03 December 2024: Original Paper
Hepatopulmonary Syndrome and Liver Transplantation: Impact on Survival and Postoperative Complications
Yin Lai ABCDEF 1,2, Hao-Chien Hung BCD 1,2, Jin-Chiao Lee BCD 1,2, Yu-Chao Wang CDE 1,2, Chih-Hsien Cheng CDE 1,2, Tsung-Han Wu BCD 1,2, Ting-Jung Wu BCD 1,2, Hong-Shiue Chou CDE 1,2, Kun-Ming Chan DEF 1,2, Wei-Chen Lee DEF 1,2, Chen-Fang Lee ACDEF 1,2*
DOI: 10.12659/AOT.945297
Ann Transplant 2024; 29:e945297






Abstract
BACKGROUND: Liver transplantation (LT) is the preferred treatment for patients with cirrhosis who have hepatopulmonary syndrome (HPS). However, the effect of HPS on LT remains controversial. We assessed the correlation between HPS severity and LT survival and compared the incidence of postoperative complications between patients with and without HPS undergoing LT.
MATERIAL AND METHODS: We retrospectively reviewed the recipients who received living-donor LT in our institute between January 2016 and July 2019. Patients with HPS (HPS group) and patients without HPS (non-HPS group) were included in our study. HPS is defined as a defect in arterial oxygenation caused by the presence of intrapulmonary vascular dilatations, which is found by transthoracic echocardiography with pre-existing liver cirrhosis. HPS severity was graded according to the value of partial pressure of arterial oxygen. The demographic characteristics and clinical outcomes between the HPS and non-HPS groups were compared.
RESULTS: A total of 181 patients were enrolled. Among them, 104 patients (57.5%) had HPS. The mean overall survival of HPS and non-HPS groups was 69.82±3.1 vs 63.36±3.8 months, with no significant difference (P=0.332). The overall survival between different degrees of HPS was also compared, and showed no significant difference (P=0.466). The HPS group had a higher incidence of delayed extubation (22.1% vs 10.4%, P=0.028) and chest pigtail catheter insertion (16.3% vs 10.4%, P=0.012). Nevertheless, it did not lead to a longer Intensive Care Unit/hospital stay or higher risk of short-term mortality.
CONCLUSIONS: Patients with HPS tend to have more post-LT pulmonary complications, but the overall survival is not adversely influenced, regardless of the severity of HPS.
Keywords: hepatopulmonary syndrome, End stage liver disease, Liver Transplantation, Humans, Male, Female, Postoperative Complications, Retrospective Studies, Middle Aged, adult, Survival Rate, Incidence
Introduction
Hepatopulmonary syndrome (HPS) and portopulmonary hypertension (POPH) are the 2 representative pulmonary vascular complications in patients with cirrhosis, with quite distinct pathophysiological changes and clincial performances between these complications [1]. While pulmonary vasoconstriction and vascular remodeling result in POPH, pulmonary vasodilation and angiogenesis lead to HPS [1]. Unlike POPH, for which some medical treatments originating from that of idiopathic pulmonary hypertension have been shown to be effective [1,2], medical therapy for HPS is overwhelmingly disappointing.
The incidence of HPS varies from 9.45% to 42.5% according to different diagnostic criterias and populations [3–9]. Diagnosing HPS usually requires the presence of chronic liver disease, specific alveolar-arterial oxygen pressure gradient (≥15 mmHg [10,11] or 20 mmHg [12]), or image evidence of intrapulmonary vascular dilatation, such as contrast-enhanced transthoracic echocardiography (CE-TTE) [10] or Technetium macroaggregated albumin lung perfusion scan [10]. Unlike other consequences with obvious presentations of liver cirrhosis, such as hepatic encephalopathy, esophageal varices, or ascites [13], pulmonary complications are often underdiagnosed, since patients can develop symptomatic hypoxia only at a high grade severity or after exertions.
Liver transplantation (LT) is the only curative management of HPS; however, the severity of HPS cannot be reflected by the model for end-stage liver disease (MELD) score appropriately. Sometimes, it is difficult for waitlist patients with severe HPS to receive transplants, due to a low MELD score, even resulting in high pre- and post-transplantation mortality [14]. The post-LT survival comparisons between patients with and without HPS or between different grades of HPS varies. While some studies demonstrated a worse survival of HPS, others shared the opposite opinion. In 2009, Gupta et al observed a higher post-LT survival rate in patients with HPS, including the severe grade, compared with other reports at that time [15]. In 2013, Lyer et al suggested an improved survival trend of HPS in the setting of MELD exception [16]. Although divergent survival rates were noted in patients with HPS, Goldberg et al also presented a similar post-LT overall survival between HPS and non-HPS patients in 2014 [17].
Owing to the controversy, a better understanding of the impact of HPS on LT is desired, to improve recipient outcomes and even influence graft allocation. In this study, we sought to assess the correlation between HPS severity and LT survival. Because of the paucity of data that address the issue of post-transplant complications associated with HPS, we also aimed to compare the incidence of postoperative complications between HPS and non-HPS patients undergoing LT in our institution.
Material and Methods
PATIENTS:
The data of patients who underwent living-donor liver transplant (LDLT) at Linkou Chang Gung Memorial Hospital between January 2016 to July 2019 were reviewed. In addition to hemogram and blood biochemistry studies, all enrolled patients had records of preoperative CE-TTE and arterial blood gas analysis. Patients who had been intubated before transplantation were excluded. Finally, a total of 181 patients were enrolled. Relevant demographic characteristics, pre-LT laboratory tests, examination results, and post-LT clinical outcomes were collected. This retrospective study was approved by the Ethics Committee and Institutional Review Board of Chang Gung Memorial Hospital (CGMH IRB No.202001325B0).
Definition of HPS and Grading of Severity
HPS is defined as a defect in arterial oxygenation caused by the presence of intrapulmonary vascular dilatations, which is found by CE-TTE in the context of liver disease. HPS severity was graded according to the value of partial pressure of arterial oxygen (PaO2) obtained from arterial blood gas test under room air within 3 days before LT, as follows: mild (PaO2 ≥80 mmHg), moderate (80 >PaO2 ≥60 mmHg), severe (60 >PaO2 ≥50 mmHg), very severe (PaO2 <50 mmHg) grades [18].
GRADING SYSTEM FOR RIGHT-TO-LEFT SHUNT (INTRAPULMONARY SHUNT):
All transthoracic echocardiograms were performed by cardiologists less than 3 months after surgery. A bubble study was used to detect the presence of a right-to-left shunt. Microbubbles were created by the agitated contrast agent, including a 5% glucose solution in water and vitamin C. After injecting 10 cc of contrast solution into the left forearm, visible bubbles in the left atrium and ventricle were recorded. The test was considered positive if more than 4 bubbles appeared between the fourth and sixth heartbeat [19]. We defined a grading system for right-to-left shunt (intrapulmonary shunt) according to the number of bubbles: grade 1 (5–10 bubbles), grade 2 (11–30 bubbles), grade 3 (31–45 bubbles), grade 4 (46–60 bubbles), and grade 5 (>60 bubbles).
LT AND IMMUNOSUPPRESSION PROTOCOL:
Details of pre-LT evaluation and operative procedures were described in our prior studies [20,21]. Our primary immunosuppression protocol contains tacrolimus, corticosteroids, and mycophenolate mofetil. The administration and dose adjustment were dependent on clinical conditions [22]. For hepatocellular carcinoma, we followed the University of California San Francisco criteria for LT [16]. A special protocol for ABO-incompatible LT in our institute was also published previously [22,23].
SHORT-TERM PULMONARY COMPLICATIONS:
Delayed extubation was defined as postoperative mechanical ventilation use for more than 48 h. Re-intubation after removal of an endotracheal tube within 7 days was recorded. Within the first week after LT, patients with chest radiographs compatible with pleural effusion/pulmonary edema, or even requiring chest pigtail catheter insertion, were identified. Positive sputum cultures with new infiltrates on chest radiographs were considered to indicate pneumonia. Weekly qPCR assay was performed routinely before discharge to determine cytomegalovirus (CMV) infection. The diagnosis of early allograft dysfunction is based on the presence of any of the following: hyperbilirubinemia (>10 mg/dL), prolonged international normalized ratio >1.6 at postoperative day 7, and/or aspartate aminotransferase or alanine aminotransferase >2000 IU/L within the first 7 days [24].
STATISTICAL ANALYSIS:
The demographic characteristics and clinical outcomes between the HPS and non-HPS groups were compared. The significant differences of categorical variables were determined by chi-square and Fisher’s exact tests, and the continuous variables were determined by 2-sample
Results
BASELINE CHARACTERISTICS IN THE HPS AND NON-HPS GROUPS:
The baseline demographic characteristics between patients in the HPS and non-HPS groups are shown in Table 1. Among all enrolled patients (n=181), 104 (57.5%) met our criteria of HPS. Among the patients in the non-HPS group (n=77), only 1 patient had a positive bubble test. There was no significant difference in the value of PaO2 between the HPS and non-HPS groups (P=0.444). In the HPS group, 72 (69.2%), 26 (25%), 2 (1.9%), and 4 (3.8%) patients had mild (PaO2 ≥80 mmHg), moderate (80 >PaO2 ≥60 mmHg), severe (60 >PaO2 ≥50 mmHg), and very severe (PaO2 <50 mmHg) HPS, respectively. Although patients in the non-HPS group had a significantly higher percentage of viral hepatitis (72.7% vs 63.5%, P=0.023), patients in the HPS group were more likely to have Child-Pugh class B or C (83.7% vs 55.8%, P<0.0001). Also, 19 patients in the HPS group and 6 patients in the non-HPS group received ABO-incompatible LDLT (18.3% vs 7.8%, P=0.051). Based on these data, the patients in the HPS group seemed to have a more severe and complicated pre-LT condition.
CORRELATION BETWEEN MELD SCORE AND HPS SEVERITY:
Compared with the non-HPS group, the HPS group had a higher MELD score (16.98±7.1 vs 15.14±9.6,
COMPARISONS OF POSTOPERATIVE COMPLICATIONS BETWEEN HPS AND NON-HPS GROUP:
The comparisons of post-LT complications between the HPS and non-HPS groups are shown in Table 2. Regarding pulmonary complications, there were no significant differences in postoperative pleural effusion/pulmonary edema, pneumonia, or CMV infection between the 2 groups. However, the HPS group had a higher percentage of delayed extubation (22.1% vs 10.4%, P=0.028). A significantly higher rate of chest pigtail catheter insertion for pleural fluid drainage in HPS was also found (16.3% vs 10.4%, P=0.012). Nevertheless, the HPS group did not have a longer Intensive Care Unit (ICU) stay (13.6±9.4 days vs 15.0±9.9 days, P=0.409) or hospital stay (36.0±30.9 days vs 31.4±18.4 days, P=0.097).
Regarding surgical complications, 4 patients in each group received re-laparotomy, owing to the following events: non-HPS: 3 cases of bleeding and 1 case of hepatic artery thrombosis; and HPS: 1 case of bleeding, 1 case of hepatic artery thrombosis, 1 case with wound dehiscence, and 1 case with ischemic bowel disease. No significant difference was noted in the incidence of early allograft dysfunction or 30-day mortality (Table 2). Together, the results demonstrated that the HPS group had a higher incidence of prolonged intubation and chest pigtail catheter drainage for massive pleural effusion, but it did not lead to a longer ICU/hospital stay or higher short-term mortality.
EFFECT OF HPS ON OVERALL SURVIVAL AFTER LT:
After analyzing the baseline characteristics and post-LT complications, we investigated whether HPS had a negative effect on overall survival after LT. The mean overall survival of patients in the HPS and non-HPS groups were 69.82±3.1 vs 63.36±3.8 months, without statistical significance (P=0.332; Figure 1). We also analyzed the overall survival in the subgroups of HPS patients. The estimated overall survival probability for non-HPS and different degrees of hypoxemia in HPS were compared (Figure 2). Since the total case number of severe and very severe subgroups was only 6, these 2 conditions were combined into 1 group. For overall survival, there was no significant difference between these subgroups (P=0.466, Figure 2). Furthermore, the presence of HPS prior to LT did not give additional risks of overall survival to the patients with either high MELD score (≥20) or low MELD scores (<20; P=0.613; Figure 3). These data suggested that pre-existing HPS did not contribute to a poorer survival in patients undergoing LT.
CORRELATION BETWEEN ECHO BUBBLE STUDY AND OVERALL SURVIVAL:
All patients in the HPS group had positive bubble test results, which were distributed across different severities. Five grades of bubble tests were organized into 3 ratings: grade 1, grade 2+3, and grade 4+5. The percentages of patients in grade 1, grade 2+3, and grade 4+5 echo bubble study were 44.2%, 42.3%, and 13.5%, respectively (Table 1). The mean overall survival was 72.74±4.2, 68.47±4.9, and 60.59±9.0 months in the grade 1, grade 2+3, and grade 4+5 groups, respectively (P=0.575; Figure 4). Although no statistically significant difference was found, a declining survival trend was observed between the subgroups categorized by the number of bubbles.
We further analyzed the correlation between baseline PaO2 and the severity grading system of the echo bubble study. The percentages of patients with PaO2 <80 mmHg in grade 1, grade 2+3, and grade 4+5 in the echo bubble study were 30.4%, 25%, and 50%, respectively. A scatter plot displays the correlation between PaO2 and the grading of the echo bubble study in Figure 5, which reveals no specific correlation.
Discussion
Portal hypertension of chronic liver disease makes complicated changes in pathophysiology, leading to an increased formation of endogenous vasoconstrictors or vasodilators at different situations and the development of HPS and POPH [25,26]. In the present study, we retrospectively reviewed the outcomes of patients with HPS who had received subsequent LT. Our results showed that there was no survival difference between HPS and non-HPS groups, indicating HPS is not an absolute contraindication for LT. Despite HPS being frequently graded by the level of PaO2 or echo bubble study, these gradings did not show survival discriminability in our database. Also, we showed that the grading of HPS dis not closely parallel the MELD score, and there was no positive correlation between the value of PaO2 and bubble study grading. As a result, HPS itself, or the severity of hypoxia, should not be considered as a negative predictor for LT.
Even though many studies show a favorable long-term outcome of HPS after LT [16,17], few studies mention the relationship between the short-term pulmonary complications and HPS. Based on our results, patients with HPS were not more susceptible to postoperative pleural effusion, pulmonary edema, pneumonia, or CMV infection. However, for those who developed postoperative pleural effusion, the rate of pigtail catheter insertion in the HPS group was significantly higher than that of the non-HPS group, indicating that HPS increased the severity of pleural effusion. Also, the length of mechanical ventilator use was longer in the HPS group. As for short-term outcomes, the HPS group did not have a higher percentage of 30-day mortality or early allograft dysfunction. Obviously, the improvement of clinical and critical care played a vital role in this regard.
In 2006, Schiffer et al announced an inferior survival of patients with HPS, with 50≤ PaO2 ≤70 mmHg, vs non-HPS [14]. In 2014, Goldberg et al proposed that PaO2 <45 mmHg had a worst survival trend than other grades of HPS, according to the data from United Network for Organ Sharing. In 2021, Kadry et al presented that even though PaO2 <45 mmHg had a lower survival, the median year was actually up to 11.5 [27]. However, we did not find a correlation between PaO2 level and post-LT survival, similar to the results from others [16,28]. In additions, some studies indicated that HPS is associated with a higher MELD score and an increased risk of death [29]; however, our results did not show the same findings. We demonstrated that the presence of HPS prior to LT would not give additional risks of survival to the patients with either high MELD scores (≥20) or low MELD scores (<20). These data suggested that pre-existing HPS does not contribute to a poorer survival in LT patients, regardless of pre-LT hypoxia and marked hepatic dysfunction.
We did not investigate waitlist survival; thus, whether the HPS MELD exception criteria can produce its greatest value by reducing pre-LT mortality remained unknown in our study. In fact, our country does not follow the exception policy for HPS patients. To avoid drop-out due to too severe hypoxia, the exception policy [30] had been established in the United States, ensuring that patients with HPS and hypoxemia (defined as PaO2 <60 mmHg, the severe or very severe stages [19]) are prioritized. The HPS MELD exception criteria [30] is basically supported by 2 arguments: (1) patients with HPS have an increased risk of waitlist death than patients without HPS [27,31], and (2) HPS patients with PaO2 <60 mmHg under room air may have a higher pre-LT mortality rate than those with PaO2 ≥60 mmHg. Aragon Pinto et al published a meta-analysis in 2021 comparing LT outcomes before and after MELD era exceptions. The findings of this meta-analysis highlight the positive effect of MELD exception implementation on the outcomes of liver transplantation in patients with HPS. The improvements in survival rates and post-transplant oxygenation in adult patients show the significance of this scoring system, while the observed increase in post-transplant oxygenation in children is also noteworthy. These results emphasize the importance of considering MELD exceptions in the evaluation and treatment of patients with HPS undergoing liver transplantation [9].
The limitations of this study included that it was retrospective study from a single center, and it had a smaller number of cases in some subgroups, which can affect statistical significance. Since the alveolar-arterial oxygen pressure gradient cannot be calculated easily, PaO2 in arterial blood gas analysis is used to indicate the severity of hypoxemia in HPS [18]. Based on the established relationship between SpO2 and PaO2 under FiO2 21%, SpO2 96% is equal to PaO2 83 mmHg [6,19]. Thus, we used PaO2 80 mmHg or SpO2 96% as the initial step for HPS screening.
Conclusions
HPS should not be considered as a limitation to LT. Although HPS will probably result in a higher rate of post-LT pulmonary complications, including delayed extubation and massive pleural effusion, that require drainage, it does not lead to a significantly decreased overall survival. Our findings help to reevaluate the aftereffects from HPS and establish appropriate selection criteria for LT candidates.
Figures
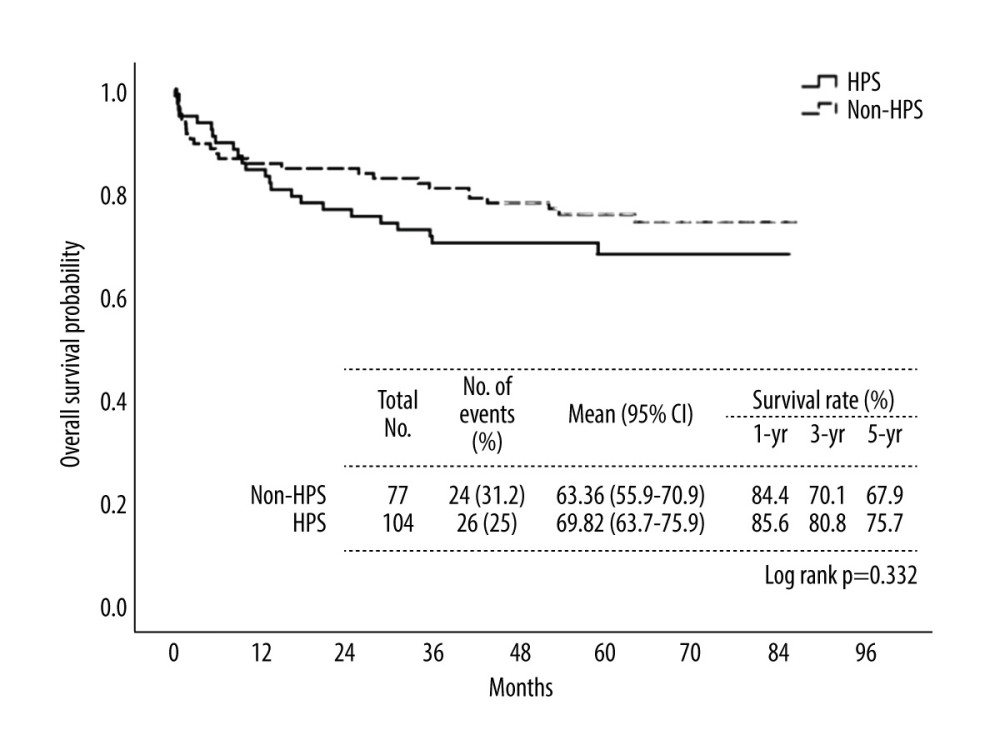 Figure 1. Kaplan-Meier curves displaying the estimated overall survival probability for HPS and non-HPS groups. There was no significant difference between the groups. HPS – hepatopulmonary syndrome. IBM SPSS Statistics (version 27.0) was used for creation of the figure.
Figure 1. Kaplan-Meier curves displaying the estimated overall survival probability for HPS and non-HPS groups. There was no significant difference between the groups. HPS – hepatopulmonary syndrome. IBM SPSS Statistics (version 27.0) was used for creation of the figure. 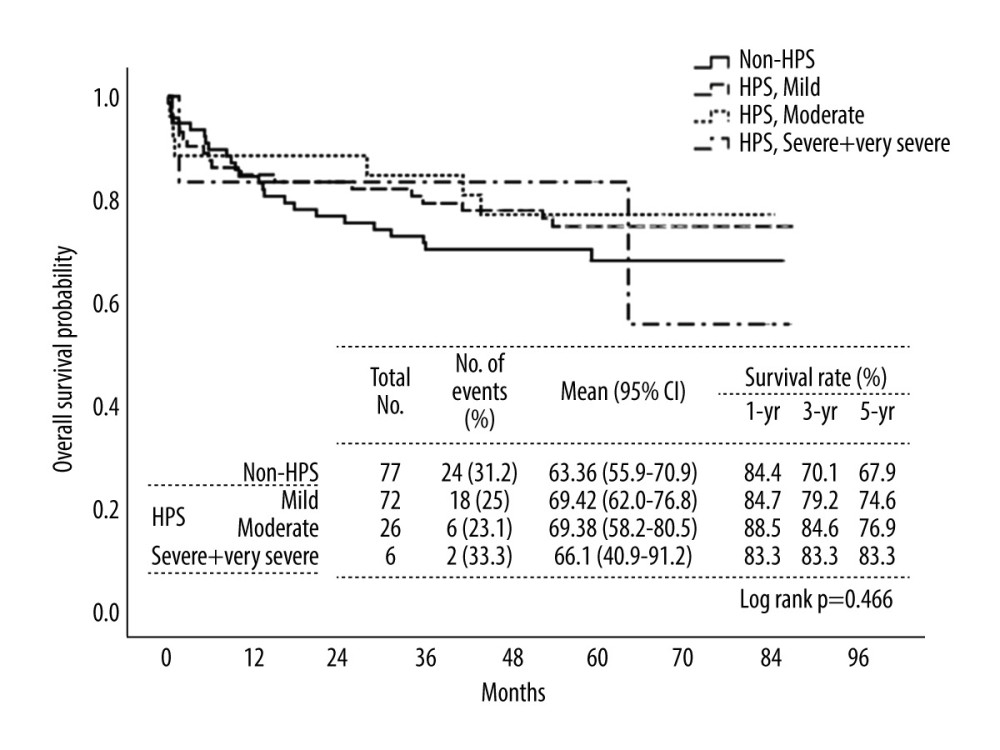 Figure 2. Kaplan-Meier curves displaying the estimated overall survival probability for non-HPS group and different grades of HPS. When comparing patients in the non-HPS and HPS groups with different severity grades, no significant difference was found. The severe and very severe grades were combined due to fewer case numbers. HPS – hepatopulmonary syndrome. IBM SPSS Statistics (version 27.0) was used for creation of the figure.
Figure 2. Kaplan-Meier curves displaying the estimated overall survival probability for non-HPS group and different grades of HPS. When comparing patients in the non-HPS and HPS groups with different severity grades, no significant difference was found. The severe and very severe grades were combined due to fewer case numbers. HPS – hepatopulmonary syndrome. IBM SPSS Statistics (version 27.0) was used for creation of the figure. 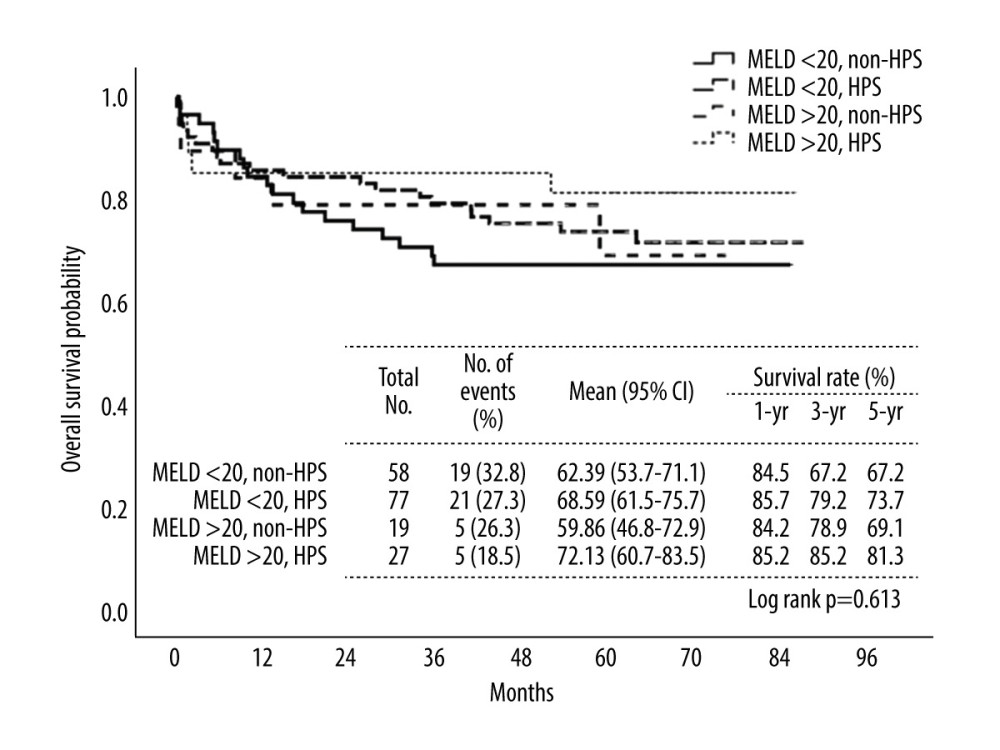 Figure 3. Kaplan-Meier curves displaying the estimated overall survival probability for 4 groups of patients divided by MELD score, with or without HPS. The presence of HPS prior to LT did not give additional risks of overall survival. IBM SPSS Statistics (version 27.0) was used for creation of the figure.
Figure 3. Kaplan-Meier curves displaying the estimated overall survival probability for 4 groups of patients divided by MELD score, with or without HPS. The presence of HPS prior to LT did not give additional risks of overall survival. IBM SPSS Statistics (version 27.0) was used for creation of the figure. 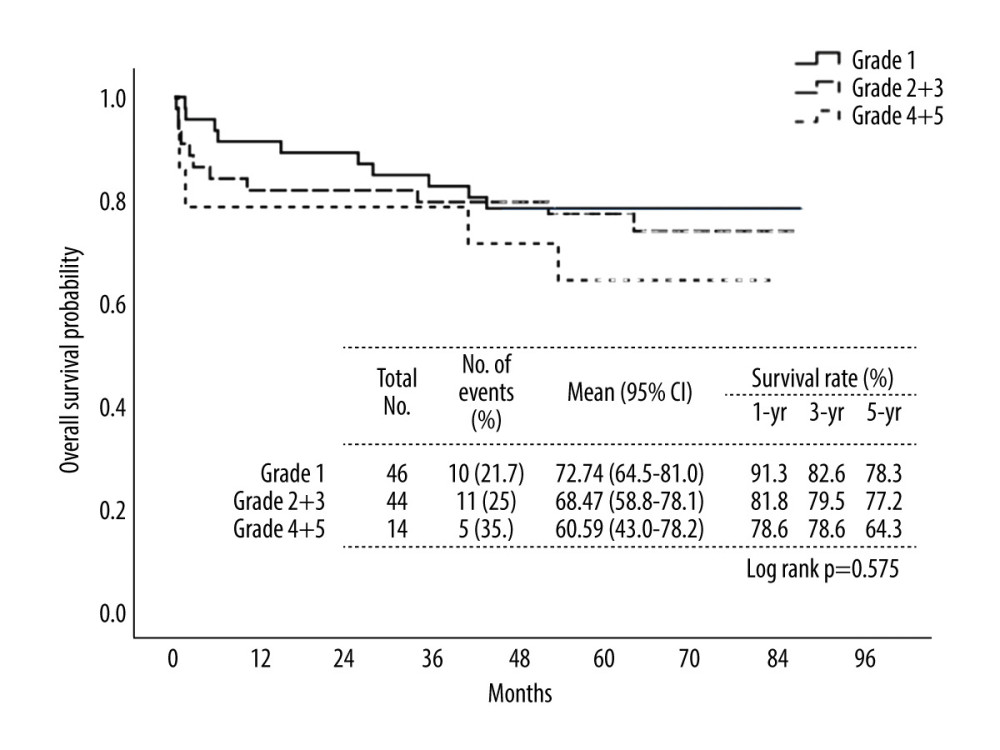 Figure 4. Kaplan-Meier curves displaying the estimated overall survival probability for different grades of echo bubble test results in hepatopulmonary syndrome (HPS). Patients in the HPS group with different echo bubbles test severity had no significant difference in overall survival; however, a declining trend was observed between the subgroups. IBM SPSS Statistics (version 27.0) was used for creation of the figure.
Figure 4. Kaplan-Meier curves displaying the estimated overall survival probability for different grades of echo bubble test results in hepatopulmonary syndrome (HPS). Patients in the HPS group with different echo bubbles test severity had no significant difference in overall survival; however, a declining trend was observed between the subgroups. IBM SPSS Statistics (version 27.0) was used for creation of the figure. 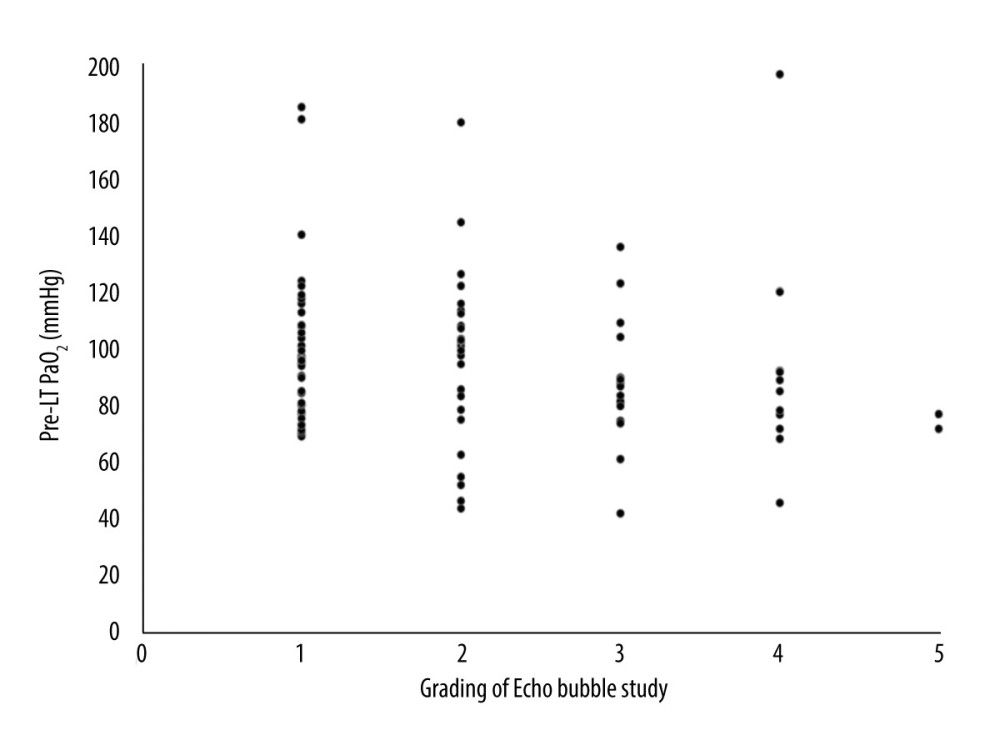 Figure 5. Scatter plot displaying the correlation between pre-liver transplant (LT) PaO2 and echo bubble test grading in hepatopulmonary syndrome (HPS). No specific correlation between pre-LT PaO2 and echo bubble test grading was found. IBM SPSS Statistics (version 27.0) was used for creation of the figure.
Figure 5. Scatter plot displaying the correlation between pre-liver transplant (LT) PaO2 and echo bubble test grading in hepatopulmonary syndrome (HPS). No specific correlation between pre-LT PaO2 and echo bubble test grading was found. IBM SPSS Statistics (version 27.0) was used for creation of the figure. References
1. Weinfurtner K, Forde K, Hepatopulmonary syndrome and portopulmonary hypertension: Current status and implications for liver transplantation: Curr Hepatol Rep, 2020; 19(3); 174-85
2. Saleemi S, Portopulmonary hypertension: Ann Thorac Med, 2010; 5(1); 5-9
3. Cárdenas Ramírez B, Padilla-Machaca PM, Mantilla Cruzatti OHepatopulmonar syndrome and liver transplantation: Experience in the transplantation department of the Guillermo Almenara Irigoyen National Hospital – EsSalud: Rev Gastroenterol Peru, 2018; 38(3); 242-47 [in Spanish]
4. Folador L, Torres FS, Zampieri JF, Hepatopulmonary syndrome has low prevalence of pulmonary vascular abnormalities on chest computed tomography: PLoS One, 2019; 14(10); e0223805
5. Ceza MR, Garcia E, Anselmi CE, Prevalence and characteristics of hepatopulmonary syndrome in children with cirrhosis in southern Brazil: Eur J Gastroenterol Hepatol, 2019; 31(1); 10-15
6. Rose SCP, Cunha DV, Medeiros SBC, Correlation between hepatopulmonary syndrome and oxygen saturation pulse oximetry in cirrhotic patients: Rev Assoc Med Bras (1992), 2020; 66(11); 1577-82
7. Khiangte B, Kothakota SR, Sasidharan M, Prevalence and determinants of hepatopulmonary syndrome in decompensated chronic liver disease: Indian J Gastroenterol, 2020; 39(4); 362-69
8. Han SK, Kim MY, Kang SH, Hepatopulmonary syndrome is related to the development of acute-on-chronic liver failure and poor prognosis in cirrhotic patients: Hepatol Int, 2021; 15(5); 1207-14
9. Aragon Pinto C, Iyer VN, Albitar HAH, Outcomes of liver transplantation in patients with hepatopulmonary syndrome in the pre and post-MELD eras: A systematic review: Respir Med Res, 2021; 80; 100852
10. Rodríguez-Roisin R, Krowka MJ, Hervé P, Fallon MBERS Task Force Pulmonary-Hepatic Vascular Disorders (PHD) Scientific Committee, Pulmonary-hepatic vascular disorders (PHD): Eur Respir J, 2004; 24(5); 861-80
11. Rockey DC, Chung JJ, Reduced nitric oxide production by endothelial cells in cirrhotic rat liver: Endothelial dysfunction in portal hypertension: Gastroenterology, 1998; 114(2); 344-51
12. Swanson KL, Wiesner RH, Krowka MJ, Natural history of hepatopulmonary syndrome: Impact of liver transplantation: Hepatology, 2005; 41(5); 1122-29
13. Simonetto DA, Liu M, Kamath PS, Portal hypertension and related complications: Diagnosis and management: Mayo Clin Proc, 2019; 94(4); 714-26
14. Schiffer E, Majno P, Mentha G, Hepatopulmonary syndrome increases the postoperative mortality rate following liver transplantation: A prospective study in 90 patients: Am J Transplant, 2006; 6(6); 1430-37
15. Gupta S, Castel H, Rao RV, Improved survival after liver transplantation in patients with hepatopulmonary syndrome: Am J Transplant, 2010; 10(2); 354-63
16. Iyer VN, Swanson KL, Cartin-Ceba R, Hepatopulmonary syndrome: Favorable outcomes in the MELD exception era: Hepatology, 2013; 57(6); 2427-35
17. Goldberg DS, Krok K, Batra S, Impact of the hepatopulmonary syndrome MELD exception policy on outcomes of patients after liver transplantation: An analysis of the UNOS database: Gastroenterology, 2014; 146(5); 1256-65e1
18. Fauconnet P, Klopfenstein CE, Schiffer E, Hepatopulmonary syndrome: The anaesthetic considerations: Eur J Anaesthesiol, 2013; 30(12); 721-30
19. Aldenkortt F, Aldenkortt M, Caviezel L, Portopulmonary hypertension and hepatopulmonary syndrome: World J Gastroenterol, 2014; 20(25); 8072-81
20. Wu TJ, Dahiya D, Lee CS, Impact of portal venous hemodynamics on indices of liver function and graft regeneration after right lobe living donor liver transplantation: Liver Transpl, 2011; 17(9); 1035-45
21. Chan KM, Cheng CH, Wu TH, Clinical strategy for the reconstruction of middle hepatic vein tributaries in right liver living donor liver transplantation: World J Surg, 2014; 38(11); 2927-33
22. Lee CF, Cheng CH, Wang YC, Adult living donor liver transplantation across ABO-incompatibility: Medicine (Baltimore), 2015; 94(42); e1796
23. Lee WC, Cheng CH, Lee CF, Quick preparation of ABO-incompatible living donor liver transplantation for acute liver failure: Clin Transplant, 2022; 36(3); e14555
24. Olthoff KM, Kulik L, Samstein B, Validation of a current definition of early allograft dysfunction in liver transplant recipients and analysis of risk factors: Liver Transpl, 2010; 16(8); 943-49
25. Maruyama H, Shiina S, Collaterals in portal hypertension: Anatomy and clinical relevance: Quant Imaging Med Surg, 2021; 11(8); 3867-81
26. Premkumar M, Anand AC, Overview of complications in cirrhosis: J Clin Exp Hepatol, 2022; 12(4); 1150-74
27. Kadry Z, Schaefer E, Krok K: JHEP Rep, 2021; 3(5); 100351
28. Taillé C, Cadranel J, Bellocq A, Liver transplantation for hepatopulmonary syndrome: A ten-year experience in Paris, France: Transplantation, 2003; 75(9); 1482-89 discussion 1446–47
29. Kawut SM, Krowka MJ, Forde KAPulmonary Vascular Complications of Liver Disease Study Group, Impact of hepatopulmonary syndrome in liver transplantation candidates and the role of angiogenesis: Eur Respir J, 2022; 60(2); 2102304 [Erratum in: Eur Respir J. 2023;62(1):2152304]
30. Fallon MB, Mulligan DC, Gish RG, Krowka MJ, Model for end-stage liver disease (MELD) exception for hepatopulmonary syndrome: Liver Transpl, 2006; 12(12 Suppl 3); S105-7 [Erratum in: Liver Transpl. 2008;14(9):1386]
31. Fallon MB, Krowka MJ, Brown RSPulmonary Vascular Complications of Liver Disease Study Group, Impact of hepatopulmonary syndrome on quality of life and survival in liver transplant candidates: Gastroenterology, 2008; 135(4); 1168-75
Figures
Figure 1. Kaplan-Meier curves displaying the estimated overall survival probability for HPS and non-HPS groups. There was no significant difference between the groups. HPS – hepatopulmonary syndrome. IBM SPSS Statistics (version 27.0) was used for creation of the figure.Figure 2. Kaplan-Meier curves displaying the estimated overall survival probability for non-HPS group and different grades of HPS. When comparing patients in the non-HPS and HPS groups with different severity grades, no significant difference was found. The severe and very severe grades were combined due to fewer case numbers. HPS – hepatopulmonary syndrome. IBM SPSS Statistics (version 27.0) was used for creation of the figure.Figure 3. Kaplan-Meier curves displaying the estimated overall survival probability for 4 groups of patients divided by MELD score, with or without HPS. The presence of HPS prior to LT did not give additional risks of overall survival. IBM SPSS Statistics (version 27.0) was used for creation of the figure.Figure 4. Kaplan-Meier curves displaying the estimated overall survival probability for different grades of echo bubble test results in hepatopulmonary syndrome (HPS). Patients in the HPS group with different echo bubbles test severity had no significant difference in overall survival; however, a declining trend was observed between the subgroups. IBM SPSS Statistics (version 27.0) was used for creation of the figure.Figure 5. Scatter plot displaying the correlation between pre-liver transplant (LT) PaO2 and echo bubble test grading in hepatopulmonary syndrome (HPS). No specific correlation between pre-LT PaO2 and echo bubble test grading was found. IBM SPSS Statistics (version 27.0) was used for creation of the figure. Tables
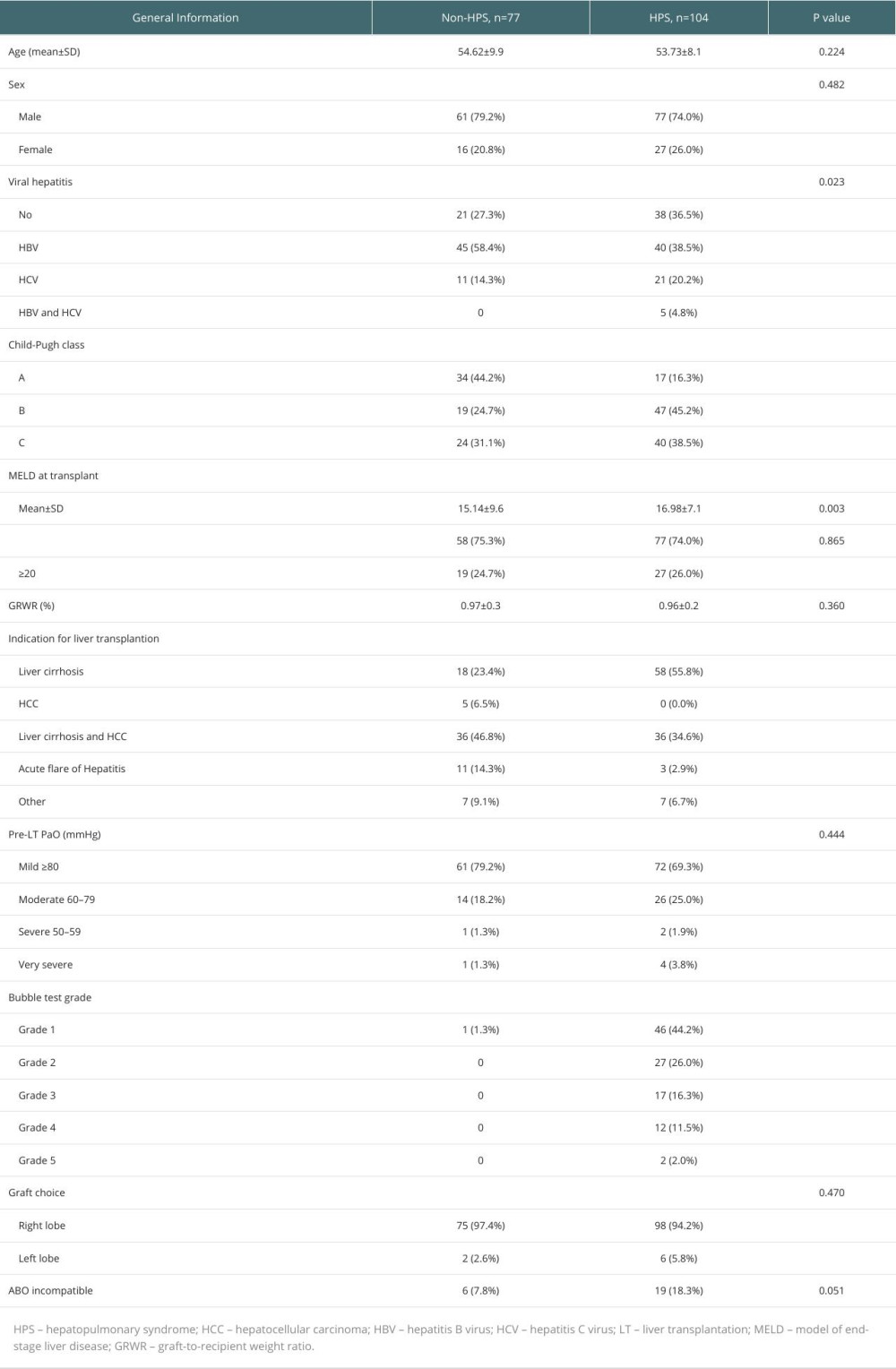 Table 1. Comparisons of baseline demographics of hepatopulmonary syndrome (HPS) group and non-HPS group.
Table 1. Comparisons of baseline demographics of hepatopulmonary syndrome (HPS) group and non-HPS group. Table 2. Comparisons of clinical characteristics and postoperative outcomes.Table 1. Comparisons of baseline demographics of hepatopulmonary syndrome (HPS) group and non-HPS group.Table 2. Comparisons of clinical characteristics and postoperative outcomes.
Table 2. Comparisons of clinical characteristics and postoperative outcomes.Table 1. Comparisons of baseline demographics of hepatopulmonary syndrome (HPS) group and non-HPS group.Table 2. Comparisons of clinical characteristics and postoperative outcomes. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988