16 January 2024: Original Paper
Immediate Impact of the COVID-19 Pandemic on Heart and Kidney Transplantation and the Recovery Trends in 30 Developed and Less-Developed Countries
Mohammad IslamDOI: 10.12659/AOT.942188
Ann Transplant 2024; 29:e942188






Abstract
BACKGROUND: The COVID-19 pandemic had multifaceted and disproportionate impacts on various countries. We investigated the decline of heart and kidney transplantation in 2020 and recovery trends in 2020, 2021, and 2022 in 30 developed and developing countries, considering COVID-19 incidence and mortality and pandemic-time economic variables.
MATERIAL AND METHODS: Data were obtained from reliable open databases. Nations were grouped by hierarchical cluster analysis into high-gross domestic product (GDP), mid-GDP, and low-GDP countries. Expected transplant numbers for 2020 to 2021 were estimated by the artificial neural network method using data from 2015 to 2019. Effect size and its inference were determined through the Hodges-Lemann estimate and Wilcoxon signed-rank test, respectively. The possible disproportionate effect was estimated by the Jonckheere-Tersptra test. Associations between transplantation and economic variables, COVID-19 caseload, and mortality were examined using Kendall rank correlation analysis.
RESULTS: All nations experienced a decline in 2020 and some real recovery in 2020 to 2022. For high-GDP countries, decline was insignificant and recovery was marginal; for mid-GDP countries, decline was significant for heart and deceased kidneys and recovery was modest; for low-GDP countries, decline was significant for heart, live kidneys, and deceased kidneys and recovery was marginal. The low-GDP countries were disproportionally negatively impacted, although the associations between the impact and economic variables, COVID-19 incidence, and COVID-19 mortality were statistically insignificant.
CONCLUSIONS: More inclusive studies of socioeconomic and cultural factors that affected the impact of the COVID-19 pandemic in different countries can be useful for better preparedness and reducing disruption in healthcare in future global pandemics.
Keywords: COVID-19, Heart Transplantation, Kidney Transplantation, Humans, COVID-19, Developing Countries, Pandemics
Background
The COVID-19 pandemic adversely impacted all aspects of human conditions, including transplantation medicine [1–3], in all nations. However, some nations [2–5] and some communities of certain nations [6,7] were disproportionately affected by COVID-19 incidence and COVID-19-related mortality. The COVID-19 pandemic might have negatively affected transplantation medicine in many ways, including a lack of organ procurement or lack of performing transplantation due to potential or actual COVID-19 infection of the donors and recipients, as well as indirect effects, such as shortages of skilled manpower, essential supplies, and hospital beds [8].
Donor organs can be grouped as vital organs, such as the heart, that only can be acquired from deceased donors, and expendable organs, such as a kidney, that a healthy person safely can donate. Live donor kidneys can be illegally traded in some countries [9,10]. Approximately 10% of the organs transplanted globally are illegally trafficked [11,12]. The COVID-19 pandemic has most drastically affected kidney transplantation [1,3]. Globally, kidney transplantation declined by 19% in 2020 [1], which can be ascribed to the effects of the COVID-19 pandemic on the transplantation of trafficked kidneys.
The impacts of the COVID-19 pandemic have extended into the realm of economics, as evident in the shifts in real gross domestic product (GDP) growth, inflation rate, unemployment rate, current account, and current government gross debt [13–17]. These economic downturns placed considerable pressure on healthcare systems [18,19], thereby diminishing the capacity of healthcare systems to adequately support transplantation programs.
While the effects of the COVID-19 pandemic on healthcare are multifaceted, in this study, we primarily focused on the immediate impact of the COVID-19 pandemic on transplantation of the heart, deceased donor kidney (DDK), and live donor kidney (LDK) in a selected group of developed countries where kidney trading is rare except in a few countries [20,21], as well as in some less-developed countries, including countries where illegal kidney trading had been repeatedly reported [20,22]. This study also examined the recovery in the rate of transplantation of these organs in 2020 through 2022, following the sharp decline in the earlier parts of 2020. In addition, we examined the association of COVID-19 impacts, namely COVID-19 incidence and mortality rates and the rate of heart and kidney transplantation. Finally, we examined the association of potential constraining factors, such as pandemic-time real GDP growth, inflation rate, unemployment rate, current account balance, current government gross debt, and transplantation rates. The broader goal of the study was to apply statistical tools to identify trends that could be helpful in policy dialogs aimed at reducing the disruptive impacts of future global pandemics.
Material and Methods
ETHICAL STATEMENT:
No ethical committee review was required because this is a secondary analysis of data obtained from publicly available databases.
DATA SOURCE:
Data on heart transplantation, DDK transplantation, and LDK transplantation for the years 2015 to 2022 were obtained from the Global Observatory on Donation and Transplantation [23]. For Hong Kong, the data were collected from the International Registry in Organ Donation and Transplantation database [24]. The data for the years 2021 and 2022 for Russia were unavailable in both data sources, so Russia was excluded in calculating recovery. Countries were selected based on (a) different levels of economic development, (b) where heart and kidney transplantation services are well-developed and reliable, and (c) where more complete data on heart, LDK, and DDK transplantation was available at the time of the study. A total of 30 countries were included in this study.
The population and per capita GDP data were obtained from the World Bank [25]. Since economic conditions can affect heart and kidney transplantation, and the COVID-19 pandemic affected the economic conditions [16–18], countries were grouped into high-GDP, mid-GDP, and low-GDP nations based on per-capita GDP using hierarchical cluster analysis, an unsupervised machine learning technique. Data on key economic variables such as real GDP growth, inflation rate, unemployment rate, current account balance, and current government gross debt were obtained from the World Bank Database [25].
STATISTICAL METHODS:
To assess the immediate impact of the COVID-19 pandemic on heart and kidney transplantation, we relied on historical transplantation records from 2015 to 2019. Our exploratory analyses indicated that the pattern of the number of transplants over that period was non-linear, thus the linear regression method was not appropriate for modeling the non-linear time series data. Therefore, the artificial neural network (ANN) method, which is equally effective in analyzing linear and nonlinear time series data [26,27], was used to model the time series data on transplants over the period from 2015 to 2019 to forecast the number of heart and kidney transplants in 2020 to 2022. Due to the lack of normality and the presence of outliers in the data, the median effect (rather than the mean effect) was calculated.
The median effect size was estimated using the Hodges-Lemann estimator [28,29], along with the 95% confidence interval (CI). The CI for the median size was constructed using the Wilcoxon signed-rank test [28,30]. The Wilcoxon signed-rank test (a nonparametric test) was used to determine whether the medians of the observed number of transplantations in 2020 and the counterfactual (ie, the predicted number of transplantations for the year 2020) were statistically different. The difference in medians reflected the effect of the COVID-19 pandemic on transplantation. The null hypothesis is that there is no effect of the COVID-19 pandemic against the alternative hypothesis that there exists an effect of the COVID-19 pandemic on heart and kidney transplants. A P value <0.05 is considered statistically significant. A negative median effect indicates a decline in transplantations due to the COVID-19 pandemic, a positive median effect reflects an increase in transplants due to the pandemic, and a zero median effect indicates no pandemic effect.
To examine if organ transplants in certain groups of countries were disproportionally affected by the COVID-19 pandemic, the Jonckheere-Tersptra non-parametric test [31,32] for the ordered alternative hypothesis was used. Kendall rank correlation [33] was used to assess the significance of the association between the number of transplants, economic variables, the number of COVID-19 cases, and COVID-19-related mortality.
To evaluate whether the countries were recovering from the 2020 decline in transplantations, data on heart and kidney transplants in 2021 and 2022 were also analyzed. Initially, we calculated the observed mean numbers of heart, DDK, LDK, and combined kidney transplants per million population for the period of 2015 to 2019 for high-GDP, mid-GDP, and low-GDP countries. Subsequently, the ANN model was applied to predict the expected organ transplantation rates for the years 2020 to 2022. We then estimated recovery or decline (change in percentage), assuming a continuation of the observed trends from 2015 to 2019 into the years 2020, 2021, and 2022. The percentage change was calculated using the formula ((O-E)/E)×100, where O and E are the observed and expected numbers of transplants, respectively. All calculations were computed using the Statistical Computing Software R 4.3.1 (
Results
HIERARCHICAL CLUSTERING OF THE COUNTRIES:
The hierarchical cluster analysis divided the 30 countries into 3 groups based on per-capita GDP (Figure 1). The high-GDP countries included 6 highly developed nations (Australia, Denmark, Norway, Sweden, Switzerland, and the United States); the mid-GDP countries included 12 developed nations (Belgium, Finland, France, Germany, Hong Kong, Israel, Italy, Japan, Kuwait, Slovenia, South Korea, and the United Kingdom). The low-GDP countries comprised 12 nations, including some less-developed nations (Argentina, Belarus, Brazil, Bulgaria, China, Croatia, Iran, Mexico, Pakistan, Romania, Russia, and Turkey).
IMMEDIATE (2020) IMPACT OF THE COVID-19 PANDEMIC:
The data on heart, DDK, LDK, and combined kidney transplantation normalized to per million population indicated that transplants of all 3 categories of organs dropped in 2020 in all countries compared to the previous 5 years, and recovered to some extent in 2021 and 2022 (Table 1). The low-GDP countries witnessed the sharpest decline (25–46%), while the mid-GDP and high-GDP countries experienced a relatively modest decline (6–14% and 1–19%, respectively) in all 3 categories of transplants in 2020 compared with 2019 (Table 1).
The COVID-19 pandemic effect size on the 3 groups of countries is shown in Figure 2. The median effect size (represented by the dark solid line in the middle of the box plot) for heart and LDK transplantation is positive (i.e., above 0) for the high-GDP countries but is increasingly negative for the mid-GDP and low-GDP countries, indicating a disproportionately negative effect in those 2 groups. The median effect size on DDK and combined kidney transplantation was negative for all 3 groups of countries but more pronouncedly negative in low-GDP countries than in high-GDP and mid-GDP countries (Figure 2), indicating an overall disproportionate negative effect on low-GDP countries.
MEDIAN EFFECT SIZE OF THE PANDEMIC IN 2020:
The median effect size of the COVID-19 pandemic on transplants in 2020, along with a 95% CI for median effect size and the P values are shown in Table 2. The COVID-19 pandemic had a negative median effect size on heart transplantation in mid-GDP and low-GDP countries. The effect was statistically significant for the mid-GDP countries (median effect size −0.58, 95% CI: −1.10 to −0.20; P=0.02). In contrast, the effect was substantial for the low-GDP countries but not statistically significant (median effect size −0.50, 95% CI: −2.54 to 1.61; P=0.06). The pandemic had a positive median effect on heart transplants in high-GDP countries (Table 2), although the effect was not statistically significant (median effect size 0.24, 95% CI −3.32 to 2.02, P=0.66).
The pandemic had a negative median effect size on LDK transplantation in both mid-GDP and low-GDP countries, but the effect was statistically significant only for low-GDP countries (median effect size −3.14, 95% CI: −6.14 to −0.42, P=0.00,). The pandemic had a positive median effect on LDK transplantation in high-GDP countries (Table 2), but the effect was not statistically significant (median effect size 0.32, 95% CI −3.12 to 2.66, P=0.72).
For DDK transplantation, the median effect size was negative in all 3 groups of countries. The effect was statistically significant for mid-GDP countries (median effect size −2.08, 95% CI: −6.07 to −0.95, P=0.00) and low-GDP countries (median effect size −4.72, 95% CI: −10.99 to −2.66, P=0.00), but not for high-GDP countries (Table 2).
The pandemic also had a negative median effect size on combined kidney transplants for all 3 groups of countries (Table 2). However, the effect was statistically significant only for low-GDP countries (median effect size −8.42, 95% CI: −12.09 to −3.45, P=0.00). Overall, the median effect size appeared to be more severe in low-GDP countries with a median effect size of −0.50 for heart transplants, −3.14 for LDK transplantation, −4.72 for DDK transplantation, and −8.42 for combined kidney transplantation (Table 2).
DISPROPORTIONAL IMPACT OF THE PANDEMIC ON 3 GROUPS OF COUNTRIES IN 2020:
The ordered alternative inferences for assessing the effect of the COVID-19 pandemic, denoted by θ1 θ2 θ3, and tested using the Jonckheere-Terpstra test, are shown in Table 3. The effect on heart transplantation was positive in high-GDP countries and negative in mid-GDP and low-GDP countries, but the trend of the effect was not statistically significant. For LDK transplantation, the effect was positive in high-GDP countries but negative in mid-GDP and low-GDP countries, and the trend was statistically significant (P=0.013). As for the DDK and combined kidney transplantation, the effect was negative in all 3 groups of countries, but the trend was statistically significant only for DDK transplantation (Table 3). Overall, the negative impact increased with the decline in GDP.
IMPACT OF PREEXISTING ECONOMIC FACTORS:
The relationship between various economic indicators and organ transplantation, as determined using the Kendall rank correlation method, is presented in Table 4. The table highlights the following trends: (a) a negative association between the inflation rate and transplantation, (b) a decrease in the number of LDK and combined kidney transplants in relation to the unemployment rate, and (c) an inverse relationship between the current account balance and DDK transplantation, suggesting that as the current account balance increases, the number of transplantations decreases (Table 4). However, none of the economic variables were found to have a statistically significant association with organ transplantation.
IMPACT OF COVID-19 INCIDENCE AND COVID-19-RELATED MORTALITY:
Table 5 shows the relationship between COVID-19 incidence (per million population), COVID-19-related mortality (per million population), and organ transplantation determined using the Kendall rank correlation method. It was observed that COVID-19 cases per million and LDK transplantation showed a negative association, while COVID-19-related mortality per million showed a negative association with heart transplantation, LDK transplantation, and combined kidney transplantation. However, none of the associations were statistically significant.
APPARENT CHANGES IN HEART AND KIDNEY TRANSPLANTS IN 2021 AND 2022:
Table 6 presents the year-to-year percentage changes in heart and kidney transplantation to highlight the changes in 2021 and 2022. For heart transplantation in 2021 (compared with that of 2020), the low-GDP countries witnessed a marginal recovery (from −25% to 3%), while a further decline was observed in mid-GDP countries (from −10% to −21%) and high-GDP countries (from −5 to −13%). In contrast, all 3 groups of countries showed some recovery in kidney transplantation in 2021 (Table 6). Low-GDP countries witnessed a substantial recovery (transplantation of DDK increased from −35% to 20%, that of LDK increased from −46% to 46%, and that of combined kidneys increased from −37% to 28% (Table 6). The recovery was modest for mid-GDP countries (transplantation of DDK increased from −7% to 9%, that of LDK increased from −6% to 11%, and combined kidneys increased from −14% to 13%), and marginal for high-GDP countries (transplantation of DDK increased from −4% to −1%, that of LDK increased from −19% to 3%, but that of combined kidneys decreased from −1% to −3%).
In 2022, compared with 2021, the trend of recovery was mostly negative (Table 6). Low-GDP countries experienced a decline in the transplantation of heart (from 3% to 0%), DDK (from 20% to 6%), LDK (from 46% to 21%), and combined kidneys (from 28% to 11%). In contrast, mid-GDP and high-GDP countries witnessed mixed outcomes. In mid-GDP countries, transplantation of hearts increased from −21% to 21%, but transplantation of kidneys decreased: that of DDK decreased from 9% to 2%, LDK decreased from 11% to −3%, and combined kidneys decreased from 13% to 0%. In high-GDP countries, transplantation of hearts increased from −13% to 5%, that of DDK increased from −1% to 4%, and combined kidneys increased from −3% to 1%, but transplantation of LDK declined from 3% to −7%.
REAL CHANGES IN HEART AND KIDNEY TRANSPLANTS IN 2021 AND 2022:
The actual (ie, observed) numbers of hearts and kidneys transplanted per million population and the expected number for the same as predicted by the ANN model (based on the numbers of organs transplanted in the years 2015 to 2019) and the net change in percentage are shown in Table 7. The data indicate that the high-GDP countries had no real decline in heart and DDK transplants in 2020 (the observed numbers of heart and DDK transplants were higher than the expected number by 33% and 9%, respectively). For this group, the trend continued in 2021 and 2022. However, the high-GDP countries had a slight decline in LDK and combined kidney transplants (−3% and −11%, respectively), and the trend essentially continued in 2021 and 2022.
The mid-GDP countries had a substantial decline in heart and LDK transplantation (−18% and −20%, respectively), and the trend essentially continued in 2021 and 2022. This group had a marginal decline in LDK and combined kidney transplants in 2020 (−5% and −8%, respectively), but the countries had a 5% to 9% recovery in LDK and combined kidney transplants in 2021 and 2022 (Table 7).
The low-GDP countries had the sharpest decline (32–47%) in all categories of transplants in 2020. This group of countries had no recovery in heart transplants in 2021 and 2022 (the observed numbers remained 32% to 33% below the expected numbers). This group had a marginal recovery in kidney transplants, but the number of kidneys transplanted had not reached the pre-pandemic level as of 2022.
Discussion
THE ANN MODEL AND ITS VALIDATION:
We used the ANN model for predicting the expected number of heart and kidney transplants in 2020 to 2022, using historical data from 2015 to 2019. Transplantation technologies and policies have been rapidly evolving and their adoption has been heterogenous among different regions of the globe [38]. We limited the collection of historical data to 2015 through 2019 to reduce the effect of such heterogeneity. This relatively small sample size of the time series may have compromised the accuracy and consistency of predictions on heart and kidney transplantation for 2020 to 2022 using the ANN model. To assess the effectiveness of the ANN model in predicting the outcomes with limited data, we constructed an ANN prediction model using data from 2015 to 2018 to forecast transplantation cases for 2019. We then compared the predicted outcomes with the actual cases of 2019. The ANN predictions closely matched the actual 2019 case number. We compared the actual and expected case numbers by calculating the root-mean-squared error (RMSE). As shown in Table 8, the RMSE values for each group of countries were below 2.67. Although RMSE is a relative indicator for the accuracy of forecasting, these reasonably low RMSE values indicated the effectiveness of the ANN prediction model [39]. Therefore, using the ANN model to predict the cases for 2020 to 2022 offered a higher level of confidence in studying the impact of the COVID-19 pandemic on transplantation. Since the ANN model is equally effective in analyzing linear and non-linear time series data [26], we considered our modeling to be robust, although we did not rule out the possibilities of some uncertainties and potential limitations of the method.
IMMEDIATE IMPACT OF THE COVID-19 PANDEMIC ON DIFFERENT GROUPS OF COUNTRIES:
Initial summary statistics (Table 1) indicate a decline in heart and kidney transplantations in high-GDP countries in 2020, but analysis of the data (Figure 2, Table 2) indicates that the COVID-19 pandemic had essentially no effect. For these nations, the median effect was positive for the heart and LDK transplantation and negative for DDK transplantation, but the effect was not statistically significant. The discrepancy between the findings of the initial summary statistics and the more detailed statistical analysis could be attributed to the small sample size (n=6). Regarding the mid-GDP countries, the median effect was negative and statistically significant for heart and DDK transplantation, and negative but statistically non-significant for LDK transplantation. For the low-GDP countries, the median effect was negative for all 3 categories of transplantation, and the effect was statistically significant for all categories (P<0.05) except for heart (P=0.06). The disproportionate effect of the COVID-19 pandemic on LDK and DDK transplantation in the low-GDP countries was confirmed by the Jonckheere-Terpstra test (P=0.013 and 0.038, respectively). Our analyses indicated that the negative impact increased with the decline in GDP.
Kute et al [3] reported a geographically defined disproportionate effect of the COVID-19 pandemic on the transplantation of many types of organs and concluded that “developing nations lagged behind, whereas developed nations have been able to recover their transplantation program during the pandemic.” The processes and policies that helped faster recovery of the developed nations warrant further studies.
A limitation of our study was grouping the countries based on GDP. While GDP has been shown to be associated with many socioeconomic parameters, including healthcare, life expectancy [40,41], and healthcare expenditure [42], GDP may not be an indicator of the general well-being of the citizens of a country [43]. In addition, GDP can be a dependent variable because factors such as infectious diseases [44], types of government, and social stability [45] can affect GDP.
THE PANDEMIC IMPACT AND ILLEGAL KIDNEY TRAFFICKING:
Since kidney transplantation experienced the most severe decline [1–3], and since the kidney is the most trafficked donor organ [46], it can be presumed that the COVID-19 pandemic disrupted organ trafficking. Trafficked and illegally traded organs are transplanted mostly in low-GDP and some mid-GDP countries, but the recipients are often transplantation tourists from high-GDP and mid-GDP countries [21,47–49]. Our study indicated that combined kidney transplants declined by 37% and LDK transplants declined by 46% in low-GDP countries. Given that trafficked organs constitute about 10% of all transplanted organs [11,12], we calculated the median effect on LDK transplantation after adding 10%, 15%, and 20% cases to the 2020 LDK transplants in low-GDP counties (data not shown). However, the median effect remained negative and statistically significant (P=0.00, 0.002, and 0.005, respectively) for the low-GDP countries. These data indicate that illegally traded kidneys may constitute more than 20% of the total number of kidneys transplanted in some countries, or the pandemic impact was more pervasive than a disruption in the demand-supply channel of illegal kidney trade. The pandemic impact was not limited to the disruption of the network of illegally traded kidneys because of restricted international and domestic travel [50] and the dislocation of potential donors and middlemen due to lockdown [35]; the pandemic also disrupted organ procurements and distribution [51] and overwhelmed the healthcare systems [34].
NO SIGNIFICANT IMMEDIATE IMPACT OF COVID-19 INCIDENCE OR MORTALITY:
High COVID-19 caseload and COVID-19-related morality could overwhelm the healthcare systems and organ transplantation. COVID-19 incidence and mortality rates in 2020 were higher in developed countries than in less developed countries [52,53]. Our analysis (Table 5) showed that COVID-19 incidence had a slight positive effect and COVID-19 mortality rates had a slight negative effect on heart and kidney transplantation, but the associations were not statistically significant. Aubert et al [1] reported that countries with low COVID-19 mortality rates had a sharper decline in organ transplantation, whereas countries with higher COVID-19 mortality rates had only a marginal decline in organ transplantation. These observations indicate that the contributors to the disproportionate impact of the pandemic on heart and kidney transplantation in different countries include factors beyond the healthcare infrastructures.
NO SIGNIFICANT IMMEDIATE IMPACT OF PANDEMIC-TIME ECONOMIC VARIABLES:
Our results show that some important economic variables, such as inflation rate and unemployment rate, negatively affected heart and kidney transplantation, but the effect was not statistically significant. The impact of the COVID-19 pandemic on the economies of different countries and communities has been studied extensively [13–17,54,55]. However, we observed a dearth of published works on the impact of pre-existing and pandemic-time economic conditions of different countries on the progression and manifestation of the COVID-19 pandemic. De and Price [56] examined the association between preexisting economic conditions and COVID-19 infections and mortality in New York City and observed a significant association between poor living conditions and COVID-19 infection and mortality.
THE 2021–2022 RECOVERY IN HEART AND KIDNEY TRANSPLANT:
Recovery from the sharp decline in 2020 started in 2020, as an umbrella of 22 transplantation societies across the globe published a consensus recommendation [57], and the American Society of Transplantation (AST) published recommendations indicating that the risk of transmission of SARS-CoV-2 from COVID-19-infected living or deceased donors (excepting the lung and intestine) is low [58]. Adoption of the recommendations might have accelerated recovery in the developed countries, but some less developed countries lagged behind [3]. We observed that the relative recovery of heart and kidney transplants in 2021 and 2022, considering the actual numbers of transplants in 2020 as the baseline, was higher in low-GDP countries than in mid-GDP and high-GHP countries (Table 1). Low-GDP countries had the sharpest decline in heart and kidney transplants in 2020, while the decline was modest in high-GDP and mid-GDP countries [2,3]; therefore, the relative recovery in the low-GDP countries appears dramatic. However, if the ANN model-predicted numbers of heart and kidney transplants in 2021 and 2022 are considered, the real recovery appears most robust in the high-GDP countries and the least robust in the low-GDP countries. This is another of the long list of ill effects of the COVID-19 pandemic on less-developed countries [59].
EPILOGUE AND LIMITATIONS OF OUR STUDY:
The aim of this study was to examine the immediate impacts of the COVID-19 pandemic on heart and kidney transplantation in 2020 in selected groups of countries. Our data indicate that the pandemic was associated with a reduction of heart and kidney transplants in all the countries examined, but the negative impact was more pronounced in the low-GDP countries than in high-GDP and mid-GDP countries. Moreover, low-GDP countries lagged in recovery in 2020 to 2022. We also examined if the pandemic-time economic variables were associated with the drastic decline in heart and kidney transplantation. Although the pandemic disproportionately and negatively affected the economic conditions of the less-developed countries than the developed countries [2,3,59], we found a lack of a significant correlation. Finally, we observed a lack of association between COVID-19 incidence rate, COVID-19-related mortality rate, and heart and kidney transplantation. These somewhat perplexing observations indicate the complexity of the factors that have affected the manifestation of the COVID-19 pandemic in general and pandemic-time healthcare, including organ transplantation, in particular.
The economic and healthcare policies of the countries, the overall healthcare infrastructures, management of the 2020 economic shutdown, and the development and adoption of effective policies are among the factors that have affected the outcomes [60,61]. Our team lacks experts on policy and social issues, but our study indicates the need for empirical research on these complex factors that may affect global healthcare during current and future pandemics. Researchers have predicted the inevitability of pandemics of the magnitude of the COVID-19 pandemic in the coming decades [62,63]. Chang et al [64] conducted one such pioneering study and identified 21 factors that affected morbidity and mortality in different countries during the COVID-19 pandemic. The aggravating factors include sex ratio, population density, urbanization, democratic form of government, political corruption, per capita GDP, and inequality in income and happiness. The mitigating factors include education, temperature, religious diversity, female leadership, the strength of the legal system, public trust in the government, experience, and healthcare infrastructures. The team also observed that technological advancement increases morbidity but reduces mortality. Further studies, especially on the strategies that allowed faster recovery in developed countries in 2020, routine and pandemic-time healthcare expenditure, international cooperation, technology transfer and proper implementation of the transferred technologies, and other resiliency measures, would benefit the healthcare system and transplantation medicine while confronting a pandemic.
In our study, we used advanced nonparametric statistical methods, including the Wilcoxon signed-rank test, ANN, and the Jonckheere-Tersptra test, to examine the impact of the COVID-19 pandemic on heart and kidney transplantation in 2020. We also employed the ANN model to examine the trends of recovery in heart and kidney transplantation in 2021 and 2022. The study had some potential flaws, including (a) clustering of the countries based on GDP alone, (b) small sample size for the countries selected, (c) 5 years of time series data used in forecasting, (d) some uncertainty of the ANN model for prediction (although we mathematically validated the model), and (e) not including the effect of the policies of the countries and many other social, cultural, and environmental factors that actually or potentially affected organ transplantation in a country during and after the COVID-19 pandemic.
Conclusions
The immediate impact of the COVID-19 pandemic on heart and kidney transplantation was disproportionately more negative and the 2020–2022 recovery was slower in less-developed countries than in developed countries. There was no significant association between the pandemic-time economic variables, COVID-19 incidence, and COVID-19 mortality and the negative impact on heart and kidney transplantation. More inclusive empirical analyses are needed to identify the aggravating and mitigating factors that shaped the outcomes of the pandemic.
Data Availability
The data that supported the findings are available from the corresponding author.
Figures
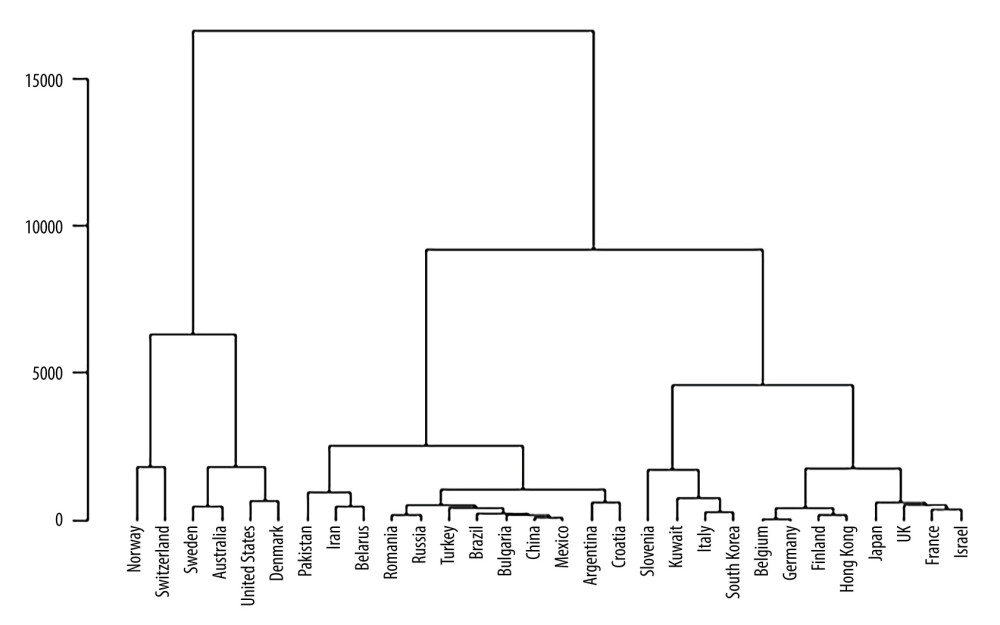 Figure 1. A dendrogram of the 30 countries, clustered based on gross domestic product (GDP). The Y-axis shows the distance between the clusters. The figure was created using Statistical Computing Software R 4.3.1 package ggplot2 (https://www.r-project.org/).
Figure 1. A dendrogram of the 30 countries, clustered based on gross domestic product (GDP). The Y-axis shows the distance between the clusters. The figure was created using Statistical Computing Software R 4.3.1 package ggplot2 (https://www.r-project.org/). 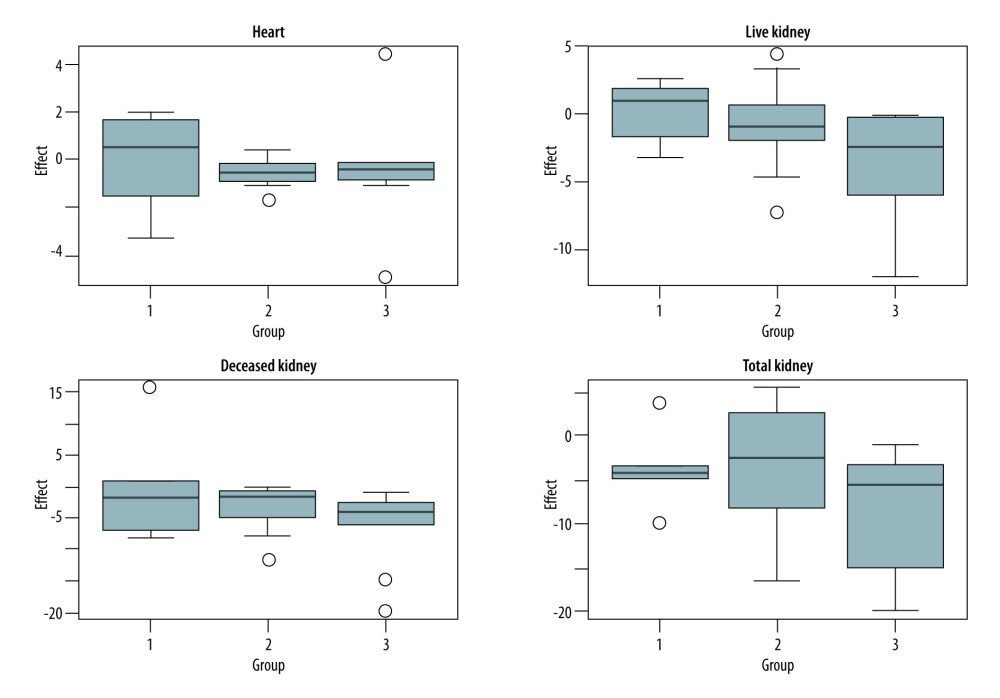 Figure 2. Side-by-side boxplots showing the median effect size of COVID-19 on heart and kidney transplantation in the 3 groups of countries. The dark solid line in the box indicates the median effect; the outlier detection lines and the outliers (the empty circles) are also shown. 1 – high- gross domestic product (GDP) nations; 2 – mid-GDP nations; 3 – low-GDP nations. The median effect is more pronounced for less-developed countries, as indicated by the shift of the median effect to <0. The figure was created using Statistical Computing Software R 4.3.1, package ggplot2 (https://www.r-project.org/).
Figure 2. Side-by-side boxplots showing the median effect size of COVID-19 on heart and kidney transplantation in the 3 groups of countries. The dark solid line in the box indicates the median effect; the outlier detection lines and the outliers (the empty circles) are also shown. 1 – high- gross domestic product (GDP) nations; 2 – mid-GDP nations; 3 – low-GDP nations. The median effect is more pronounced for less-developed countries, as indicated by the shift of the median effect to <0. The figure was created using Statistical Computing Software R 4.3.1, package ggplot2 (https://www.r-project.org/). Tables
Table 1. Year-to-year changes in heart, live donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation per million population over the years 2016 to 2020 in high-gross domestic product (GDP), mid-GDP, and low-GDP countries. The annual change is calculated based on the actual number of transplants performed in that year (Y2) and the previous year (Y1), using the formula ((Y2-Y1)/Y1)×100, thus, data for 2015 is not shown. Table 2. The median effect size per million population of the COVID-19 pandemic on heart and kidney transplantation by countries’ gross domestic product (GDP), along with 95% CI and P values for the null hypothesis of the median effect being zero are shown. A negative value for the median effect size indicates a negative effect and a positive value for the median effect size indicates a positive effect of the pandemic.
Table 2. The median effect size per million population of the COVID-19 pandemic on heart and kidney transplantation by countries’ gross domestic product (GDP), along with 95% CI and P values for the null hypothesis of the median effect being zero are shown. A negative value for the median effect size indicates a negative effect and a positive value for the median effect size indicates a positive effect of the pandemic. Table 3. Summary statistics of the impact size (per million population) of the COVID-19 pandemic on heart and kidney transplantation and P values for Jonckheere-Terpstra test θ1 θ2 θ3. Here, θ1, θ2, and θ3 represent the median effect for high-gross domestic product (GDP), mid-GDP, and low-GDP countries, respectively.
Table 3. Summary statistics of the impact size (per million population) of the COVID-19 pandemic on heart and kidney transplantation and P values for Jonckheere-Terpstra test θ1 θ2 θ3. Here, θ1, θ2, and θ3 represent the median effect for high-gross domestic product (GDP), mid-GDP, and low-GDP countries, respectively.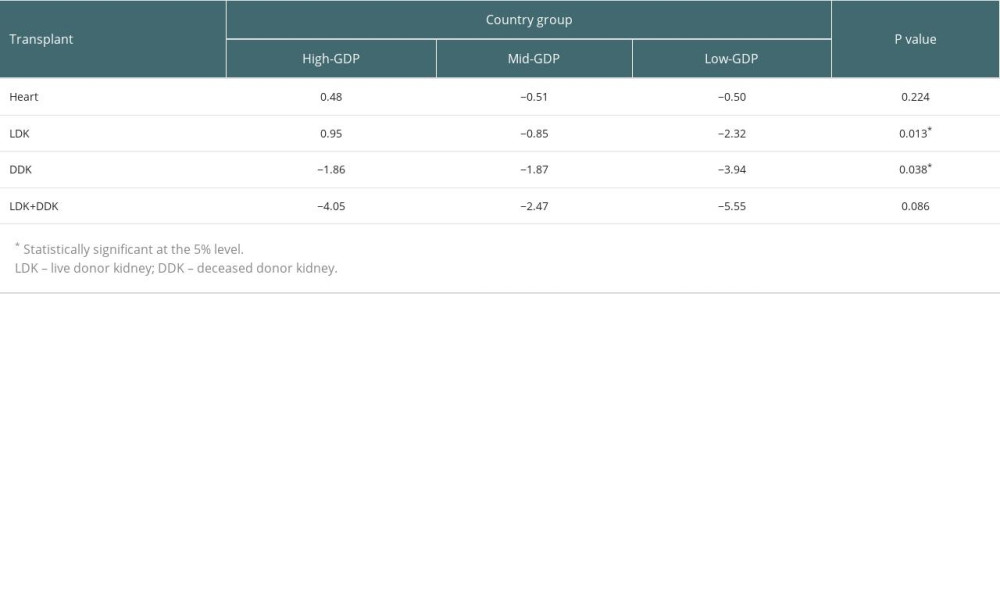 Table 4. Kendall Tau association between economic variables and numbers of heart and kidney transplants. The high P values (shown in parentheses) indicate a lack of a significant association between economic indicators and heart and kidney transplantation.
Table 4. Kendall Tau association between economic variables and numbers of heart and kidney transplants. The high P values (shown in parentheses) indicate a lack of a significant association between economic indicators and heart and kidney transplantation.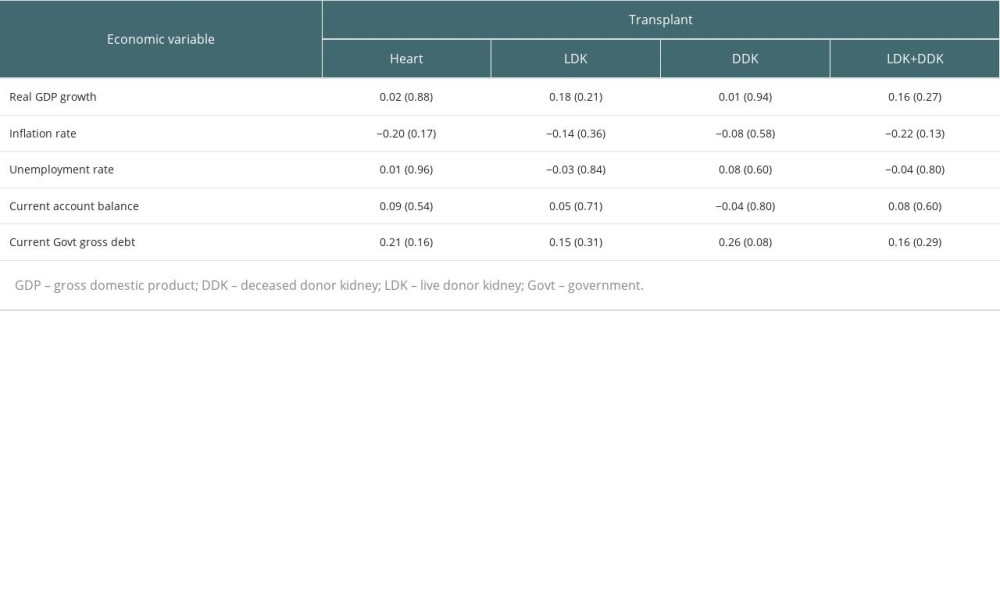 Table 5. Kendall Tau association between COVID-19 incidence, COVID-19 mortality, and the numbers of heart and kidney transplants. The high P values (shown in parentheses) indicate a lack of a significant association between COVID-19 incidence and COVID-19-related morality and heart and kidney transplantation.
Table 5. Kendall Tau association between COVID-19 incidence, COVID-19 mortality, and the numbers of heart and kidney transplants. The high P values (shown in parentheses) indicate a lack of a significant association between COVID-19 incidence and COVID-19-related morality and heart and kidney transplantation.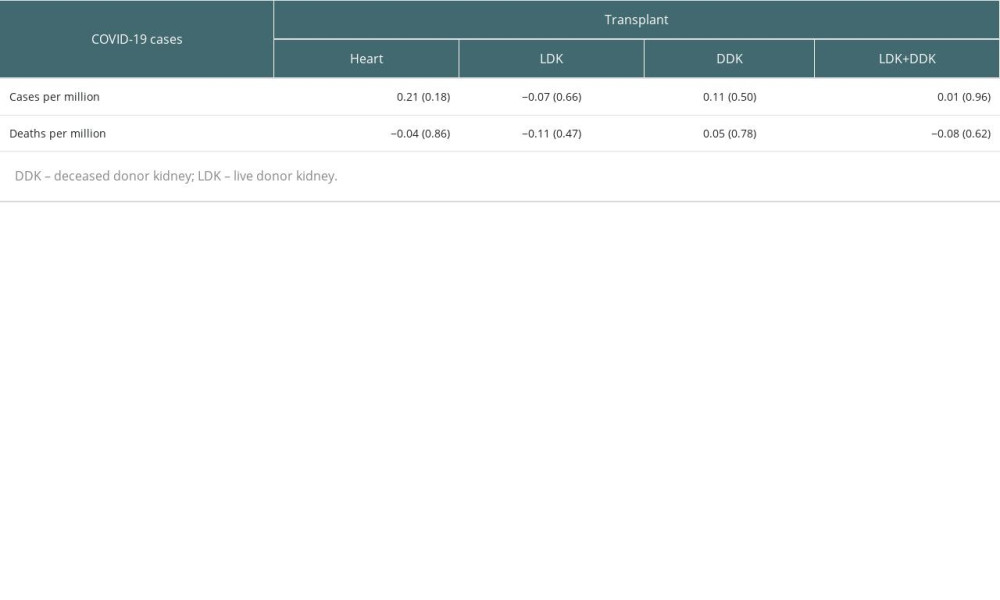 Table 6. Year-to-year changes in heart, living donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation per million population over the years 2020, 2021, and 2022 in high-gross domestic product (GDP), mid-GDP, and low-GDP countries. The annual change is calculated based on the actual number of transplants performed in that year (Y2) and the previous year (Y1), using the formula ((Y2-Y1)/Y1))×100.
Table 6. Year-to-year changes in heart, living donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation per million population over the years 2020, 2021, and 2022 in high-gross domestic product (GDP), mid-GDP, and low-GDP countries. The annual change is calculated based on the actual number of transplants performed in that year (Y2) and the previous year (Y1), using the formula ((Y2-Y1)/Y1))×100.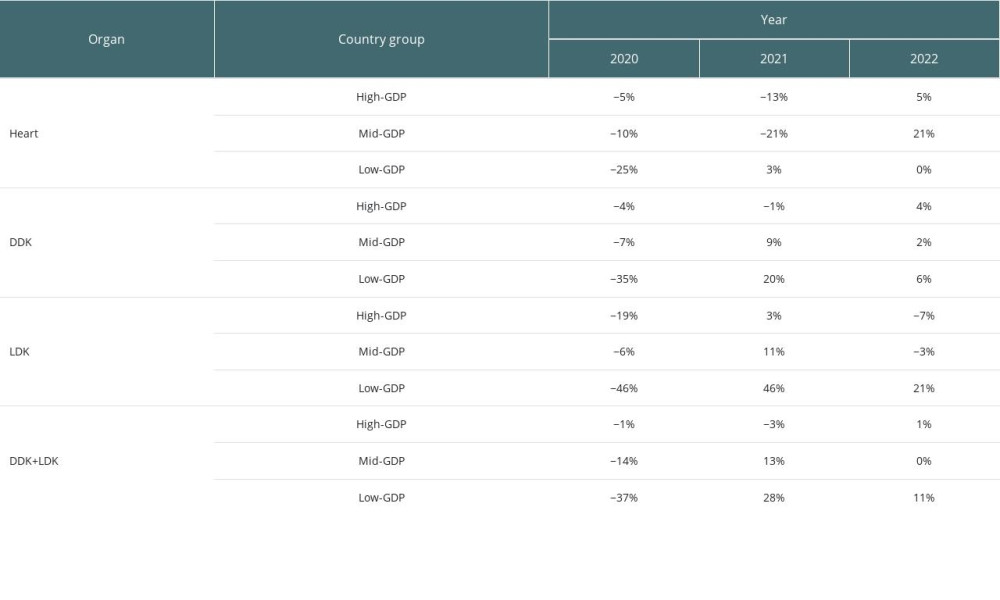 Table 7. The real change in heart, living donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation in the years 2020, 2021, and 2022. The observed numbers of transplants per million population (O), and the expected number of transplants per million population (E), as predicted by the artificial neural network model based on the data from 2015 to 2019 for the years 2020, 2021, and 2022 are shown. The recovery or decline in percentage (ie, ((O-E)/E)×100) is shown in parentheses.
Table 7. The real change in heart, living donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation in the years 2020, 2021, and 2022. The observed numbers of transplants per million population (O), and the expected number of transplants per million population (E), as predicted by the artificial neural network model based on the data from 2015 to 2019 for the years 2020, 2021, and 2022 are shown. The recovery or decline in percentage (ie, ((O-E)/E)×100) is shown in parentheses. Table 8. Prediction accuracy measure estimated by measuring the root mean squared error (RMSE) for the artificial neural network (ANN) model. Shown are the number of actual transplants in 2019 and the estimated number of transplants in 2019, forecasted based on transplantation data for the years 2015 to 2018. The low RMSE indicates the robustness of the ANN model for forecasting.
Table 8. Prediction accuracy measure estimated by measuring the root mean squared error (RMSE) for the artificial neural network (ANN) model. Shown are the number of actual transplants in 2019 and the estimated number of transplants in 2019, forecasted based on transplantation data for the years 2015 to 2018. The low RMSE indicates the robustness of the ANN model for forecasting.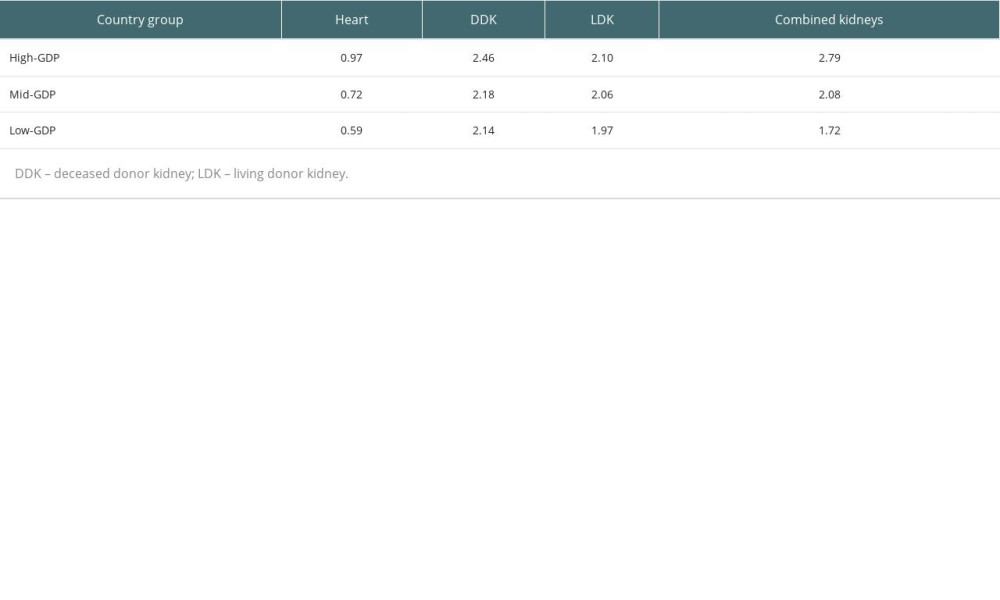
References
1. Aubert O, Yoo D, Zielinski D, Cozzi E, COVID-19 pandemic and worldwide organ transplantation: A population-based study: Lancet Public Health, 2021; 6(10); e709-e19
2. Nimmo A, Gardiner D, Ushiro-Lumb I, The global impact of COVID-19 on solid organ transplantation: Two years into a pandemic: Transplantation, 2022; 106(7); 1312-29
3. Kute VB, Tullius SG, Rane H, Global impact of the COVID-19 pandemic on solid organ transplant: Transplant Proc, 2022; 54(6); 1412-16
4. World Health Organization: WHO Coronavirus (COVID-19) dashboard Available from: https://covid19.who.int/
5. Hiscott J, Alexandridi M, Muscolini M, The global impact of the coronavirus pandemic: Cytokine Growth Factor Rev, 2020; 53; 1-9
6. Lopez L, Hart LH, Katz MH, Racial and ethnic health disparities related to COVID-19: JAMA, 2021; 325(8); 719-20
7. American Hospital Association: The Disproportionate Impact of COVID-19 on Communities of Color May 27, 2020 Available from: https://www.aha.org/testimony/2020-05-27-testimony-disproportionate-impact-covid-19-communities-color
8. Lange SJ, Ritchey MD, Goodman AB, Potential indirect effects of the COVID-19 pandemic on use of emergency departments for acute life-threatening conditions – United States, January–May 2020: MMWR Morb Mortal Wkly Rep, 2020; 69; 795-800
9. Alnour H, Sharma A, Halawa A, Alalawi F, Global practices and policies of organ transplantation and organ trafficking: Exp Clin Transplant, 2022; 20(8); 717-31
10. Shimazono Y, The state of the international organ trade: A provisional picture based on integration of available information: Bull World Health Organ, 2007; 85(12); 955-62
11. Duguay J-P, Hermon B, Smiath A, Trafficking in human organs: An overview: Library of parliament of Canada Available from: https://lop.parl.ca/sites/PublicWebsite/default/en_CA/ResearchPublications/202083E
12. Budiani-Saberi DA, Delmonico FL, Organ trafficking and transplant tourism: A commentary on the global realities: Am J Transplant, 2008; 8(5); 925-29
13. Ceylan RF, Ozkan B, Mulazimogullari E, Historical evidence for economic effects of COVID-19: Eur J Health Econ, 2020; 21; 817-23
14. Deb P, Furceri D, Ostry JD, Tawk N: The economic effects of COVID-19 containment measures, 2020, International Monetary Fund Available from: https://www.imf.org/en/Publications/WP/Issues/2020/08/07/The-Economic-Effects-of-COVID-19-Containment-Measures-49571
15. Padhan R, Prabheesh KP, The economics of COVID-19 pandemic: A survey: Economic Analysis and Policy, 2021; 70; 220-37
16. Bizuneh M, Geremew M, Assessing the Impact of COVID-19 pandemic on emerging market economies’ (EMEs) sovereign bond risk premium and fiscal solvency: East Econ J, 2021; 47(4); 519-45
17. Naseer S, Khalid S, Parveen S, COVID-19 outbreak: Impact on global economy: Front Public Health, 2022; 10; 1009393 Available from: https://doi.org/10.3389/fpubh.2022.1009393
18. Lee SS, Sielski MW, Charpentier KP, Association between the economic environment and the living organ donation rate: Evidence and implications: J Am Coll Surg, 2021; 232(2); 187-94
19. Sandal S, Massie A, Boyarsky B, Impact of the COVID-19 pandemic on transplantation by income level and cumulative COVID-19 incidence: A multinational survey study: BMJ Open, 2022; 12(1); e055367 Available from: http://dx.doi.org/10.1136/bmjopen-2021-055367
20. Ambagtsheer F, Bugter R, The organization of human organ trade: A comparative crime script analysis: Crime Law Soc Change, 2023; 80; 1-32
21. Lundin S, Organ economy: Organ trafficking in Moldova and Israel: Public Underst Sci, 2012; 21(2); 226-41
22. Kovac C, Kidney trafficking is “big business,” says Council of Europe: BMJ, 2003; 327(7409); 249
23. : Global Observatory on Donation and Transplantation (GODT), 2023, World Health Organization Available from: https://www.transplant-observatory.org/
24. : International Registry in Organ Donation and Transplantation (IRODaT), 2023, Barcelona, Spain, Donation and Transplantation Institute Available from: https://www.irodat.org/
25. The World Bank: DataBank, 2023, Washington DC, USA Available from: https://databank.worldbank.org/
26. Srivastava S, Tripathi KC, Artificial neural network and non-linear regression: A comparative study: Int J Sci Res Publ, 2012; 2(12); 740-44
27. Zhang GP, Time series forecasting using a hybrid ARIMA and neural network model: Neurocomputing, 2003; 50; 159-75
28. Hollander M, Wolfe DA, Chicken E: Nonparametric statistical methods, 2014, Hoboken (NJ), John Wiley & Sons
29. Hershberger SL, Hodges-Lehmann estimators: International Encyclopedia of Statistical Science, 2011; 635-36, Berlin, Springer
30. Wilcoxon F, Individual comparisons by ranking methods: Biometrics Bulletin, 1945; 1(6); 80-83
31. Jonckheere AR, A distribution-free k-sample test against ordered alternatives: Biometrika, 1954; 41; 133-45
32. Terpstra TJ, The asymptotic normality and consistency of Kendall’s test against trend, when ties are present in one ranking: Indagationes Mathematicae, 1952; 14; 327-33
33. Kendall MG: Rank correlation methods, 1962, London, Charles Griffin
34. Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Global challenges to public health care systems during the COVID-19 pandemic: A review of pandemic measures and problems: J Pers Med, 2022; 12(8); 1295
35. Gopinath G, The great lockdown: Worst economic downturn since the great depression: IMF BLOG Available from: https://www.imf.org/en/Blogs/Articles/2020/04/14/blog-weo-the-great-lockdown-worst-economic-downturn-since-the-great-depression
36. Center for Disease Control and Prevention (CDC): CDC Museum COVID-19 Timeline 2023
37. Loupy A, Aubert O, Reese PP, Organ procurement and transplantation during the COVID-19 pandemic: Lancet, 2020; 395(10237); e95-e96
38. White SL, Hirth R, Mahíllo B, The global diffusion of organ transplantation: trends, drivers and policy implications: Bull World Health Organ, 2014; 92(11); 826-35
39. Nevitt J, Hancock GR, Improving the root mean square error of approximation for nonnormal conditions in structural equation modeling: J Exp Edu, 2000; 68(3); 251-68
40. Swift R, The relationship between health and GDP in OECD countries in the very long run: Heath Econ, 2011; 20(3); 306-22
41. Miladinov G, Socioeconomic development and life expectancy relationship: Evidence from the EU accession candidate countries: Genus, 2020; 76(1); 2
42. Beylik U, Cirakli U, Cetin M, The relationship between health expenditure indicators and economic growth in OECD countries: A Driscoll-Kraay approach: Front Public Health, 2022; 10; 1050550
43. Stiglitz JE, Measuring what matters: Sci Am, 2020; 323(2); 24-31
44. Qureshi H, Mohyuddin H, Health status, diseases, and economic development: A cross-country analysis: J Developing Areas, 2006; 39(2); 121-28
45. Aisen A, Veiga FJ: How does political instability affect economic growth? IMF Working Paper, Middle East and Central Asia Department, 2010, International Monetary Fund Available from: https://www.imf.org/external/pubs/ft/wp/2011/wp1112.pdf
46. Bain C, Mari J, Delmonico FL, Organ trafficking: The unseen form of human trafficking: ACAMS Today June 26, 2018 Available from: https://www.acamstoday.org/organ-trafficking-the-unseen-form-of-human-trafficking/
47. Flaherty GT, Nasir N, Gormley CM, Pandey S, Transplant tourism and organ trafficking: Current practices, controversies, and solutions: In J Travel Med Glob Health, 2021; 9(3); 102-6
48. Broumand B, Saidi RF, New definition of transplant tourism: Int J Organ Transplant Med, 2017; 8(1); 49-51
49. Smith A, Medical tourism and organ trafficking: African J Hospitality, Tourism Leisure, 2012; 2(1) Available from: http://www.ajhtl.com/uploads/7/1/6/3/7163688/smith_a._vol._2_1_-_2012.pdf
50. Usman M, Yuyan L, Husnain M, Waheed MW, COVID-19, travel restrictions and environmental consequences: Environ Dev Sustain, 2023; 18; 1-21
51. Nimmo A, Gardiner D, Ushiro-Lumb I, The global impact of COVID-19 on solid organ transplantation: Two years into a pandemic: Transplantation, 2022; 106(7); 1312-29
52. Johns Hopkins University School of Medicine: Maps and Trends of Mortality Analyses, 2023 Available from: https://coronavirus.jhu.edu/data/mortality
53. Bayati M, Why is COVID-19 more concentrated in countries with high economic status?: Iran J Public Health, 2021; 50(9); 1926-29
54. Nicola M, Alsafi Z, Sohrabi C, The socio-economic implications of the coronavirus pandemic (COVID-19): A review: Int J Surgery, 2020; 78; 185-93
55. Susskind D, Vines D, The economics of the COVID-19 pandemic: An assessment: Oxford Review of Economic Policy, 2020; 36; S1-S13 Available from: https://doi.org/10.1093/oxrep/graa036
56. De PK, Price T, Pre-existing economic conditions and COVID-19 infections and mortality in New York City: J Health Care Poor Underserved, 2021; 32(4); 1978-94
57. Ritschl PV, Nevermann N, Wiering L, Solid organ transplantation programs facing lack of empiric evidence in the COVID-19 pandemic: A By-proxy Society Recommendation Consensus approach: Am J Transplant, 2020; 20(7); 1826-36
58. American Society for Transplantation: SARS-CoV-2: Recommendations and Guidance for Organ Donor Testing and Evaluation Updated on October 5, 2020 The 2023 update available from: https://www.myast.org/sites/default/files/Donor%20Testing%20Document1.18.23.pdf
59. Josephson A, Kilic T, Michler JD, Socioeconomic impacts of COVID-19 in low-income countries: Nat Hum Behav, 2021; 5; 557-65
60. Ugur ZB, Perez AM, The toll of COVID-19 on organ donation and kidney transplantation in Europe: Do legislative defaults matter?: Health Policy, 2023; 136; 104890 Available from: https://www.sciencedirect.com/science/article/abs/pii/S0168851023001756?dgcid=author
61. Katvan E, Cohen J, Ashkenazi T, Organ donation in the time of COVID-19: the Israeli experience one year into the pandemic-ethical and policy implications: Isr J Health Policy Res, 2022; 11(1); 6
62. Haileamlak A, Pandemics will be more frequent: Ethiop J Health Sci, 2022; 32(2); 228
63. Marani M, Katul GG, Pan WK, Parolari AJ, Intensity and frequency of extreme novel epidemics: PNAS, 2021; 18(35); e2105482118
64. Chang D, Chang X, He Y, Tan KJK, The determinants of COVID-19 morbidity and mortality across countries: Sci Rep, 2022; 12(1); 5888
Figures
Figure 1. A dendrogram of the 30 countries, clustered based on gross domestic product (GDP). The Y-axis shows the distance between the clusters. The figure was created using Statistical Computing Software R 4.3.1 package ggplot2 (https://www.r-project.org/).Figure 2. Side-by-side boxplots showing the median effect size of COVID-19 on heart and kidney transplantation in the 3 groups of countries. The dark solid line in the box indicates the median effect; the outlier detection lines and the outliers (the empty circles) are also shown. 1 – high- gross domestic product (GDP) nations; 2 – mid-GDP nations; 3 – low-GDP nations. The median effect is more pronounced for less-developed countries, as indicated by the shift of the median effect to <0. The figure was created using Statistical Computing Software R 4.3.1, package ggplot2 (https://www.r-project.org/). Tables
Table 1. Year-to-year changes in heart, live donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation per million population over the years 2016 to 2020 in high-gross domestic product (GDP), mid-GDP, and low-GDP countries. The annual change is calculated based on the actual number of transplants performed in that year (Y2) and the previous year (Y1), using the formula ((Y2-Y1)/Y1)×100, thus, data for 2015 is not shown.Table 2. The median effect size per million population of the COVID-19 pandemic on heart and kidney transplantation by countries’ gross domestic product (GDP), along with 95% CI and P values for the null hypothesis of the median effect being zero are shown. A negative value for the median effect size indicates a negative effect and a positive value for the median effect size indicates a positive effect of the pandemic.Table 3. Summary statistics of the impact size (per million population) of the COVID-19 pandemic on heart and kidney transplantation and P values for Jonckheere-Terpstra test θ1 θ2 θ3. Here, θ1, θ2, and θ3 represent the median effect for high-gross domestic product (GDP), mid-GDP, and low-GDP countries, respectively.Table 4. Kendall Tau association between economic variables and numbers of heart and kidney transplants. The high P values (shown in parentheses) indicate a lack of a significant association between economic indicators and heart and kidney transplantation.Table 5. Kendall Tau association between COVID-19 incidence, COVID-19 mortality, and the numbers of heart and kidney transplants. The high P values (shown in parentheses) indicate a lack of a significant association between COVID-19 incidence and COVID-19-related morality and heart and kidney transplantation.Table 6. Year-to-year changes in heart, living donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation per million population over the years 2020, 2021, and 2022 in high-gross domestic product (GDP), mid-GDP, and low-GDP countries. The annual change is calculated based on the actual number of transplants performed in that year (Y2) and the previous year (Y1), using the formula ((Y2-Y1)/Y1))×100.Table 7. The real change in heart, living donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation in the years 2020, 2021, and 2022. The observed numbers of transplants per million population (O), and the expected number of transplants per million population (E), as predicted by the artificial neural network model based on the data from 2015 to 2019 for the years 2020, 2021, and 2022 are shown. The recovery or decline in percentage (ie, ((O-E)/E)×100) is shown in parentheses.Table 8. Prediction accuracy measure estimated by measuring the root mean squared error (RMSE) for the artificial neural network (ANN) model. Shown are the number of actual transplants in 2019 and the estimated number of transplants in 2019, forecasted based on transplantation data for the years 2015 to 2018. The low RMSE indicates the robustness of the ANN model for forecasting.Table 1. Year-to-year changes in heart, live donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation per million population over the years 2016 to 2020 in high-gross domestic product (GDP), mid-GDP, and low-GDP countries. The annual change is calculated based on the actual number of transplants performed in that year (Y2) and the previous year (Y1), using the formula ((Y2-Y1)/Y1)×100, thus, data for 2015 is not shown.Table 2. The median effect size per million population of the COVID-19 pandemic on heart and kidney transplantation by countries’ gross domestic product (GDP), along with 95% CI and P values for the null hypothesis of the median effect being zero are shown. A negative value for the median effect size indicates a negative effect and a positive value for the median effect size indicates a positive effect of the pandemic.Table 3. Summary statistics of the impact size (per million population) of the COVID-19 pandemic on heart and kidney transplantation and P values for Jonckheere-Terpstra test θ1 θ2 θ3. Here, θ1, θ2, and θ3 represent the median effect for high-gross domestic product (GDP), mid-GDP, and low-GDP countries, respectively.Table 4. Kendall Tau association between economic variables and numbers of heart and kidney transplants. The high P values (shown in parentheses) indicate a lack of a significant association between economic indicators and heart and kidney transplantation.Table 5. Kendall Tau association between COVID-19 incidence, COVID-19 mortality, and the numbers of heart and kidney transplants. The high P values (shown in parentheses) indicate a lack of a significant association between COVID-19 incidence and COVID-19-related morality and heart and kidney transplantation.Table 6. Year-to-year changes in heart, living donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation per million population over the years 2020, 2021, and 2022 in high-gross domestic product (GDP), mid-GDP, and low-GDP countries. The annual change is calculated based on the actual number of transplants performed in that year (Y2) and the previous year (Y1), using the formula ((Y2-Y1)/Y1))×100.Table 7. The real change in heart, living donor kidney (LDK), deceased donor kidney (DDK), and combined kidney transplantation in the years 2020, 2021, and 2022. The observed numbers of transplants per million population (O), and the expected number of transplants per million population (E), as predicted by the artificial neural network model based on the data from 2015 to 2019 for the years 2020, 2021, and 2022 are shown. The recovery or decline in percentage (ie, ((O-E)/E)×100) is shown in parentheses.Table 8. Prediction accuracy measure estimated by measuring the root mean squared error (RMSE) for the artificial neural network (ANN) model. Shown are the number of actual transplants in 2019 and the estimated number of transplants in 2019, forecasted based on transplantation data for the years 2015 to 2018. The low RMSE indicates the robustness of the ANN model for forecasting. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988