 35; 169-86
12. Takahashi A, Hu SL, Bostom A, Physical activity in kidney transplant recipients: A review: Am J Kidney Dis, 2018; 72; 433-43
13. Black CK, Termanini KM, Aguirre O: Ann Transl Med, 2018; 6; 409
14. Rana A, Ackah RL, Webb GJ, No gains in long-term survival after liver transplantation over the past three decades: Ann Surg, 2019; 269; 20-27
15. Wilkinson TJ, Clarke AL, Nixon DGD, Prevalence and correlates of physical activity across kidney disease stages: An observational multicentre study: Nephrol Dial Transplant, 2021; 36; 641-49
16. Van Adrichem EJ, Dekker R, Krijnen WP, Physical activity, sedentary time, and associated factors in recipients of solid-organ transplantation: Phys Ther, 2018; 98; 646-57
17. Masiero L, Puoti F, Bellis L, Physical activity and renal function in the Italian kidney transplant population: Ren Fail, 2020; 42; 1192-204
18. Kallwitz ER, Loy V, Mettu P, Physical activity and metabolic syndrome in liver transplant recipients: Liver Transplant, 2013; 19; 1125-31
19. Van Adrichem EJ, van de Zande SC, Dekker R, Perceived barriers to and facilitators of physical activity in recipients of solid organ transplantation, a qualitative study: PLoS One, 2016; 11; e0162725
20. Burra P, Burroughs A, Graziadei I, EASL clinical practice guidelines: Liver transplantation: J Hepatol, 2016; 64; 433-85
21. Costanzo MR, Dipchand A, Starling R, The International Society of Heart and Lung Transplantation guidelines for the care of heart transplant recipients: J Heart Lung Transplant, 2010; 29; 914-56
22. Wickerson L, Rozenberg D, Janaudis-Ferreira T, Physical rehabilitation for lung transplant candidates and recipients: An evidence-informed clinical approach: World J Transplant, 2016; 6; 517-31
23. Yamagata K, Hoshino J, Sugiyama H, Clinical practice guideline for renal rehabilitation: Systematic reviews and recommendations of exercise therapies in patients with kidney diseases: Ren Replace Ther, 2019; 5; 28
24. Janaudis-Ferreira T, Mathur S, Deliva R, Exercise for solid organ transplant candidates and recipients: A joint position statement of the Canadian society of transplantation and CAN-RESTORE: Transplantation, 2019; 103; e220-e38
25. Tarp J, Fagerland MW, Dalene KE, Device-measured physical activity, adiposity and mortality: A harmonized meta-analysis of eight prospective cohort studies: Br J Sports Med, 2022; 56(13); 725-32
26. Bellizzi V, Cupisti A, Capitanini A, Physical activity and renal transplantation: Kidney Blood Press Res, 2014; 39; 212-19
27. Bull FC, Al-Ansari SS, Biddle S, World Health Organization 2020 guidelines on physical activity and sedentary behavior: Br J Sports Med, 2020; 54; 1451-62
28. Lyden K, Boucher R, Wei G, Targeting sedentary behavior in ckd a pilot and feasibility randomized controlled trial: Clin J Am Soc Nephrol, 2021; 16; 717-26
29. Johnson ST, Diehl-Jones W, Vallance JK, Walking, sedentary time and health-related quality life among kidney transplant recipients: An exploratory study: Transplant Proc, 2016; 48; 59-64
30. Biernat E, International Physical Activity Questionnaire – Polish long version: Med Sportpress, 2013; 1(4); 1-15
31. Biernat E, Stupnicki R, Gajewski AInternational Physical Activity Questionnaire (IPAQ) – Polish version: Wychowanie Fizyczne i Sport, 2007; 51(1); 47-54 [in Polish]
32. McTiernan A, Friedenreich CM, Katzmarzyk PT, Physical activity in cancer prevention and survival: A systematic review: Med Sci Sports Exerc, 2019; 51(6); 1252-61
33. Warburton DER, Nicol CW, Bredin SSD, Health benefits of physical activity: The evidence: CMAJ, 2006; 74; 801-9
34. Nieman DC, Wentz LM, The compelling link between physical activity and the body’s defense system: J Sport Health Sci, 2019; 8; 201-17
35. Königsrainer I, Löffler M, Bühler S, Impact of endotoxin exposure after exhausting exercise on the immune system in solid organ transplant recipients: Exerc Immunol Rev, 2012; 18; 177-83
36. World Health Organization: WHO guidelines on physical activity and sedentary behaviour, 2020, Geneva, World Health Organization https://www.who.int/europe/publications/i/item/9789240014886
37. Nieman DC, Wentz LM, The compelling link between physical activity and the body’s defense system: J Sport Health Sci, 2019; 8(3); 201-17
38. Polski P, Alzubedi A, Kusz M, Rudzki S, Activity after kidney transplant: Journal of Education, Health and Sport, 2018; 8(11); 11-17
39. Mosconi G, Cuna V, Tonioli M, Physical activity in solid organ transplant recipients: Preliminary results of the Italian project: Kidney Blood Press Res, 2014; 39(2–3); 220-27
40. Bishop NC, Stensel DJ, Lindley MR, The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease: Nat Rev Immunol, 2011; 11; 607-15
41. Zelle DM, The role of diet and physical activity in post-transplant weight gain after renal transplantation: Clin Transplant, 2013; 27; 484-90
42. Painter P, Marcus RL, Assessing physical function and physical activity in patients with CKD: Clin J Am Soc Nephrol, 2013; 8; 861-72
43. Kotarska K, Wunsch E, Kempińska-Podhorodecka A, Factors affecting health-related quality of life and physical activity after liver transplantation for autoimmune and nonimmune liver disease: A prospective, single centre study: J Immunol Res, 2014; 2014; 738297
44. Masala D, Mannocci A, Unim B, Quality of life and physical activity in liver transplantation patients: Results of a case-control study in Italy: Transplant Proc, 2012; 44(5); 1346-50
45. Biernat E, Piątkowska M, Stay active for life: Physical activity across life stages: Clinical Interventions in Aging, 2018; 13; 1341-54
46. Lipert A, Jegier A, The measurement of physical activity: Med Sportpress, 2009; 3(6); 155-68
47. Biernat E, Stupnicki R, Lebiedziński B, Janczewska L, Assessment of physical activity by IPAQ questionnaire: Phys Educ Sport, 2008; 52; 83-89
48. Oikonomou IM, Sinakos E, Antoniadis N, Effects of an active lifestyle on the physical frailty of liver transplant candidates: World J Transplant, 2022; 12(11); 365-77
49. Kobashigawa J, Dadhania D, Bhorade S, Report from the American Society of Transplantation on frailty in solid organ transplantation: Am J Transplant, 2019; 19(4); 984-94
50. Tandon P, Zanetto A, Piano S, Liver transplantation in the patient with physical frailty: J Hepatol, 2023; 78; 1105-17
51. Cheng XS, Lentine KL, Koraishy FM, Implications of frailty for peritransplant outcomes in kidney transplant recipients: Curr Transpl Rep, 2019; 6; 16-25
52. Lai JC, Shui AM, Duarte-Rojo A, Association of frailty with health-related quality of life in liver transplant recipients: JAMA Surg, 2023; 158(2); 130-38
In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988