03 November 2020: Original Paper
Comorbidity Burden May Be Associated with Increased Mortality in Patients with Severe Acute Liver Injury Referred for Liver Transplantation
Lindsey Steiner-Temnykh1ABCDEF, Lara Dakhoul2ABCDEF, James Slaven3ACDE, Lauren Nephew2BCDEF, Kavish R. Patidar2BCDEF, Eric Orman2BCDEF, Archita P. Desai2BCDEF, Eduardo Vilar-Gomez2BCDEF, Chandrashekhar Kubal4BCDEF, Burcin Ekser4BCDEF, Naga Chalasani2ABCDEF, Marwan Ghabril2ABCDEF*DOI: 10.12659/AOT.926453
Ann Transplant 2020; 25:e926453






Abstract
BACKGROUND: Severe acute liver injury (S-ALI) can lead to acute liver and multisystem failure, with high mortality and need for liver transplantation (LT); however, the burden and impact of liver disease and comorbid conditions are unknown.
MATERIAL AND METHODS: We assessed liver disease and Charlson Comorbidity Index (CCI) in adults without cirrhosis evaluated for LT at our center for S-ALI between 2004 and 2017. The study endpoints were 30-day death or LT and 90-day mortality (with LT as a competing risk).
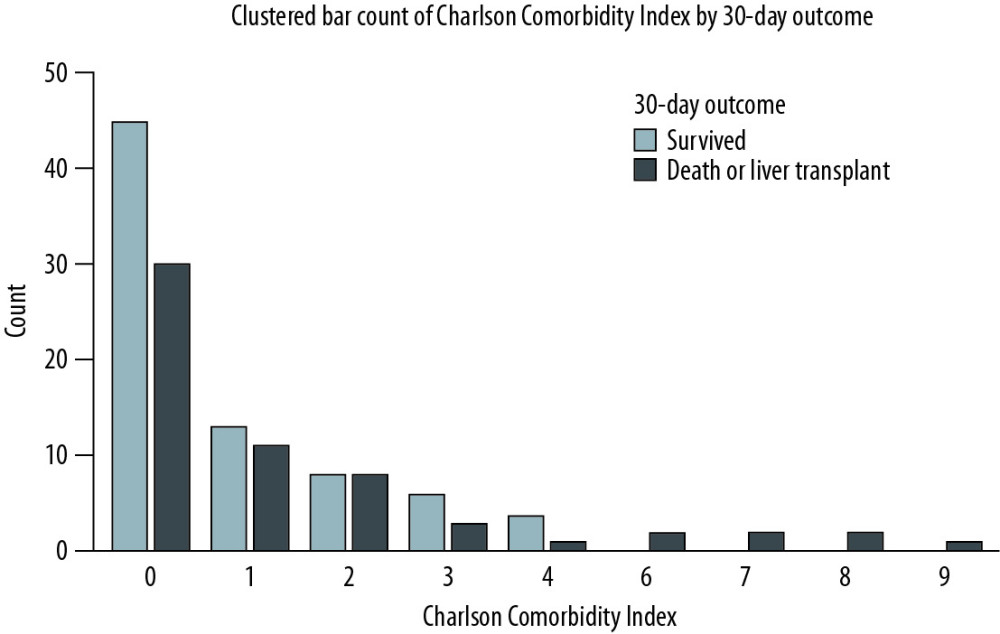
RESULTS: A total of 136 patients with S-ALI were included; 13% had underlying liver disease and a higher Model for End-stage Liver Disease score than those without liver disease. Sixty patients (41%) died or underwent LT within 30 days. They were older and more frequently female and had disease of autoimmune, viral, or indeterminate etiology. Transplant-free survival was associated with acetaminophen injury. The mean CCI was higher in patients with 30-day mortality or LT (1.5±2.4) vs. LT-free survivors (0.8±1.2), (P=0.03). Beyond severity of illness, CCI was associated with increased 90-day mortality (subhazard ratio 1.17, 95% confidence interval, 1.01–1.35) but not 30-day mortality or LT in the risk-adjusted analyses.
CONCLUSIONS: Comorbidity burden may be an important modifier of transplant-free survival in patients with S-ALI, but further studies are needed to validate these findings.
Keywords: Comorbidity, Liver Diseases, Liver Failure, Acute, End stage liver disease, Liver Transplantation, Severity of Illness Index, young adult
Background
Acute liver injury, when severe, can lead to acute liver failure (ALF) and multisystem failure with high short-term risk of mortality and need for liver transplantation (LT) [1–3]. Medical comorbidity is associated with increased mortality in acute and chronic medical conditions, such as acute coronary syndrome and congestive heart failure [4–6]. Beyond Model for End-stage Liver Disease (MELD), comorbidity burden is also independently associated with increased risk of 6-month mortality in patients with suspected drug-induced liver injury, highlighting an important interplay of severity of liver injury and comorbidity burden [7]. Patients with less severe liver injury but significant comorbidities had higher short-term mortality than patients with more severe liver injury but no or mild comorbidities [7]. These findings were also observed in the subset of patients with underlying liver disease in that study. Underlying liver disease was associated with more severe liver injury in a prospectively studied cohort of patients with drug-induced liver injury [8]. The impact of comorbidity burden and underlying liver disease (which contributes to comorbidity burden) on outcomes in other forms of acute liver injury are not well described, but they may be most pertinent in patients with severe acute liver injury (S-ALI) and may inform clinical management and prognostication. There is no universally accepted definition of S-ALI; however, Koch et al. [1] have described criteria to define S-ALI that were associated with death or need for LT in 23% of cases in their study. Therefore S-ALI appears to be clinically important, and understanding the factors that can impact outcomes in this context would be meaningful. We hoped to build on our prior observations that, in addition to the severity of liver injury, comorbidity burden affected 6-month mortality in patients with suspected drug-induced liver injury but in a broader context of patients with S-ALI and consideration of LT. Chronic liver disease is an integral component of comorbidity burden scores [9,10], but it can also predispose to more severe liver injury for a given insult with worse outcomes. While patients with underlying cirrhosis sustaining S-ALI with ALF are commonly captured and studied in acute-on-chronic liver failure (ACLF) literature with particularly poor outcomes [11,12], patients with mild liver disease are generally excluded from study of acute liver injury and ALF [1,13]. The aim of this study was to test the hypothesis that underlying liver disease and comorbidity burden may adversely affect short-term transplant-free survival in patients with S-ALI in the absence of underlying cirrhosis.
The management of the most severe forms of acute liver injury leading to ALF is predicated on early referral to centers with LT services. We examined this hypothesis in a cohort of patients hospitalized for S-ALI, with or without ALF, and who were consequently referred for LT.
Material and Methods
CHILDREN (AGE <18 YEARS) AND PATIENTS WITH PRIOR LT OR UNDERLYING CIRRHOSIS WERE EXCLUDED:
Demographic and clinical data were collected on admission and throughout hospitalization, including the etiology of liver injury and any documented contraindications for LT candidacy. The presence of underlying liver disease and cirrhosis was determined by review of clinical documentation and imaging data in all cases and by liver biopsy data when available [15]. Comorbidity burden was measured using the Charlson Comorbidity Index (CCI), a well-known and validated measure (Supplementary Table 1) [9]. The CCI is an aggregate of weighted scores for malignancy (solid and or hematologic), liver disease, diabetes mellitus, renal disease, atherosclerotic disease, congestive heart failure, rheumatologic disease, AIDS, peptic ulcer disease, and dementia. Underlying liver disease is an important component of CCI, but it could also directly contribute to worse outcomes of liver injury in the cohort. Consequently, we examined both CCI and underlying liver disease in the study cohort and in the analysis of study endpoints. The CCI was determined based on only pre-existing conditions and not acute illness in the context of S-ALI. The study endpoint included 30-day mortality or LT to reflect very short-term combined endpoints commonly examined in ALF literature, as well as 90-day mortality more inclusively, with LT as a competing risk.
Similar to our previous work, we assessed the severity of liver injury using MELD (7), which has also been shown to predict transplant-free survival in patients with ALF (16). King’s College Criteria (KCC) were determined in all cases as high or low risk, according to APAP and non-APAP etiology of liver injury [3]. We also examined organ failure scoring using the CANONIC study Chronic Liver Failure Sequential Organ Failure Assessment (CLIF-SOFA) score (12). The seminal CANONIC study described ACLF in 1343 hospitalized patients with cirrhosis and demonstrated increased short-term mortality [12]. In contrast, the Asia Pacific Association for the Study of the Liver does not require underlying cirrhosis to define ACLF in liver failure developing in patients with chronic liver disease [17,18]. In the current study, we defined ACLF as ALF developing in patients with underlying (noncirrhotic) liver disease and examined their outcomes.
In the descriptive analysis, 30-day transplant-free survivors were compared with patients who died or underwent LT within 30 days of S-ALI. We assessed the impact of underlying liver disease and CCI on outcomes using 2 complementary regression analyses, in which MELD was used as the primary measure of liver injury severity. Logistic regression was used to assess the predictors of 30-day mortality or LT. Since LT is lifesaving, this combined endpoint may attenuate the impact of underlying liver disease or CCI on mortality. To assess the risk of short-term mortality, a competing risk regression analysis was performed to assess the predictors of 90-day mortality, with LT being analyzed as a competing risk. As a means of sensitivity testing, we repeated these analyses by modeling underlying liver disease and CCI while adjusting separately for non-MELD prediction or severity of illness scores, including CLIF-SOFA, the recently described risk score by the Acute Liver Failure Study Group (ALFSG), and the KCC score as calculated at presentation [3,12,13]. The ALFSG risk score incorporates hepatic encephalopathy grade, etiology of liver failure, vasopressor use, and log transformations of bilirubin and INR on admission in predicting transplant-free survival in patients with ALF. Factor V levels were not available to analyze the factors of interest while adjusting for the Clichy Criteria (19). While the disease severity scores used in our analyses are described in patients with ALF, little is known about their performance in predicting short-term outcomes in patients with acute liver injury. We performed area under the receiver operator curve (AUROC) analyses of MELD, CLIF-SOFA, ALFSG, and KCC and 30-day mortality or LT in the study cohort and in the subset of patients developing ALF. All analyses were performed using Stata SE 14 (College Station, TX), and tests were 2-sided with a significance threshold of P<0.05.
Results
UNDERLYING LIVER DISEASE:
Patients with underlying liver disease had similar age (38±12
ALF developed in 17 (94%) of 18 patients with underlying liver disease, compared with 97 (82%) of 118 patients without liver disease (P=0.2). In other words, almost all patients with underlying liver disease, albeit nonadvanced, developed ACLF per the study definition. Hence the analysis of the impact of underlying liver disease in this cohort largely reflected the impact of ACLF as well. The underlying liver conditions that were more frequently observed in patients who died or underwent LT within 30 days included viral and autoimmune disease, which were more common in women. In contrast, the liver condition observed more frequently in 30-day transplant-free survivors was alcohol related (Table 2). In aggregate, these observations point to potential sex-based differences in relation to outcomes, predominantly related to favorable 30-day transplant-free survival with APAP-related injury and in men vs. women (81% vs. 53%; P=0.06). The respective outcomes were similar for men and women with non-APAP-related liver injury (25% vs. 32%, respectively).
COMORBIDITY CONDITIONS IN CCI:
The most common comorbid conditions contributing to CCI in the cohort included underlying liver disease (13%), diabetes mellitus (14%), peptic ulcer disease (12%), chronic obstructive pulmonary disease (11%), and solid tumors (6%). Of these, only solid tumors were significantly more frequent in patients who died or underwent LT within 30 days (Table 3).
LT EVALUATION AND OUTCOMES:
The clinical records were scrutinized for documented contraindications to LT, and these were compared in patient who died or underwent LT within 30 days vs. 30-day transplant-free survivors (Table 4). Although the number of contraindications were similar between the groups, the types of contraindications differed. Substance abuse and psychiatric disease were more frequent contraindications in 30-day survivors, whereas being too sick to undergo a transplant was a more frequent contraindication in those who died within 30 days. Outcomes of LT evaluation were examined for descriptive purposes. Among a small subset of 30-day survivors who were listed for LT, more than half improved without LT.
FACTORS ASSOCIATED WITH MORTALITY AND LT:
Twenty-one survivors had less than 30-day follow-up (mean age 30±13, median CCI 0 [interquartile range, 0, 0], 92% APAP-related S-ALI, mean follow-up 8±5 days). These patients were excluded from the logistic regression analysis of 30-day mortality or LT. However, they were included in the time to event (competing risk) analysis of mortality within 90 days.
We examined the association of clinical factors at presentation with 30-day combined endpoint of mortality or LT with simple and multiple logistic regression. The factors associated with increased risk on simple logistic regression included MELD score, while APAP-related liver injury was associated with reduced risk (Table 5). Factors not associated with the endpoint included underlying liver disease, race, and treatments of S-ALI or ALF (N-acetyl cysteine or steroids). The multiple logistic regression was controlled for age, sex, and APAP- vs. non-APAP-related liver injury. Severity of liver injury (MELD score) was associated with 30-day mortality or LT. The CCI was not associated with the endpoint on the risk-adjusted analysis. APAP-related liver injury was associated with reduced 30-day mortality or LT. The findings were similar with introduction of interaction terms between sex and APAP-related liver injury. A post hoc power analysis indicated that the sample size was only 35% powered to detect the observed differences in 30-day mortality or LT in patients with and without underlying liver disease.
We examined the association of baseline clinical factors at presentation with 90-day mortality, but with LT as a competing risk. Factors not associated with the 90-day mortality in the univariable analysis included age, race, underlying liver disease, and treatment for S-ALI or ALF. The factors associated with 90-day mortality in the risk-adjusted analysis included CCI and MELD score (Table 6). Sensitivity analyses were performed to assess the risk-adjusted associated of CCI with mortality in the competing risk regression using 30 day (subhazard ratio 1.2, 95% confidence interval [95% CI] 1.05–1.38; P=0.009), 180 day (subhazard ratio 1.2, 95% CI 1.05–1.38; P=0.009), or time unrestricted analyses (subhazard ratio 1.2, 95% CI 1.04–1.38; P=0.01). APAP-related liver injury was not associated with 90-day mortality, but the other findings were similar when we included interaction terms between sex and APAP-related liver injury.
Additional sensitivity analyses were performed to assess how different models of severity of liver injury or illness, beyond MELD, might influence the association of CCI or underlying liver disease with 30-day and 90-day outcomes (including CLIF-SOFA, ALFSG, and KCC in lieu of MELD-based modeling). The CCI was not associated with 30-day mortality or LT on multiple logistic regression analysis while adjusting for (i) CLIF-SOFA, (ii) the ALFSG risk score, or (iii) the KCC (Supplementary Table 3). However, the CCI was associated with 90-day mortality on the competing risk analysis (significantly or trend) while adjusting for (i) the CLIF-SOFA (subhazard ratio 1.13, 95% CI 0.97–1.31; P=0.10), (ii) the ALFSG risk score (subhazard ratio 1.19, 95% CI 1.03–1.037; P=0.014), or (iii) the KCC (subhazard ratio 1.15, 95% CI 0.99–1.3; P=0.054).
The regression analyses were repeated in the 114 patients who developed ALF (55 survived without LT, and 59 died or underwent LT within 30 days). The CCI was not associated with 30-day mortality or LT in models based on MELD, CLIF-SOFA, ALFSG, and KCC. However, CCI was associated with a trend for increased 90-day mortality in the competing risk model based on MELD and ALFSG scores, but not CLIF-SOFA or KCC (Supplementary Table 4).
The AUROCs (95% CI) for predicting 30-day mortality or LT in all patients (S-ALI with or without ALF) were MELD, 0.74 (0.65–0.84); CLIF-SOFA, 0.73 (95% CI 0.63–0.82); ALFSG, 0.69 (95% CI 0.58–0.79); and KCC, 0.57 (95% CI 0.5–0.66). The AUROCs (95% CI) for the same endpoint only in patients developing ALF were MELD, 0.72 (0.61–0.83); CLIF-SOFA, 0.69 (0.58–0.8); ALFSG, 0.65 (0.54–0.77); and KCC, 0.56 (0.46–0.65), respectively.
Discussion
LIMITATIONS:
We acknowledge a number of limitations of the study, including the small sample size, retrospective design, and lack of an accepted definition of S-ALI. Sample size specifically limited our ability to assess the impact of underlying liver disease on mortality and LT. These limitations were unavoidable, despite the high volume (1961) of primary liver transplants performed at our center during the study period. Since the study patients were referred to our center for LT, the actual start date of S-ALI could not be reliably determined, and using the admission date as the reference for 30-day outcomes could have affected the related analyses. However, we believe that these patients would have had a high priority for admission, and we suspect there would have been little if any delay in admission to the study center after referral. A referral bias for more severe cases of acute liver injury may also affect our cohorts’ characteristics and analysis results in the context of LT referral. We also did not have laboratory data such as Factor V to calculate additional ALF criteria scores [19]. Thirty-day follow-up was also missing for some patients who were discharged to home. The majority of those patients were young with CCI=0 and rapidly resolving APAP-related liver injury at the time of discharge, and they would have been expected to recover from S-ALI. They were included in the competing risk analysis of 90-day mortality. The use of the 30-day time point for mortality or LT missed 10% of overall events (occurring after 30 days). However, this time frame allowed the optimal balance of capturing the majority of patients with these endpoints while maintaining a critical sample size of evaluable patients with documented follow-up for the logistic regression analysis.
Conclusions
In summary, nonadvanced underlying liver disease and medical comorbidity burden are prevalent in patients with S-ALI referred for LT. Underlying liver disease is associated with more severe liver injury, while severity of injury and overall comorbidity burden are associated with decreased 90-day transplant-free survival. These findings warrant further investigation, and if validated, incorporating comorbidity scores could improve the accuracy of prognostic models available to patients and clinicians and guide earlier referral to LT centers in patients with S-ALI.
Tables
Table 1. A comparison of demographic and clinical characteristics of patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as mean±standard deviation or number (percentage).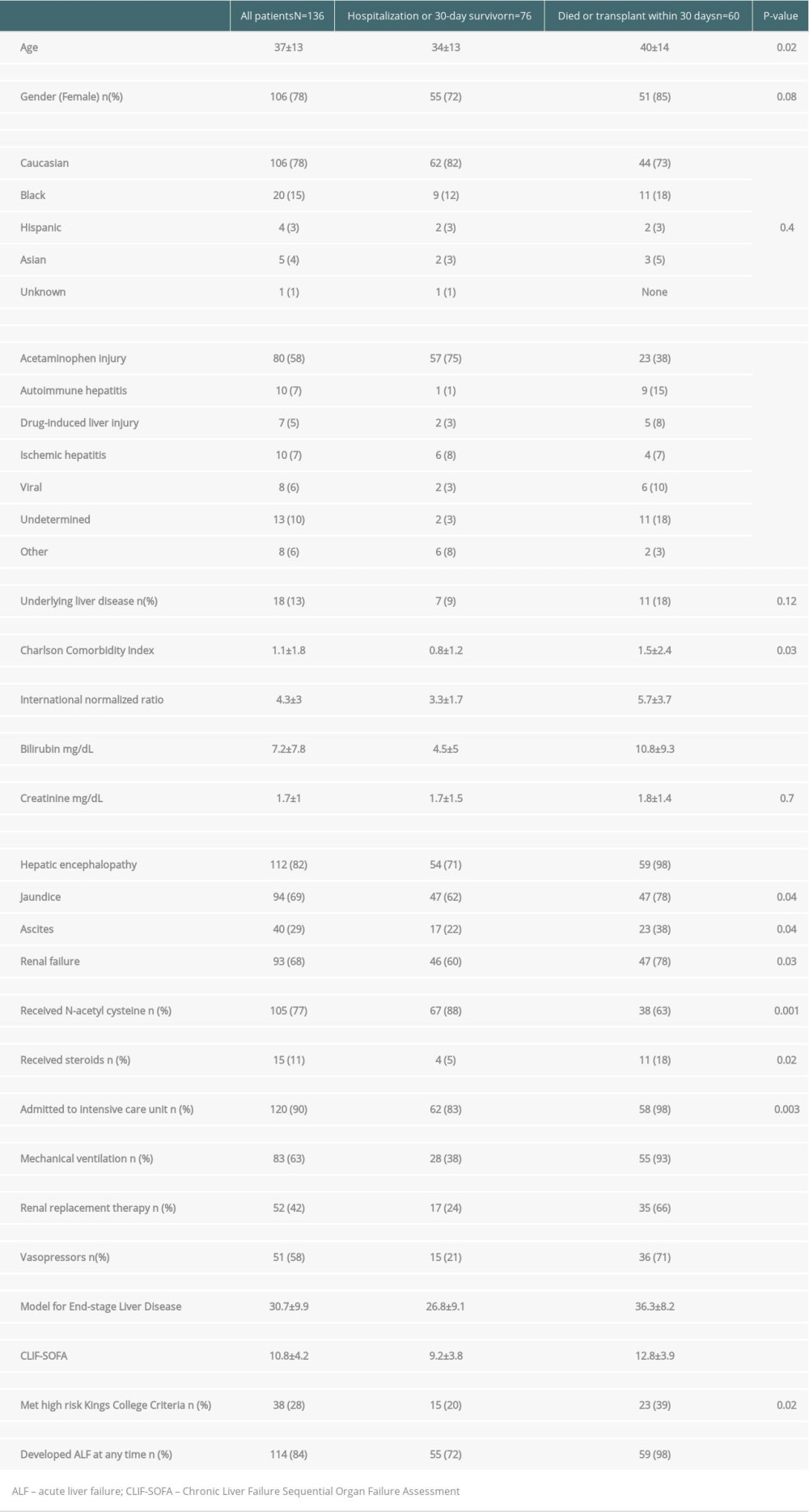 Table 2. Underlying liver disease in patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as number (percentage).
Table 2. Underlying liver disease in patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as number (percentage).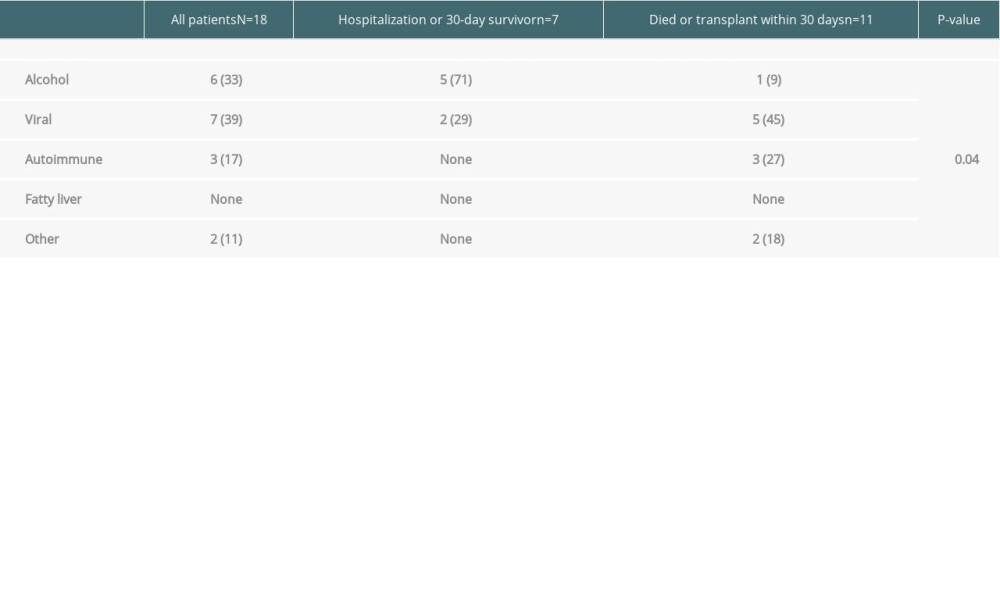 Table 3. A comparison of individual comorbidities in patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as number (percentage).
Table 3. A comparison of individual comorbidities in patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as number (percentage). Table 4. Evaluation and contraindications for liver transplant candidacy in patients surviving vs. dying or undergoing liver transplantation within 30 days after acute liver injury. Data are shown as number (percentage).
Table 4. Evaluation and contraindications for liver transplant candidacy in patients surviving vs. dying or undergoing liver transplantation within 30 days after acute liver injury. Data are shown as number (percentage).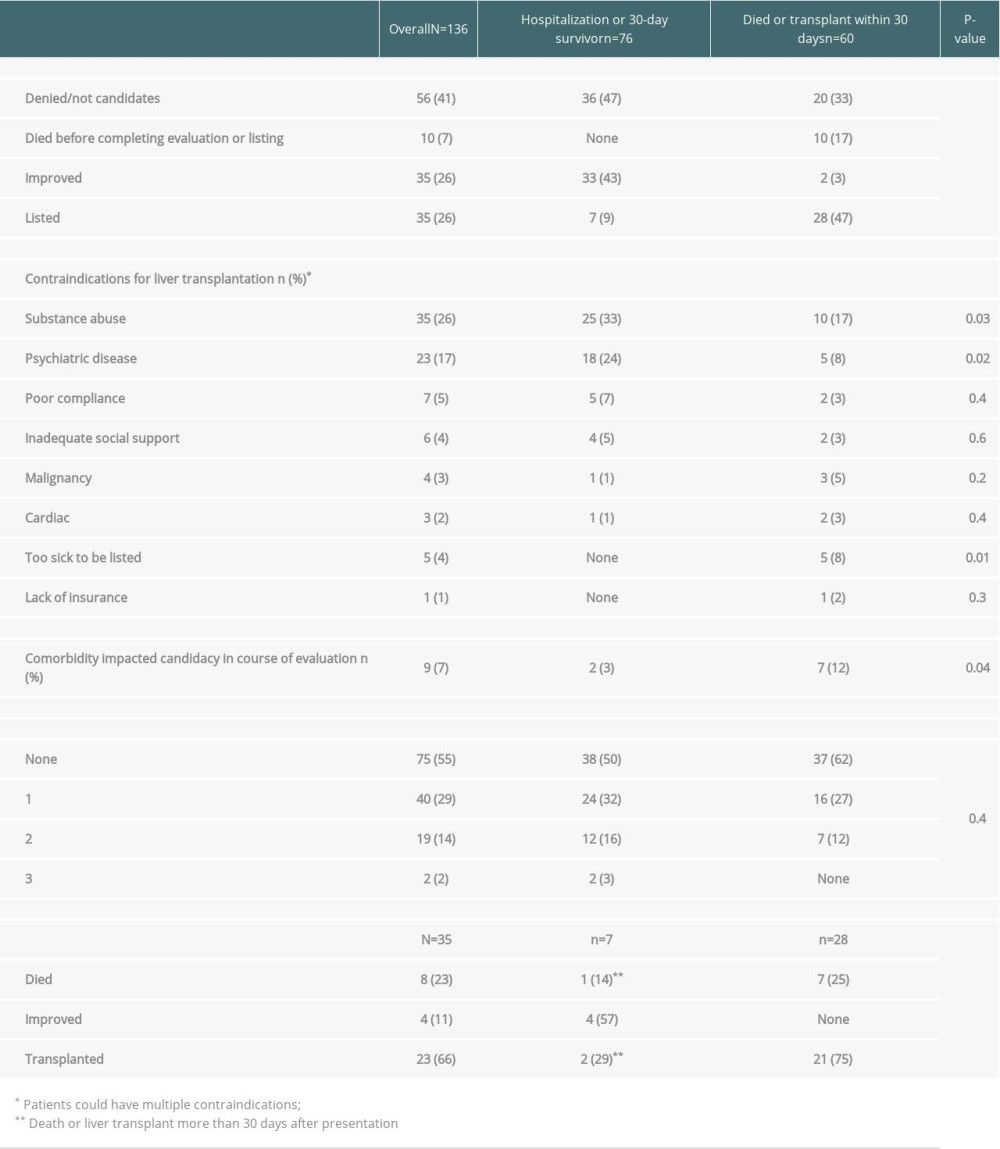 Table 5. The logistic regression analysis of predictors of 30-day mortality or liver transplantation in patients with severe acute liver injury referred for liver transplantation.
Table 5. The logistic regression analysis of predictors of 30-day mortality or liver transplantation in patients with severe acute liver injury referred for liver transplantation.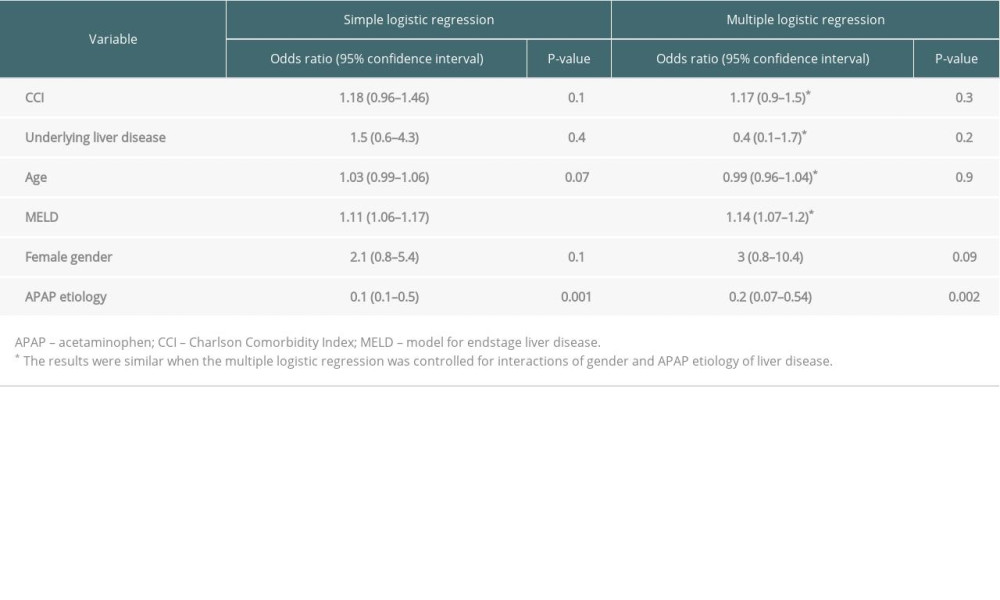 Table 6. The competing risk regression analysis of predictors of mortality within 90 days, with liver transplantation as a competing risk, in patients with severe acute liver injury referred for liver transplantation.
Table 6. The competing risk regression analysis of predictors of mortality within 90 days, with liver transplantation as a competing risk, in patients with severe acute liver injury referred for liver transplantation.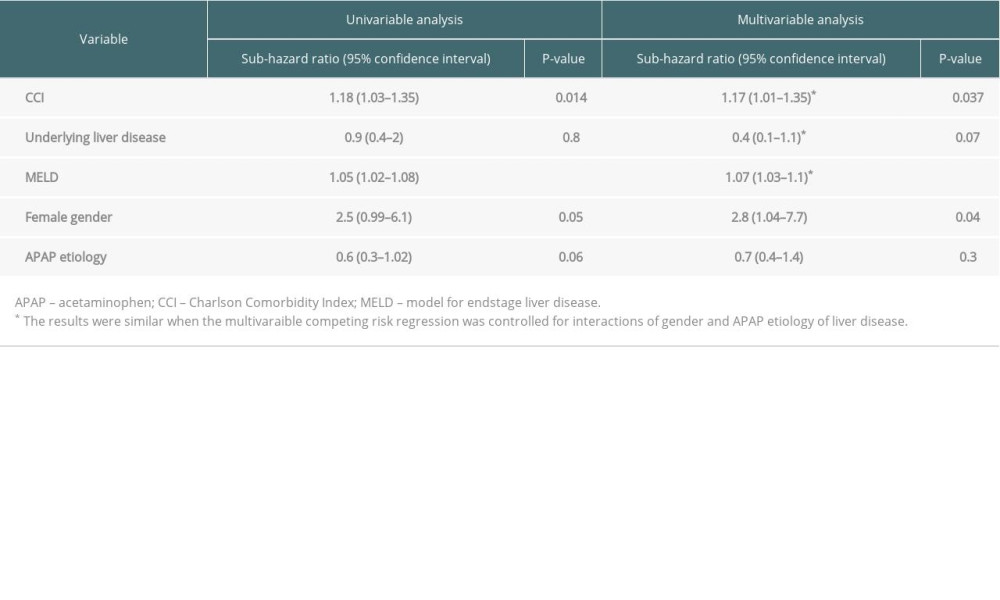 Supplementary Table 1. The conditions composing the Charlson Comorbidity Index as described by Charlson et al. [9].
Supplementary Table 1. The conditions composing the Charlson Comorbidity Index as described by Charlson et al. [9].![The conditions composing the Charlson Comorbidity Index as described by Charlson et al. [9].](https://jours.isi-science.com/imageXml.php?i=t7-anntransplant-25-e926453.jpg&idArt=926453&w=1000) Supplementary Table 2. A comparison of salient demographic and clinical characteristics of patients who survived, underwent liver transplantation, or died within 90 days of presenting with severe acute liver injury. Data are shown as mean±standard deviation or number (percentage).
Supplementary Table 2. A comparison of salient demographic and clinical characteristics of patients who survived, underwent liver transplantation, or died within 90 days of presenting with severe acute liver injury. Data are shown as mean±standard deviation or number (percentage).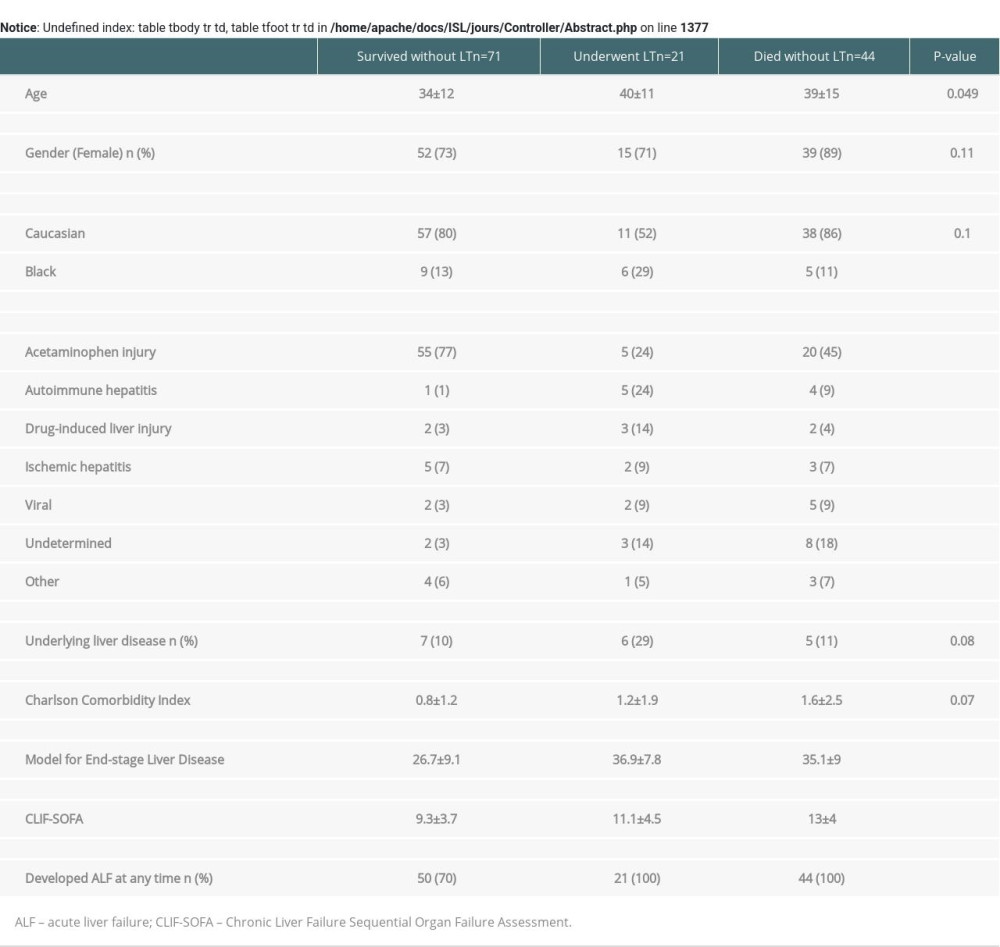 Supplementary Table 3. The association of the Charlson Comorbidity Index with 30-day mortality or liver transplantation by multiple logistic regression, and 90-day mortality by multivariable competing risk regression analyses when modeled with different severity of illness scores.
Supplementary Table 3. The association of the Charlson Comorbidity Index with 30-day mortality or liver transplantation by multiple logistic regression, and 90-day mortality by multivariable competing risk regression analyses when modeled with different severity of illness scores.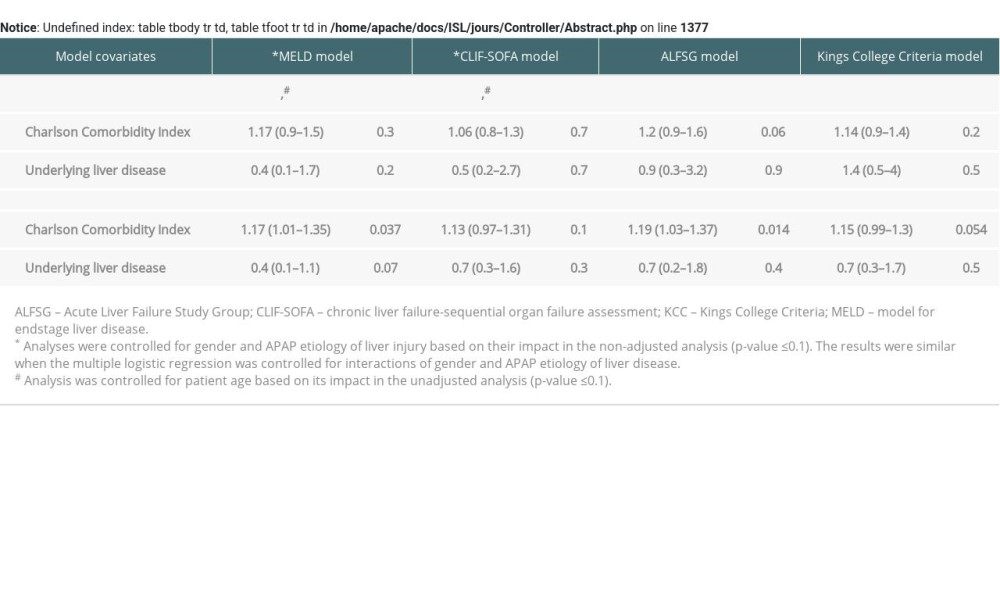 Supplementary Table 4. The association of the Charlson Comorbidity Index with 30-day mortality or liver transplantation by multiple logistic regression, and 90-day mortality by multivariable competing risk regression analyses when modeled in the 114 patients with acute liver failure with different severity of illness scores.
Supplementary Table 4. The association of the Charlson Comorbidity Index with 30-day mortality or liver transplantation by multiple logistic regression, and 90-day mortality by multivariable competing risk regression analyses when modeled in the 114 patients with acute liver failure with different severity of illness scores.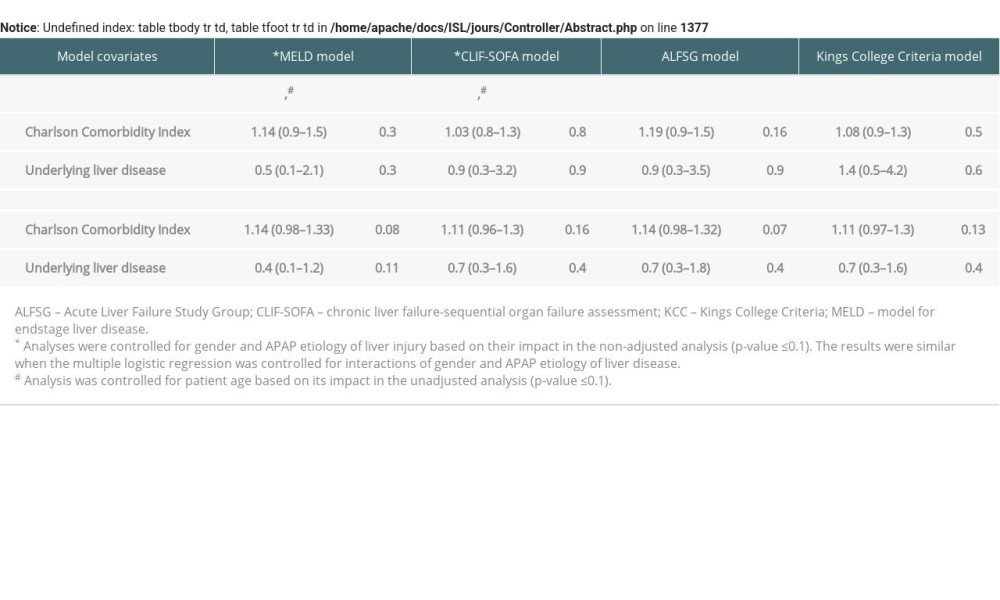
References
1. Koch DG, Speiser JL, Durkalski V, The natural history of severe acute liver injury: Am J Gastroenterol, 2017; 112(9); 1389-96
2. Lee WM, Squires RH, Nyberg SL, Acute liver failure: Summary of a workshop: Hepatology, 2008; 47(4); 1401-15
3. O’Grady JG, Alexander GJ, Hayllar KM, Williams R, Early indicators of prognosis in fulminant hepatic failure: Gastroenterology, 1989; 97(2); 439-45
4. Sanchis J, Soler M, Nunez J, Comorbidity assessment for mortality risk stratification in elderly patients with acute coronary syndrome: Eur J Intern Med, 2019; 62; 48-53
5. Sanchis J, Nunez J, Bodi V, Influence of comorbid conditions on one-year outcomes in non-ST-segment elevation acute coronary syndrome: Mayo Clin Proc, 2011; 86(4); 291-96
6. Lee DS, Austin PC, Rouleau JL, Predicting mortality among patients hospitalized for heart failure: Derivation and validation of a clinical model: JAMA, 2003; 290(19); 2581-87
7. Ghabril M, Gu J, Yoder L, Development and validation of model consisting of comorbidity burden to calculate risk of death within 6 months for patients with suspected drug-induced liver injury: Gastroenterology, 2019; 157(5); 1245-52.e3
8. Chalasani N, Bonkovsky HL, Fontana R, Features and outcomes of 899 patients with drug-induced liver injury: The DILIN prospective study: Gastroenterology, 2015; 148(7); 1340-52.e7
9. Charlson ME, Pompei P, Ales KL, MacKenzie CR, A new method of classifying prognostic comorbidity in longitudinal studies: development and validation: J Chronic Dis, 1987; 40(5); 373-83
10. Deyo RA, Cherkin DC, Ciol MA, Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases: J Clin Epidemiol, 1992; 45(6); 613-19
11. Arroyo V, Moreau R, Jalan RGinès P; EASL-CLIF Consortium CANONIC Study, Acute-on-chronic liver failure: A new syndrome that will re-classify cirrhosis: J Hepatol, 2015; 62(1 Suppl); S131-43
12. Moreau R, Jalan R, Gines P, Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis: Gastroenterology, 2013; 144(7); 1426-37
13. Koch DG, Tillman H, Durkalski V, Development of a model to predict transplant-free survival of patients with acute liver failure: Clin Gastroenterol Hepatol, 2016; 14(8); 1199-206.e2
14. Lee WM, Stravitz RT, Larson AM, Introduction to the revised American Association for the Study of Liver Diseases Position Paper on acute liver failure 2011: Hepatology, 2012; 55(3); 965-67
15. Mittal S, El-Serag HB, Sada YH, Hepatocellular carcinoma in the absence of cirrhosis in United States veterans is associated with nonalcoholic fatty liver disease: Clin Gastroenterol Hepatol, 2016; 14(1); 124-31.e1
16. McPhail MJ, Farne H, Senvar N, Ability of King’s College criteria and model for end-stage liver disease scores to predict mortality of patients with acute liver failure: A meta-analysis: Clin Gastroenterol Hepatol, 2016; 14(4); 516-25.e5 quiz e43–e45
17. Sarin SK, Kedarisetty CK, Abbas Z, Acute-on-chronic liver failure: Consensus recommendations of the Asian Pacific Association for the Study of the Liver (APASL) 2014: Hepatol Int, 2014; 8(4); 453-71
18. Hernaez R, Solà E, Moreau R, Ginès P, Acute-on-chronic liver failure: An update: Gut, 2017; 66(3); 541-53
19. Bernuau J, Goudeau A, Poynard T, Multivariate analysis of prognostic factors in fulminant hepatitis B: Hepatology, 1986; 6(4); 648-51
20. Rubin JB, Hameed B, Gottfried MAcute Liver Failure Study Group, Acetaminophen-induced acute liver failure is more common and more severe in women: Clin Gastroenterol Hepatol, 2018; 16(6); 936-46
21. Schiodt FV, Atillasoy E, Shakil AO, Etiology and outcome for 295 patients with acute liver failure in the United States: Liver Transpl Surg, 1999; 5(1); 29-34
22. Marudanayagam R, Shanmugam V, Gunson B, Aetiology and outcome of acute liver failure: HPB (Oxford), 2009; 11(5); 429-34
23. Reuben A, Tillman H, Fontana RJ, Outcomes in adults with acute liver failure between 1998 and 2013: An observational cohort study: Ann Intern Med, 2016; 164(11); 724-32
24. European Association for the Study of the Liver, Clinical practice guidelines panel, Wendon J, Panel Members Cordoba J, Dhawan A, Stolze Larsen F et al: EASL Clinical Practical Guidelines on the management of acute (fulminant) liver failure: J Hepatol, 2017; 66(5); 1047-81
25. Russo MW, Galanko JA, Shrestha R, Liver transplantation for acute liver failure from drug-induced liver injury in the United States: Liver Transpl, 2004; 10(8); 1018-23
Tables
Table 1. A comparison of demographic and clinical characteristics of patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as mean±standard deviation or number (percentage).Table 2. Underlying liver disease in patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as number (percentage).Table 3. A comparison of individual comorbidities in patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as number (percentage).Table 4. Evaluation and contraindications for liver transplant candidacy in patients surviving vs. dying or undergoing liver transplantation within 30 days after acute liver injury. Data are shown as number (percentage).Table 5. The logistic regression analysis of predictors of 30-day mortality or liver transplantation in patients with severe acute liver injury referred for liver transplantation.Table 6. The competing risk regression analysis of predictors of mortality within 90 days, with liver transplantation as a competing risk, in patients with severe acute liver injury referred for liver transplantation.Table 1. A comparison of demographic and clinical characteristics of patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as mean±standard deviation or number (percentage).Table 2. Underlying liver disease in patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as number (percentage).Table 3. A comparison of individual comorbidities in patients surviving hospitalization vs. dying or undergoing liver transplantation within 30 days of hospitalization for acute liver injury. Data are shown as number (percentage).Table 4. Evaluation and contraindications for liver transplant candidacy in patients surviving vs. dying or undergoing liver transplantation within 30 days after acute liver injury. Data are shown as number (percentage).Table 5. The logistic regression analysis of predictors of 30-day mortality or liver transplantation in patients with severe acute liver injury referred for liver transplantation.Table 6. The competing risk regression analysis of predictors of mortality within 90 days, with liver transplantation as a competing risk, in patients with severe acute liver injury referred for liver transplantation.Supplementary Table 1. The conditions composing the Charlson Comorbidity Index as described by Charlson et al. [9].Supplementary Table 2. A comparison of salient demographic and clinical characteristics of patients who survived, underwent liver transplantation, or died within 90 days of presenting with severe acute liver injury. Data are shown as mean±standard deviation or number (percentage).Supplementary Table 3. The association of the Charlson Comorbidity Index with 30-day mortality or liver transplantation by multiple logistic regression, and 90-day mortality by multivariable competing risk regression analyses when modeled with different severity of illness scores.Supplementary Table 4. The association of the Charlson Comorbidity Index with 30-day mortality or liver transplantation by multiple logistic regression, and 90-day mortality by multivariable competing risk regression analyses when modeled in the 114 patients with acute liver failure with different severity of illness scores. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988