06 November 2020: Original Paper
Outcomes of Living-Donor Kidney Transplantation in Female Recipients with Possible Pregnancy-Related Pre-Sensitization According to Donor Relationship
Jee Yeon Kim1BCDEF, Mun Chae Choi2BCD, Dong Hyun Kim1BCD, Youngmin Ko1BCD, Seong Jun Lim1B, Joo Hee Jung1B, Hyunwook Kwon1BCD, Young Hoon Kim1ABE, Sung Shin1ABCDEF*, Duck Jong Han1ABEDOI: 10.12659/AOT.925229
Ann Transplant 2020; 25:e925229






Abstract
BACKGROUND: Given that pregnancy is an immune-sensitizing event, female kidney transplant recipients who receive allografts from their offspring or husbands may have a higher risk of rejection and graft failure due to pre-sensitization acquired during pregnancy or childbirth. We investigated the association between donor relatedness (i.e., offspring, husband, unrelated) and graft survival among female living-donor kidney transplant (LDKT) recipients with pregnancy histories.
MATERIAL AND METHODS: From January 2009 to January 2018, a total of 2060 LDKTs were performed at Asan Medical Center, Seoul, Korea. After excluding HLA-incompatible transplantation, re-transplantation, and those without a clear history of childbirth, 390 female recipients were included and categorized into group I (offspring-to-mother, n=175), group II (husband-to-wife, n=159), and group III (unrelated, n=56). The primary endpoint was biopsy-proven acute rejection (BPAR) and graft survival. We also evaluated delayed graft function (DGF), death-censored graft failure, and mortality.
RESULTS: Group I had the lowest number of HLA mismatches (p<0.001), and group II had the highest number of ABO-incompatible transplantations (p=0.005). At 5 years after transplant, graft survival and death-censored graft survival did not significantly differ among the 3 groups (graft survival: 96.0% vs. 95.5% vs. 93.3%, p=0.685; death-censored graft survival: 98.3% vs. 97.5% vs. 100%, p=0.732). Five-year BPAR-free survival showed no significant differences among the 3 groups (88.6 vs. 88.7 vs. 88.6%, p=0.842). Group II had the highest rate of clinical rejection (p=0.103) and DGF (p=0.174), but the difference was not statistically significant.
CONCLUSIONS: Female LDKT recipients with possible pregnancy-related pre-sensitization who received grafts from offspring or husbands did not show significantly worse clinical outcomes than those who received grafts from unrelated donors.
Keywords: Allografts, Kidney Transplantation, Reproductive History, Tissue and Organ Procurement, Female, Graft Rejection, Graft Survival, HLA Antigens, Humans, Isoantibodies, Living Donors, Pregnancy, Republic of Korea
Background
Kidney transplantation confers a significant survival benefit in patients with end-stage renal disease [1]. However, the shortage of donors remains the major obstacle for kidney transplantation worldwide [2]. Living-donor kidney transplantation (LDKT) has significantly increased the size of the donor pool, and living donor provides the greatest opportunity for maximizing long-term survival of both patients and grafts [3–5]. Graft survival rates in kidney transplants from living-related and living-unrelated donors are equivalent regardless of other donor- and recipient-related factors, and are superior to the rates of deceased-donor transplants [6–8]. Living-related and living-unrelated kidney transplantation also have similar allograft survival rates.
However, the effect of donor-recipient relatedness in kidney transplantation in women with a history of childbirth and the possibility of pre-sensitization is unclear. Animal studies on maternal immune response to the fetus during pregnancies suggest that populations with an antigen-experience repertoire may have better long-term survival of grafts [9]. While multiple factors contribute to graft survival, HLA matching is a critical determinant of long-term graft outcome [10–12]. However, given that pregnancy is an immune-sensitizing event with specificity for spousal and offspring HLA, it is possible that women with a history of childbirth may have a higher risk of acute or chronic rejection and negative long-term outcomes [13]. However, there is no empirical evidence showing the long-term patient and allograft survival outcomes among female recipients of LDKT.
In this study, we evaluated the association between donor relatedness (i.e., offspring, husband, unrelated) and graft outcomes among female recipients with prior donor-specific alloimmunization during pregnancy in order to assess whether offspring-to-mother and husband-to-wife transplants are inferior to unrelated transplantation in terms of clinical outcomes in LDKT.
Material and Methods
STUDY POPULATION:
From January 2009 to January 2018, a total of 2680 patients underwent kidney transplantation at Asan Medical Center (Seoul, Korea), 2060 of whom underwent LDKT (Figure 1). Among a total of 864 female LDKT recipients, cross-match-positive transplants (n=24) and re-transplantation (n=49) recipients were excluded. There were 5 patients who received re-transplantation and showed a positive cross-match. Those without (n=37) or unknown (n=7) childbirth history were also excluded. Complement-dependent cytotoxicity cross-match and flow cytometry were evaluated prior to transplant. Cross-match-positive was defined by either positive complement-dependent cytotoxicity cross-match, positive flow cytometry, or both. Childbirth history was determined based on the nursing information in the medical records. Finally, 390 female recipients were selected for analysis and categorized into 3 groups: offspring-to-mother (Group I, n=175), husband-to-wife (Group II, n=159), and unrelated donors (Group III, n=56). Group III consisted of transplants from all living donors other than maternal-offspring or spousal relationships. This study received approval from the Institutional Review Board of Asan Medical Center (IRB number: 2014-0776). The clinical and research activities are reported in accordance with the Declaration of Istanbul on Organ Trafficking and Transplant Tourism. All living organ donations were approved by the Korean Network for Organ Sharing (KONOS) under the Organ Transplantation Act (OTA).
IMMUNOSUPPRESSANTS:
Basiliximab was mainly used as the induction regimen, while rabbit anti-thymocyte globulin (Thymoglobulin®, Genzyme, Cambridge, MA) was used in patients with immunological risk factors, including highly sensitized individuals and those with complications due to long-term use of steroids. The maintenance immunosuppressive regimen was a combination of calcineurin inhibitor (cyclosporine, tacrolimus), anti-metabolite (mycophenolic acid), and prednisolone.
In cases of ABO-incompatible kidney transplant, rituximab (200 mg) was used for desensitization 2 weeks before transplantation; the immunosuppression regimen was not different from that in ABO-compatible kidney transplants.
CLINICAL OUTCOMES:
We compared the rate of biopsy-proven acute rejection among the 3 groups. We assessed the rate of clinical rejection defined by clinical presentation and laboratory test results. We also assessed the
STATISTICAL ANALYSIS:
Continuous data were compared using one-way ANOVA, t test, or Mann-Whitney U-test according to the distribution of the variables. Results are presented as mean±SD. Categorical data were compared using the chi-squared test. Kaplan-Meier curves and log-rank tests were used to describe and compare the rates of graft survival and biopsy-proven acute rejection (BPAR)-free survival. Cox proportional hazards model analysis was performed to assess the outcomes of graft survival and acute rejection, using hazard ratios (HRs) and 95% confidence intervals (CIs). We selected variables that are known to have an important impact on the outcomes, including age, BMI, HLA, and ABO mismatch and pre-transplant DSA [14]. Adjusted variables with p<0.2 on univariate analyses were included as variables for multivariate analyses. Multiple imputation was used to address missing data.
All statistical analyses were performed with the SPSS Statistics for Windows, version 18.0 f (SPSS, Inc., Chicago, IL, USA) with a p value of <0.05 as the criteria for statistical significance.
Results
BASELINE CHARACTERISTICS OF DONORS AND RECIPIENTS:
Table 1 shows the baseline characteristics of the study population. Recipients in group I were significantly older (p<0.001) and had a higher body mass index (p<0.001) compared with the other groups. The mean duration of hemodialysis before kidney transplantation was significantly longer in group III compared with the other groups (p=0.032). The number of HLA ABDR mismatches (2.4±0.9 vs. 4.4±1.2 vs. 4.5±1.2, p<0.001) and HLA DR mismatches (0.8±0.4 vs. 1.6±1.2 vs. 1.4±0.6, p<0.001) were significantly lower in group I compared with the other groups. ABO-incompatible kidney transplant was more frequent in group II compared with the other groups (20.0% vs. 34.0% vs. 17.9%, p=0.005).
Donors in group I were significantly younger (29.5±7.5
PATIENT SURVIVAL AND DEATH-CENSORED GRAFT SURVIVAL:
There were 4 (2.3%), 3 (1.9%), and 3 (5.4%) cases of mortality in group I, group II, and group III, respectively (p=0.352). Causes of mortality were pneumonia (n=4), septic shock (n=3; acute cholangitis, small-bowel infarction, urinary tract infection), malignancy (n=1), suicide (n=1), and unknown (n=1). Group I and group II each had 1 case of death-censored graft failure while group III had none (p=0.709). At 5 years after transplant, graft survival and death-censored graft survival did not significantly differ among the 3 groups (graft survival: 96.0% vs. 95.5% vs. 93.3%, p=0.685; death-censored graft survival: 98.3% vs. 97.5% vs. 100%, p=0.732) (Figure 2). Univariate and multivariate Cox proportional hazards modeling showed that the relationship to the donor was not significantly associated with graft survival (Table 2) or death-censored graft survival (Table 3).
:
There was no significant difference in the rate of BPAR (9.2 vs. 11.3 vs. 10.7%, p=0.801), and 5-year BPAR-free survival showed no significant differences among the 3 groups (88.6 vs. 88.7 vs. 88.6%, p=0.842) (Figure 3). The clinical rejection rate was higher in group II (10.7%) compared with the other groups (4.6 and 7.1% in group I and III, respectively), but without statistical significance (p=0.103). DGF was highest in group II (6.9%), but there was no statistically significant difference (3.4 and 1.8% in group I and III, respectively, p=0.174). However, 9 (16.1%) patients in group III developed de novo DSA, which was a significantly higher rate compared with 5 (2.9%) in group I and 9 (5.7%) in group III (p=0.001). Univariate and multivariate Cox proportional hazard modeling showed that recipients with pre-transplant DSA had significantly higher BPAR [HR 2.10, 95% CI 1.06–4.15] (Table 4).
Discussion
Due to the shortage of organ donors, living donation from offspring and spouses remains an important source of organs for female transplant candidates [15]. However, it is unclear whether such related donors are the best option for women who may have developed immunologic responses to the donor HLA during exposure in pregnancy and childbirth, which can result in poor graft outcomes. We thus evaluated whether transplantation from offspring or spousal donors is comparable to that from unrelated donors in female recipients who underwent pregnancy and childbirth.
We first found that group I (offspring-to-mother) had fewer HLA mismatches and younger donors. However, the number of HLA mismatches and the age of donors were not found to be significantly associated to acute rejection or graft survival based on Cox proportional hazard modeling. It has been proposed that first-degree genetic relatives, especially offspring donors, represent an accessible pool of well-matched kidneys [15] due to the benefit of haplotype matching and young donor age. In 1977, Opelz and Terasaki speculated that pregnancy confers immunologic benefits to transplant recipients rather than acting as a source for sensitization and triggering either tolerance or enhancement [16]. Terasaki et al. also reported that there was no evidence of pre-occurring donor-specific immune sensitization of mothers who received transplants from their offspring [17]. On the other hand, Mahanty et al. reported that multiparous women had worse graft outcome irrespective of whether the donor was their offspring [18].
With the increase in the number of spousal donations, Pollack et al. and Bohmig et al. suggested that there is a possibility of accelerated rejection if the wife had been pregnant and exposed to her husband’s HLA [19,20]. It is controversial whether the spousal relationship significantly affects the graft outcome: some reports suggested that spousal donation, especially husband-to-wife donation, may be associated with better graft survival compared with other live-donor transplants [21,22], whereas other studies reported severe rejection following husband-to-wife kidney transplants [23]. Gjertson et al. showed that graft survival rates from husbands and wives were similar regardless of the number of past pregnancies [4]. A Korean study by Yoon et al. reported that 10-year survival rates and BPAR-free survival rates in spousal donor grafts were similar to those in unrelated grafts [2], and suggested that while the reason for the similar rate of graft survival is likely multifactorial, enhanced immunosuppression may play a key role.
In the present study, the 3 groups showed similar 5-year graft survival rates, ranging from 93.3% to 96.0% (p=0.685), and no significant difference in 5-year BPAR-free survival rate (p=0.842). These survival rates are comparable with the national data and the data from our single-center experience. Recent publication of our center 4000 kidney transplant experience showed a 5-year graft survival rate of 92.3% in living donor transplants [24], and Korean national data from Korean Organ Transplant Registry (KOTRY) reported a 3-year graft survival rate of 93.7% and 3-year acute rejection-free survival rate of 82.7% in the entire living-donor and deceased-donor kidney transplant population [25]. There are multiple hypotheses as to why rejections due to anamnestic reactions are not more frequently observed among women who receive transplants from their children or husbands. First, only about 50% to 65% of women with multiple pregnancies are exposed to fetal leukocytes [26,27], and not all who were exposed to fetal leukocytes become immunized. After years without re-exposure, women who do become immunized often lose their immunity [19,20]. Also, the cross-match eliminates recipients with persistent antibody responses against the donor [4,7], which may also apply to the present study, in which the participants with reactivity to their husband’s lymphocytes were excluded. Lastly, a modified immune response that benefits graft survival may develop in some women exposed to fetal leukocytes; however, as there is little data available on immune modification in this phenomenon, it is uncertain whether the specific mechanism is associated with tolerance, enhancement, microchimerism, or suppressor cells [23].
Concerning the scarcity of currently available information on the immune mechanisms of sensitization to fetal HLA, there is no agreement as to whether the rejections are caused by antibody-mediated, T cell activity, or both [23]. For searching the immunological causes of rejection, information from allograft pathology and the detection of circulating donor-specific antibody may be utilized. In our study, pre-transplant DSA was the only variable significantly associated with increased risk of biopsy-proven acute rejection. Also, the detection rate of
We investigated the outcomes of female recipients from living kidney donors in an individual transplant program with a vast amount of experience with offspring-to-mother and husband-to-wife transplants. Therefore, the principal strength of this study is that it was conducted under homogenous transplantation practice with a long duration of follow-up while substantially reducing variabilities in donor and recipient selection criteria and immunosuppression regimens. Also, the donor-specific antibody data provided further understanding of the possible immunologic responses that contributed to long-term graft outcomes in the 3 groups.
However, despite these strengths, this study also has notable limitations inherent to its retrospective nature. The pregnancy histories were retrospectively obtained through medical record review, so it is uncertain whether the husband donors were the biological fathers of the offspring. Although we suspect that such a discrepancy would be rare in our cohort, this can lead to different categorization of groups and is an unavoidable limitation of medical record data. Also, detailed obstetric data such as parity, course of pregnancy and transfusion history during delivery could not be sufficiently obtained to be included in the analyses. Future prospective studies that focus on the impact of pregnancy-related variables could provide further insight into pre-sensitization of female transplant recipients. Another limitation of our study is that the numbers of HLA mismatches and ABO-incompatible transplants were different among the 3 groups. However, these variables were not associated with graft survival or increased acute rejection in our analyses. Therefore, we cautiously conclude that offspring and spousal transplants can provide desirable long-term outcomes similar to those from unrelated donors, despite the possible pre-sensitization of donor HLA from pregnancy.
Conclusions
We report that recipients of offspring and spousal living donor transplants had mortality and graft survival rates similar to those of recipients of unrelated donor transplants. Offspring and spousal living-donor transplantation may be considered whenever feasible for female recipients with prior immunologic exposure through pregnancy.
Figures
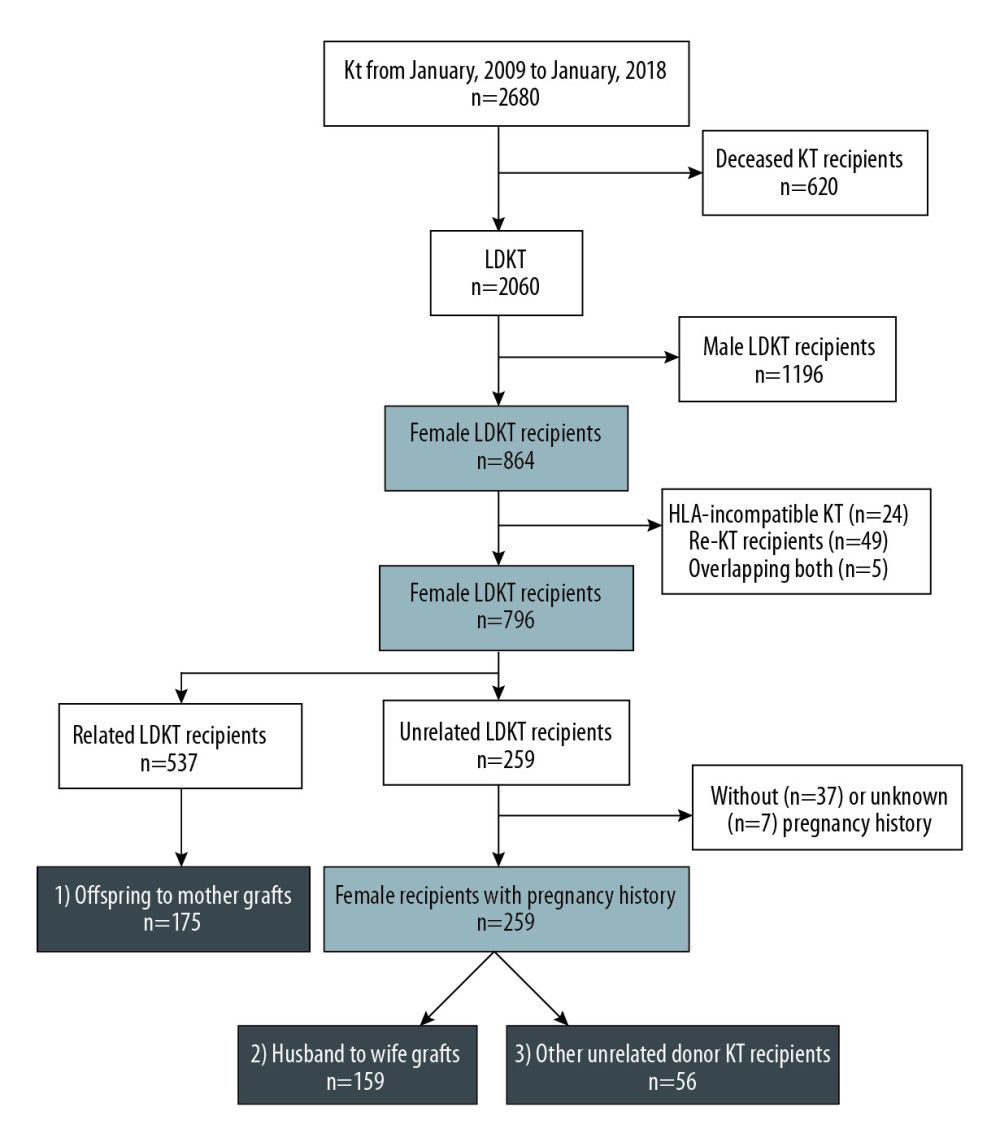 Figure 1. Flow diagram of the study.
Figure 1. Flow diagram of the study. 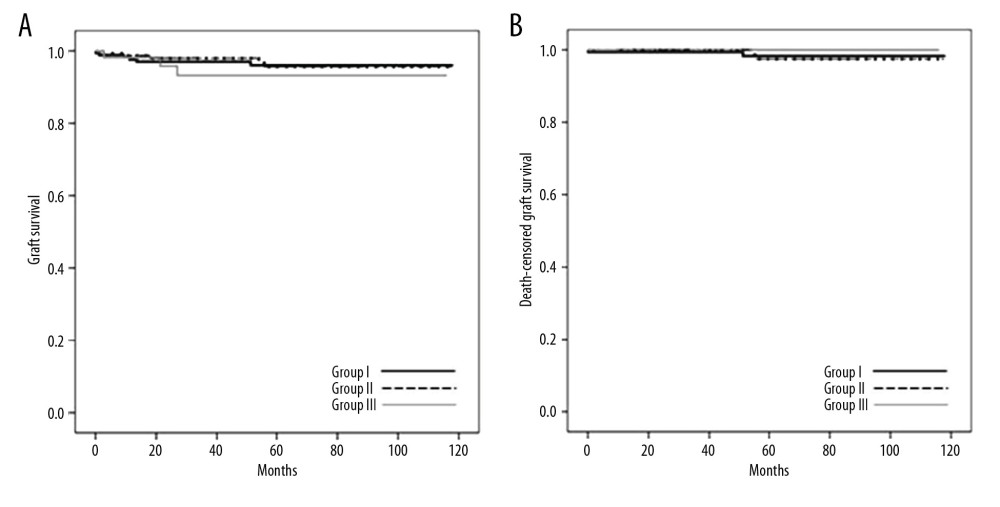 Figure 2. Rates of graft survival and death-censored graft survival at 5 years after transplant. (A) Graft survival rates (96.0% vs. 95.5% vs. 93.3%, p=0.685) and (B) death-censored graft survival rates (98.3% vs. 97.5% vs. 100%, p=0.732). Kaplan-Meier curves and log-rank tests were used to describe and compare the rates of graft survival.
Figure 2. Rates of graft survival and death-censored graft survival at 5 years after transplant. (A) Graft survival rates (96.0% vs. 95.5% vs. 93.3%, p=0.685) and (B) death-censored graft survival rates (98.3% vs. 97.5% vs. 100%, p=0.732). Kaplan-Meier curves and log-rank tests were used to describe and compare the rates of graft survival. 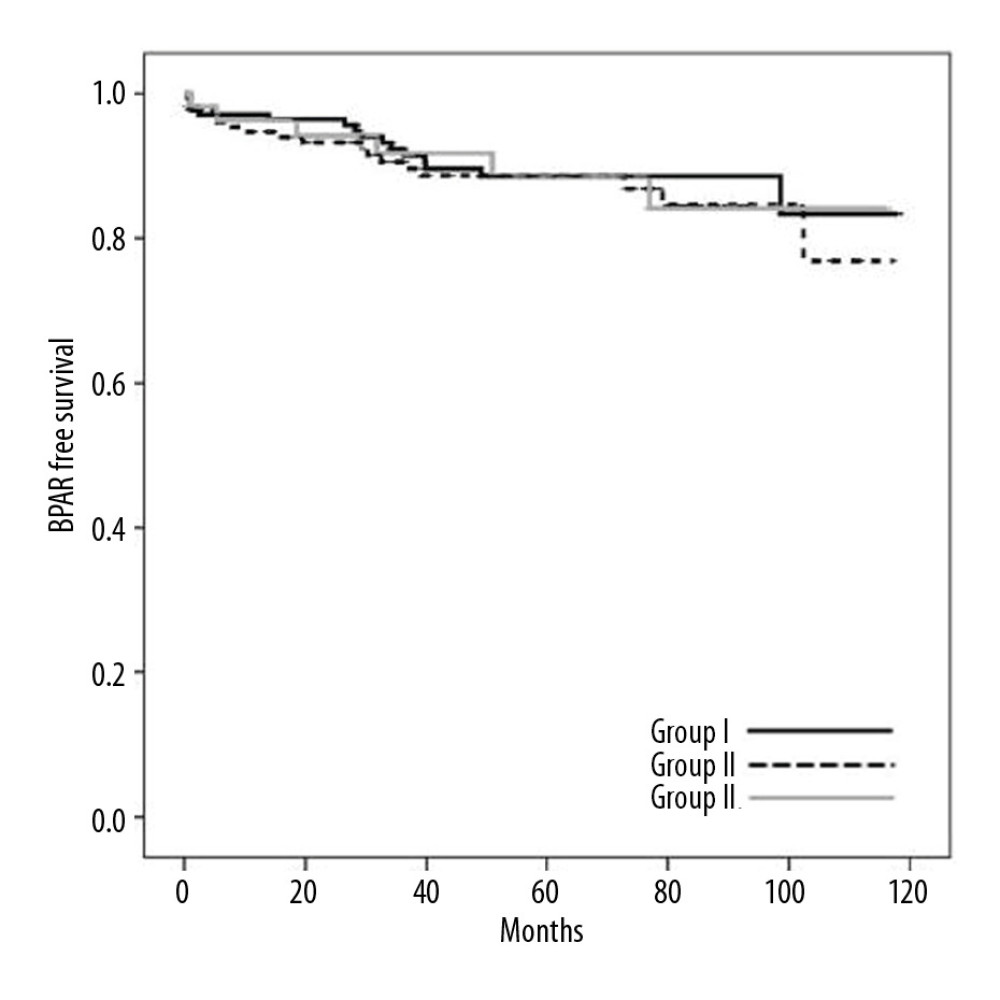 Figure 3. Five-year BPAR-free survival rates (88.6 vs. 88.7 vs. 88.6%, p=0.842). Kaplan-Meier curves and log-rank tests were used to describe and compare the biopsy-proven acute rejection (BPAR)-free survival.
Figure 3. Five-year BPAR-free survival rates (88.6 vs. 88.7 vs. 88.6%, p=0.842). Kaplan-Meier curves and log-rank tests were used to describe and compare the biopsy-proven acute rejection (BPAR)-free survival. References
1. Port FK, Wolfe RA, Mauger EA: JAMA, 1993; 270; 1339-43
2. Yoon HE, Song JC, Hyoung BJ, Comparison of long-term outcomes between spousal transplants and other living unrelated donor transplants: Single-center experience: Nephron Clin Pract, 2009; 113; c241-49
3. Kaneku HK, Terasaki PI, Thirty year trend in kidney transplants: UCLA and UNOS Renal Transplant Registry: Clin Transpl, 2006; 1-27
4. Gjertson DW, Cecka JM, Living unrelated donor kidney transplantation: Kidney Int, 2000; 58; 491-99
5. Velidedeoglu E, Tokyay R, Cuhadaroglu S, Haberal M, Living unrelated donor kidney transplantation: Transplant Proc, 1992; 24; 1894-95
6. Simforoosh N, Basiri A, Fattahi MR, Living unrelated versus living related kidney transplantation: 20 years’ experience with 2155 cases: Transplant Proc, 2006; 38; 422-25
7. Terasaki PI, Cecka JM, Gjertson DW, Takemoto S, High survival rates of kidney transplants from spousal and living unrelated donors: N Engl J Med, 1995; 333; 333-36
8. Voiculescu A, Ivens K, Hetzel GR, Kidney transplantation from related and unrelated living donors in a single German centre: Nephrol Dial Transplant, 2003; 18; 418-25
9. Barton BM, Xu R, Wherry EJ, Porrett PM, Pregnancy promotes tolerance to future offspring by programming selective dysfunction in long-lived maternal T cells: J Leukoc Biol, 2017; 101; 975-87
10. Susal C, Opelz G, Current role of human leukocyte antigen matching in kidney transplantation: Curr Opin Organ Transplant, 2013; 18; 438-44
11. Legendre C, Canaud G, Martinez F, Factors influencing long-term outcome after kidney transplantation: Transpl Int, 2014; 27; 19-27
12. Milner J, Melcher ML, Lee B, HLA Matching Trumps Donor Age: Donor-recipient pairing characteristics that impact long-term success in living donor kidney transplantation in the era of paired kidney exchange: Transplant Direct, 2016; 2; e85
13. Cohen JB, Owei L, Sawinski DL, Porrett PM, Inferior long-term allograft and patient outcomes among recipients of offspring living donor kidneys: Am J Transplant, 2018; 18; 1699-709
14. Shabir S, Halimi JM, Cherukuri A, Predicting 5-year risk of kidney transplant failure: A prediction instrument using data available at 1 year posttransplantation: Am J Kidney Dis, 2014; 63; 643-51
15. Bromberger B, Spragan D, Hashmi S, Pregnancy-induced sensitization promotes sex disparity in living donor kidney transplantation: J Am Soc Nephrol, 2017; 28; 3025-33
16. Opelz G, Terasaki PI, Studies on the strength of HLA antigens in related donor kidney transplants: Transplantation, 1977; 24; 106-11
17. Terasaki PI, Perdue S, Mickey MR, Sasaki N, Offspring to mother kidney transplants. An example of donor-specific immunized transplants: Transplantation, 1982; 33; 450-52
18. Mahanty HD, Cherikh WS, Chang GJ, Influence of pretransplant pregnancy on survival of renal allografts from living donors: Transplantation, 2001; 72; 228-32
19. Pollack MS, Trimarchi HM, Riley DJ, Shared cadaver donor-husband HLA class I mismatches as a risk factor for renal graft rejection in previously pregnant women: Hum Immunol, 1999; 60; 1150-55
20. Bohmig GA, Regele H, Saemann MD, Role of humoral immune reactions as target for antirejection therapy in recipients of a spousal-donor kidney graft: Am J Kidney Dis, 2000; 35; 667-73
21. Shames BD, D’Alessandro AM, Pirsch JD, Living-unrelated renal transplantation at the University of Wisconsin: Clin Transpl, 2001; 149-56
22. Terasaki PI, Cecka JM, Gjertson DW, Cho YW, Spousal and other living renal donor transplants: Clin Transpl, 1997; 269-84
23. Rosenberg JC, Jones B, Oh H, Accelerated rejection following offspring-to-mother and husband-to-wife transplants: Clin Transplant, 2004; 18; 729-33
24. Kwon H, Kim YH, Choi JY, Analysis of 4000 kidney transplantations in a single center: Across immunological barriers: Medicine (Baltimore), 2016; 95; e4249
25. Ahn C, Koo TY, Jeong JC, Initial report of the Korean Organ Transplant Registry: The first report of national kidney transplantation data: Transplant Proc, 2014; 46; 425-30
26. Burke J, Johansen K, The formation of HL-A antibodies in pregnancy. The antigenicity of aborted and term fetuses: J Obstet Gynaecol Br Commonw, 1974; 81; 222-28
27. Terasaki PI, Mickey MR, Yamazaki JN, Vredevoe D, Maternal-fetal incompatibility. I. Incidence of HL-A antibodies and possible association with congenital anomalies: Transplantation, 1970; 9; 538-43
Figures
Figure 1. Flow diagram of the study.Figure 2. Rates of graft survival and death-censored graft survival at 5 years after transplant. (A) Graft survival rates (96.0% vs. 95.5% vs. 93.3%, p=0.685) and (B) death-censored graft survival rates (98.3% vs. 97.5% vs. 100%, p=0.732). Kaplan-Meier curves and log-rank tests were used to describe and compare the rates of graft survival.Figure 3. Five-year BPAR-free survival rates (88.6 vs. 88.7 vs. 88.6%, p=0.842). Kaplan-Meier curves and log-rank tests were used to describe and compare the biopsy-proven acute rejection (BPAR)-free survival. Tables
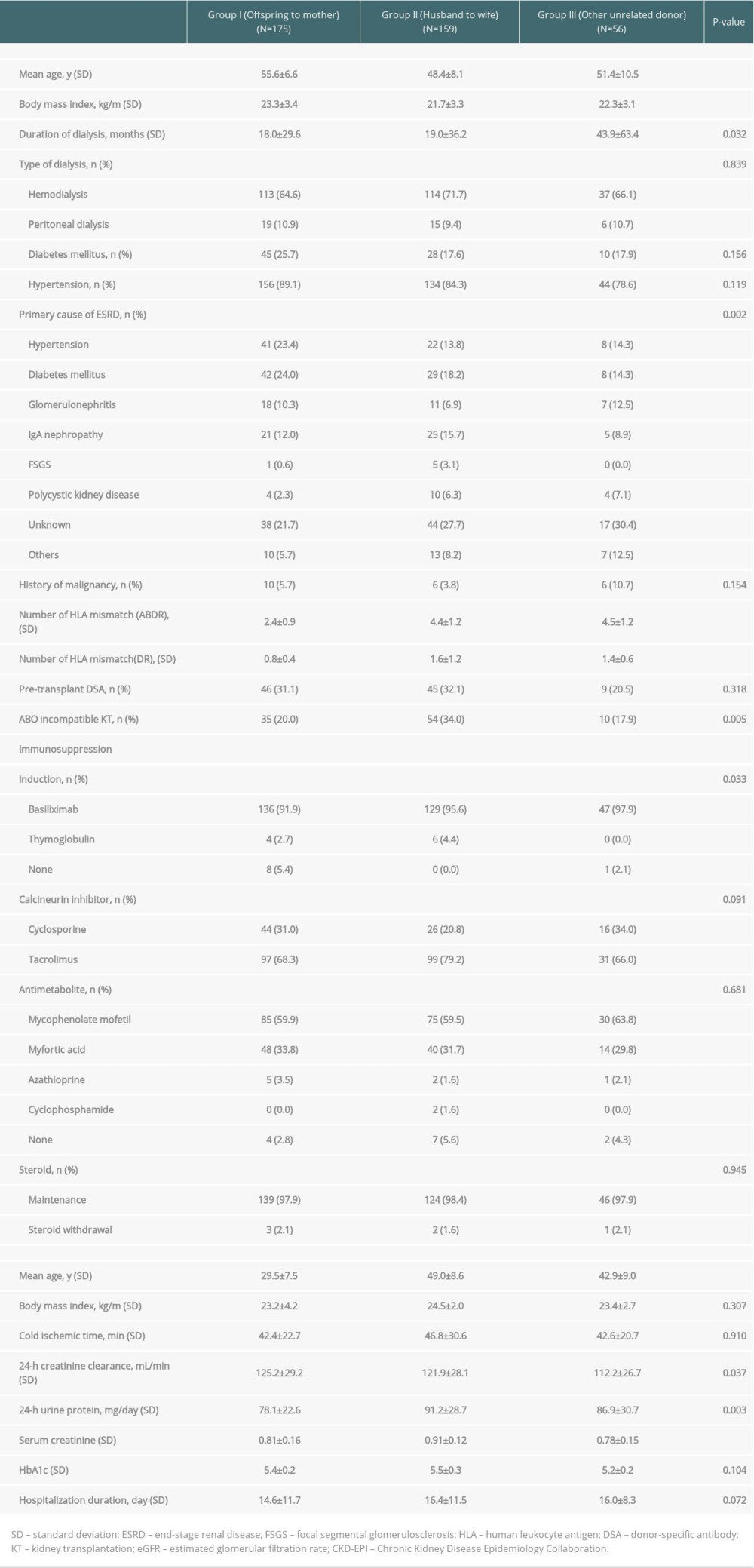 Table 1. Baseline characteristics.
Table 1. Baseline characteristics.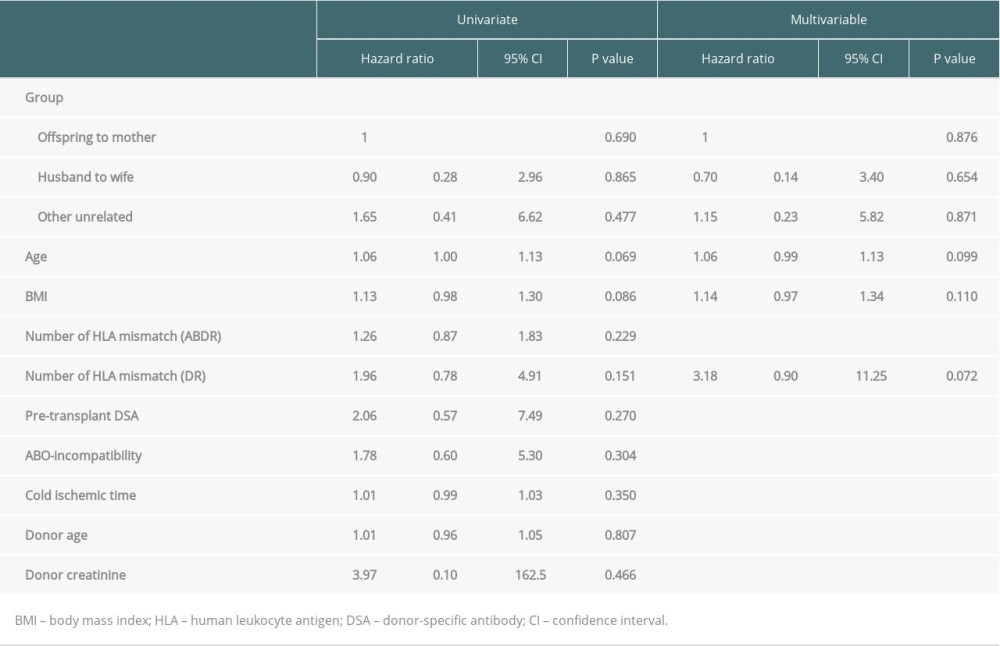 Table 2. Cox proportional hazards model analysis of graft survival.
Table 2. Cox proportional hazards model analysis of graft survival. Table 3. Cox proportional hazards model analysis of death-censored graft survival.
Table 3. Cox proportional hazards model analysis of death-censored graft survival.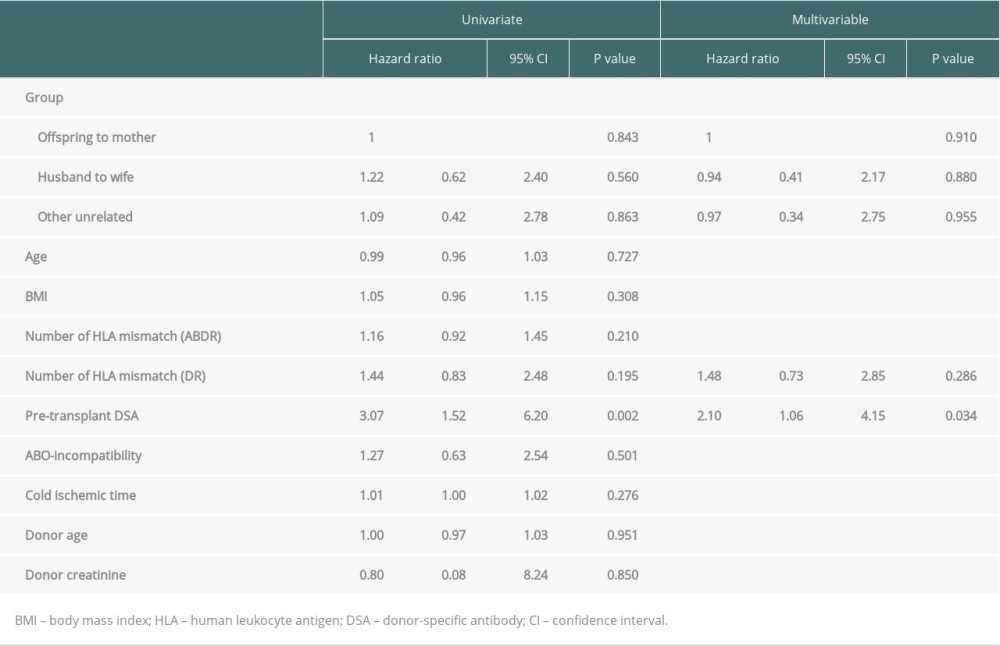 Table 4. Cox proportional hazards model analysis of biopsy-proven acute rejection.Table 1. Baseline characteristics.Table 2. Cox proportional hazards model analysis of graft survival.Table 3. Cox proportional hazards model analysis of death-censored graft survival.Table 4. Cox proportional hazards model analysis of biopsy-proven acute rejection.
Table 4. Cox proportional hazards model analysis of biopsy-proven acute rejection.Table 1. Baseline characteristics.Table 2. Cox proportional hazards model analysis of graft survival.Table 3. Cox proportional hazards model analysis of death-censored graft survival.Table 4. Cox proportional hazards model analysis of biopsy-proven acute rejection. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988