07 May 2024: Original Paper
Transplant Nephrectomy: A Comparative Study of Timing and Techniques in a Single Institution
Ursula Pession1ABCDE*, Ingrid Lammers1BCF, Ingeborg Hauser2AE, Teresa Schreckenbach1CE, Andreas Schnitzbauer1E, Jeannine Lang2B, Michael Heise1BD, Wolf Otto Bechstein1ADEDOI: 10.12659/AOT.942252
Ann Transplant 2024; 29:e942252






Abstract
BACKGROUND: Transplant nephrectomy (TN) has historically been associated with high morbidity and mortality rates. Our objective is to share our own experience and compare indications and surgical outcomes between early and late TN and intracapsular (ICAN) and extracapsular allograft nephrectomy (ECAN) techniques.
MATERIAL AND METHODS: Our study included all 69 TN procedures performed between January 2010 and February 2021. Of these, 17 TN procedures were performed within the first 60 days after transplantation (referred to as ‘early’), while the remaining 52 procedures were performed later (‘late’). Within the late allograft nephrectomy (AN) group, we compared the outcomes of intracapsular (ICAN) and extracapsular (ECAN) techniques. We conducted a statistical analysis using the chi-square test and the 2-sample t test.
RESULTS: The primary indication for early TN was surgical transplant complications (94.1%), with 58.8% of these cases requiring emergency surgery. Morbidity (major complications) occurred in 47.1% of cases, and mortality was 5.9%. In contrast, graft intolerance syndrome was the leading indication for late TN (76.9%), with elective surgery performed in 88.5% of cases. Morbidity (major complications) occurred in 11.5% of cases, and mortality was 3.8%. Within the late TN group, 82.7% of cases were treated with ICAN and 17.3% with ECAN. Blood transfusion was required during surgery in 17.3% of cases, with no significant difference between the groups. Multivariate logistic regression analysis revealed that the timing of surgery was the only statistically significant predictor of complication occurrence.
CONCLUSIONS: Our data suggest that TN can be performed with relatively low morbidity. However, early TN remains the only independent risk factor for developing adverse outcomes.
Keywords: Kidney Transplantation, Nephrectomy, transplant recipients, Humans, Female, Male, Middle Aged, adult, Postoperative Complications, Time Factors, Retrospective Studies, Treatment Outcome, Aged
Introduction
Renal transplantation is the preferred treatment for end-stage renal disease. However, 10% of patients return to dialysis during the first year after transplantation, and 25% return after 5 years [1,2]. Approximately 4% of transplant recipients return to dialysis yearly [1,2]. Some of these patients will undergo transplant nephrectomy (TN).
TN is considered a challenging procedure with high morbidity and mortality rates [3]. The indications for TN vary and include acute irreversible rejection, thrombosis, technical failure in early TN, graft intolerance syndrome, infection, and malignancy in late TN [4]. The time of surgery also affects the surgical technique used since a desmoplastic reaction develops around the graft over time, resulting in development of a fibrotic capsule that surrounds the graft and adheres to the abdominal wall and renal hilum. This capsule makes it more difficult to identify the hilus. Two different techniques are used in TN, depending on the capsule: intracapsular allograft nephrectomy (ICAN) and extracapsular allograft nephrectomy (ECAN) [5].
Perioperative morbidity has been reported to vary depending on the time and technique of surgery [6]. The purpose of this study was to analyze our own experience over the last 11 years. We compared the clinical characteristics of patients who underwent TN according to the time and technique of TN to define risk factors for morbidity and mortality.
Material and Methods
PATIENT DEMOGRAPHICS AND CLINICAL DATA:
Data for this study were collected from electronic health records. Between January 1, 2010 and February 28, 2021, we performed 69 TNs and 661 TXs. We collected patient-specific and surgery-specific data and divided the TNs into 2 groups based on transplant survival up to or beyond 60 days: early (n=17) and late (n=52) TNs.
We recorded patients’ age, sex, concomitant diseases, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, blood specimens at the time of TN, living or deceased donor, the reason for graft failure, and indication for graft removal. Surgical variables included urgency, duration of surgery, blood transfusion, and technique (ICAN/ECAN). ICAN (intracapsular allograft nephrectomy) is an intracapsular approach that facilitates easier identification of the hilum, which is secured by a running continuous non-absorbable suture after clamping while leaving the capsule and ureter as donor tissue in situ. ECAN (extracapsular allograft nephrectomy) is a more radical approach in which the entire kidney is resected with complete isolation of the ureter, renal artery, and vein, which are individually ligated and divided. Gibson incision is standard for TN after kidney TX and median laparotomy for TN after simultaneous pancreas-kidney TX; otherwise, the surgery is performed the same way.
Complications were classified using the Clavien-Dindo scale [7]. For better analysis of this small study population, complications were divided into minor and major categories. Minor complications were defined as Clavien-Dindo grade I and II, while major complications were Clavien-Dindo grade III to V.
STATISTICS:
All statistical analyses were performed using IBM’s SPSS for Windows (version 28.0; Chicago, IL, USA). Categorical variables are shown as frequencies and percentages, while continuous variables are represented as means and standard deviations (SDs). We used the chi-squared (χ2) test or Fisher’s exact test, as needed, to compare categorical variables and a 2-sample
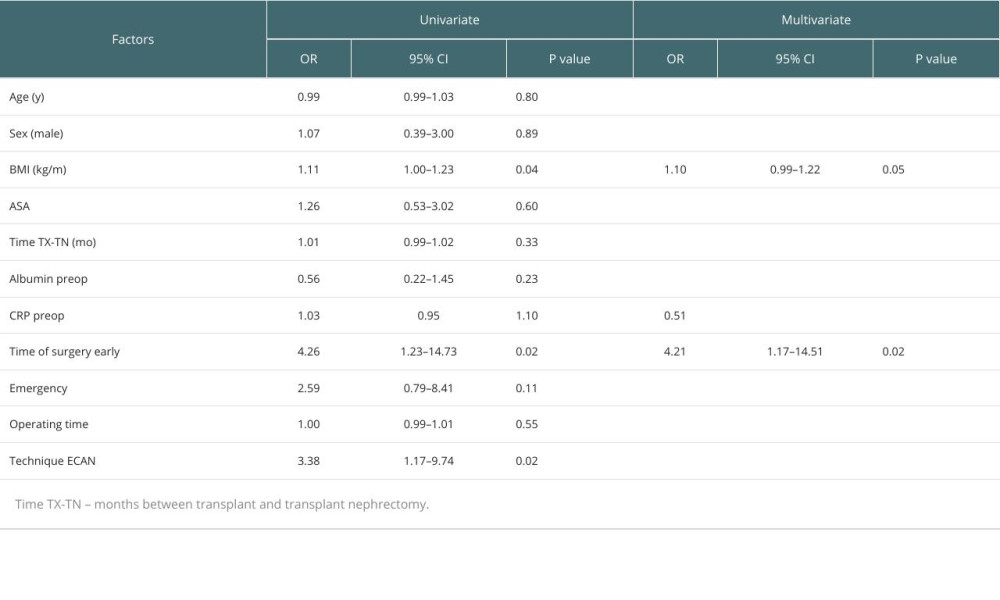
We performed regression analysis to identify predictive factors for complications following TN. For the univariate analysis, we used age, sex, BMI, ASA classification, the time between transplant and TN, preoperative albumin and C-reactive protein, time of surgery (early/late), emergency status, duration of surgery, and surgical technique. We calculated the odds ratio for complications with a 95% confidence interval (CI) and
We performed multivariate linear regression analysis for the significant parameters identified in the univariate analysis: BMI and time of surgery (early TN – late TN). To avoid multicollinearity, we excluded surgical technique from the multivariate analysis, as it showed a significant correlation in the chi-squared (χ2) test with the time of surgery. We considered
Results
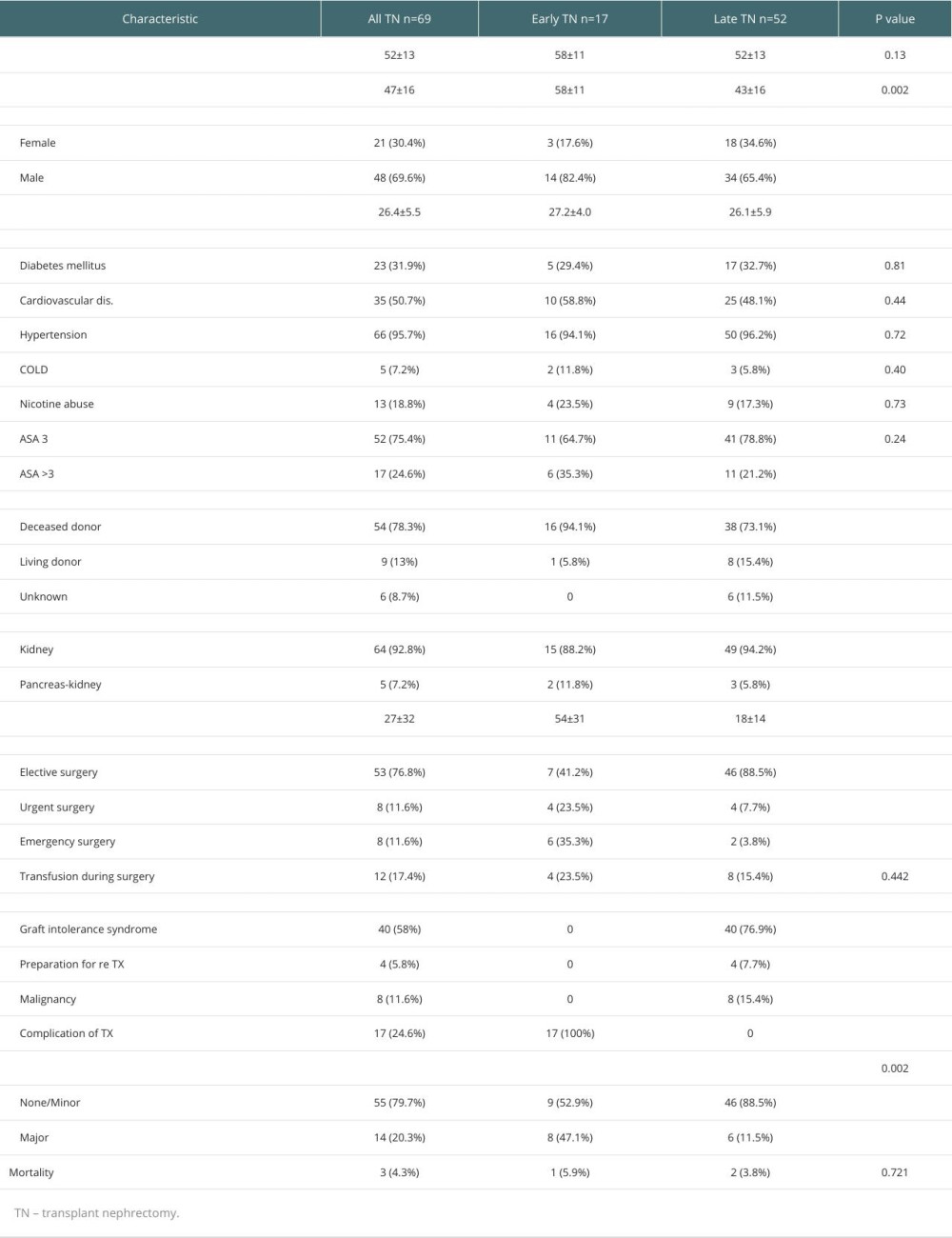
Among the 69 patients with TN, 21 were female and 48 were male, with a mean age of 54±13 years and a mean BMI of 26.4±5.5 kg/m2. Renal transplants were from deceased donors in 54 cases (78.3%), living donors in 9 cases (13%), and unknown in 6 cases (8.7%). Simultaneous pancreas-kidney transplantation was performed in 5 cases (7.2%). At the time of TN, 75.5% of the patients were classified as ASA 3, 21.7% as ASA 4, and 2.9% as ASA 5. In addition to renal disease, 95.7% of the patients had arterial hypertension, 50.7% had cardiovascular diseases (CVD), 31.9% had diabetes mellitus, 18.8% had nicotine abuse, and 7.2% had COLD. None of the patient had a previous embolization of the allograft.
The indication for TN was graft intolerance syndrome in 57.9%, malignancy in 11.6%, a surgical reason (the plan of new transplant) in 5.8%, and early complications around TX in 24.6%. This last group had TN during the first 60 days after TX and will be referred to as the early TN group. The other group will be called the late TN group and had TN performed more than 60 days after TX in the late TN group, 82.7% had ICAN, and 17.3% had ECAN. Perioperative parameters are shown in Table 1. Mean duration of dialysis before TN was 14 ±21 months in the ICAN group and 27±47 in the ECAN group.
Most patients had elective surgery (76.8%), while some had urgent (11.6%) and emergency (11.6%) surgery. The mean operative time was 114±77 min. The length of hospital stay ranged from 5 to 213 days, with a mean of 27±32 days. Operative minor complications were seen in 33.3% of the cases, while major complications were seen in 20.4%. Minor complications included blood transfusions, surgical site infections, hematoma, 1 reversible lesion of the femoral nerve, and diarrhea. Major complications were discovered in 12 patients and included 4 cases of bleeding, 2 cases of surgical site infection (SSI) grade III, 1 case of seroma, 1 case of dissection of the external iliac artery, 1 case of rectal perforation, 2 cases of sepsis, and 1 case of fascial dehiscence.
The mortality rate was 4.3%, meaning 3 out of 69 patients died during their hospital stay. One patient, a 28-year-old man in the early TN group, had simultaneous pancreas-kidney transplantation (SPK), and developed immunotherapy-induced hepatotoxicity. Organs were explanted 13 days after TX to save the patient, but he died due to fulminant liver failure. The other 2 patients were in the late TN group. One patient, a 45-year-old woman on dialysis, had a perforation of the sigma with complications and underwent multiple re-laparotomies. TN was performed during one of these surgeries, but it did not change the patient’s medical course, and she died from sepsis. The last patient, a 65-year-old man with prostate and bladder cancer, had simultaneous cystoprostatectomy and TN. This was complicated by rectal perforation after surgery, and he died due to a heart attack during re-laparotomy. Only this last patient had TN as an indication for TN surgery and died afterward.
We compared early and late TN for all the described factors and found a significantly higher incidence of major complications in the early group (47.1% in early TN and 11.5% in late TN). The indication for surgery was significantly different, with ischemia and bleeding (76.5%) being more common in the early TN group and graft intolerance syndrome (76.9%) being more common in the late group. Emergency surgery was performed significantly more often in early TN (35.3%). ECAN was performed significantly more often in early TN, which is self-evident, since the capsule does not form shortly after TX. Laboratory findings, such as CRP, hemoglobin, leukocyte count, albumin, and total proteins, were similar in both groups. The chance of being relisted for transplant was similar (17.6% in early TN and 13.5% in late TN), but there was a higher rate of re-transplantation in the late TN group (13.4% versus 5.9% in early TN).
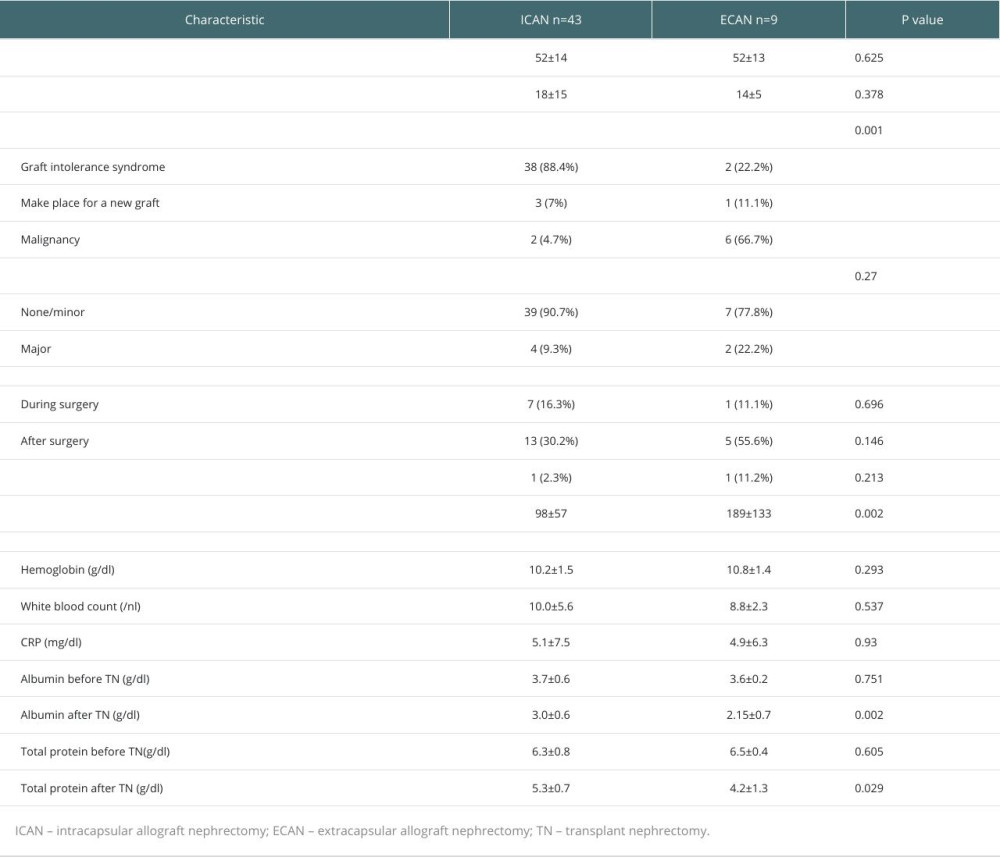
Lastly, we compared ICAN/ECAN in the late TN group and found no significant differences in patient characteristics (Table 2). However, indications for TN were significantly different, with graft intolerance syndrome being the leading indication (88.4%) in ICAN and malignancy of the graft being the leading indication (66.7%) in ECAN. The mean duration of surgery was significantly longer in ECAN. Analysis of laboratory findings showed a significantly lower albumin level postoperatively in ECAN, which correlates with a higher malignancy rate and longer operating time.
To identify the risk factors for surgery-related complications in each group, we analyzed clinical and laboratory parameters using univariate and multivariate logistic regression models (Table 3). Early TN was a significant independent factor in developing adverse outcomes.
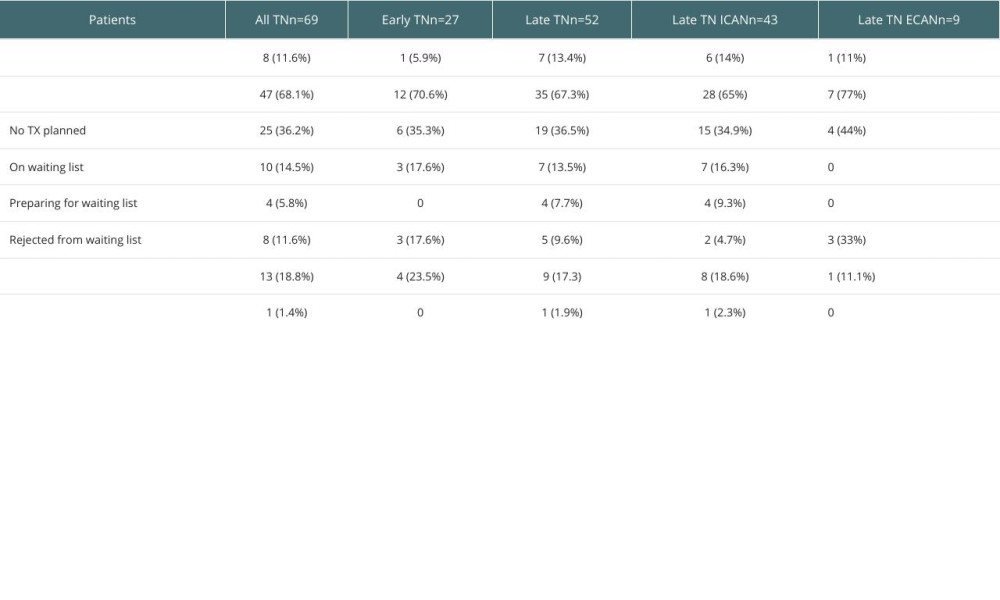
Follow-up was established in April 2021 (Table 4). At this time, 11.6% of all patients who had undergone graft nephrectomy had received a new renal transplant. One patient (5.9%) in the early TN group received a new graft, while 7 (13.5%) in the late TN group had received a new graft, mostly in the ICAN group (6/7). Overall, 18.8% of the patients had died, and 14.5% had been relisted for a transplant.
Discussion
International guidelines for performing TN in cases of renal transplant failure are currently unavailable. Therefore, each transplant center follows its own clinical standards of practice. The first data on 31 TN patients was published by Sharma et al in 1989, which reported a morbidity rate of 64.5% and a mortality rate of 41% [8]. Only 5 years later, O’Sullivan reported on 86 TN patients, with a lower morbidity rate of 60% and mortality rate of 4.6% [9]. Many subsequent studies have reported morbidity rates ranging from 5% to 48.3% and mortality rates ranging from 0%to 7% [4,10,11]. The largest population was analyzed by Johnson et al in 2007 [12]. This cohort study included 6213 TN procedures performed between 1995 and 2003 in the United States, which reported a mortality rate of 5% [12].
In our population, we observed a mortality rate of 4.3% for all TN procedures. Upon analyzing individual patients, we found that only 1 patient who underwent TN had it as the primary indication for surgery, which is consistent with previous reports. In the other 2 cases, TN was performed during surgery for other reasons, or the patient died due to a pre-existing condition that was not altered or improved by graft nephrectomy. Thus, if we analyze the mortality rate based on the indication for surgery rather than the performed procedure, we arrive at a mortality rate of 1.4%.
As the Clavien-Dindo classification was implemented after 2004, it is difficult to directly compare morbidity data over a long period [7]. Mazzucchi et al reported only surgical complications as morbidity and classified them as major if patients required second surgery and as or minor if surgery was unnecessary [6]. Chowanek et al employed the Clavien-Dindo classification system but only for surgical complications and reported a morbidity rate of 38% for grades I to IV [3]. Meanwhile, Alberts et al and Sun et al did not use the Clavien-Dindo classification and considered every TN-related event as morbidity [13,14].
In summary, morbidity and mortality rates have decreased since the earlier reports but have remained relatively stable over the last decade. The overall morbidity rate (major, Clavien-Dindo III–V) in our population was 20.3%, which is consistent with the data reported in the literature.
To analyze morbidity in detail, we divided the population by the time and technique of TN. The early TN group had a significantly higher morbidity rate than the late TN group (47.1% vs 11.5%). However, Alberts et al did not find any association between the time of TN and morbidity [13]. Other authors have reported more complications with late TN [3,6,15]. This could be explained by the different definitions of early TN used in different studies, which were 30 days, 60 days, 6 months, and 1 year [5,6,14,16]. In our study, we defined early TN as occurring within 60 days after transplantation for 2 reasons: (1) during the first 2 months after transplantation, graft nephrectomy is often related to technical or medical issues of the transplant, and (2) the capsule around the graft is not completely formed during the first 60 days.
Patients who underwent early graft nephrectomy were significantly older than patients in the late TN group at the time of transplantation. Some of them had received a kidney graft within the Eurotransplant Senior Program [17]. However, even though they were older at the time of transplantation, the patients undergoing early TN did not differ in terms of comorbidities at the time of graft nephrectomy from patients undergoing late TN.
Early TN is often an emergency surgery compared to late TN and is typically indicated for complications of transplantation. As such, early TN can be viewed as revision surgery. In our study, the indications for early TN were ischemia, bleeding, and thrombosis in most cases (76.5%). We performed early TN in 2.5% of all TX in the study period.
As previously described by Secin et al, emergency graft nephrectomy is associated with significantly higher morbidity and mortality [4]. Our study also found that the complication rate was significantly higher in emergency surgeries (
The multivariate analysis revealed that early graft nephrectomy was the only independent risk factor for developing adverse outcomes. Regarding the technique of graft nephrectomy, we only considered ICAN and ECAN for the late TN group, as the capsule is not fully formed during the first 2 months after transplantation. Late TN patients mostly underwent elective surgery for graft intolerance syndrome, chronic infection, or malignancy.
We did not observe significant differences in morbidity and mortality between ICAN and ECAN in the late TN group, although we noted a higher incidence of major complications (9.3% in ICAN and 22.2% in ECAN) and mortality in the ECAN group. Similar findings were reported by Touma et al and Eng et al, who demonstrated less blood loss, shorter operating time, and fewer complications in the ICAN group [5,18]. However, the study by Mazzucchi et al reported more complications, greater blood loss, and more transfusions in the ICAN group [6]. Freitas et al also found more complications in the ICAN group [16].
As malignancy was the primary indication for ECAN, some patients in this group underwent more aggressive surgery, including cystoprostatectomy in 1 case, which may explain the higher incidence of major complications. The significantly longer operating time observed in graft nephrectomies performed using the ECAN technique is also related to this issue.
At the time of follow-up, 8% of the population had received a new renal graft. Of all patients, 18.8% had died, with a higher percentage in the early TN group (23.5%). This finding was consistent with that reported by Johnson et al, who also noted a higher incidence of cardiovascular diseases that correlated with mortality [12]. Although we observed a higher incidence of cardiovascular diseases in our study, it was not statistically significant.
Patients in the late TN group who underwent ECAN surgery were not planned for transplantation, as malignancy was the primary indication for the ECAN technique, and malignancy typically precludes readmission to the waiting list for 5 years. However, the current study is limited by its retrospective nature, small sample size, and single-center institution.
Conclusions
In conclusion, this retrospective study on transplant nephrectomy demonstrates that allograft nephrectomy comprises different procedures ranging from emergency allograft nephrectomy due to acute rejection on the day of transplant to elective ECAN and cystoprostatectomy for cancer treatment.
Our data indicate that these procedures can be performed safely with relatively low morbidity and mortality rates, even when considering the different types of procedures involved. Early TN is the only independent risk factor for developing adverse outcomes, which is not an intrinsic characteristic of TN but rather a reflection of technical or patient-related problems associated with the transplant.
References
1. McDonald S, Russ G, Campbell S, Chadban S, Kidney transplant rejection in Australia and New Zealand: Relationships between rejection and graft outcome: Am J Transplant, 2007; 7; 1201-8
2. Meier-Kriesche HU, Schold JD, Kaplan B, Long-term renal allograft survival: Have we made significant progress or is it time to rethink our analytic and therapeutic strategies?: Am J Transplant, 2004; 4; 1289-95
3. Chowaniec Y, Luyckx F, Karam G, Transplant nephrectomy after graft failure: Is it so risky? Impact on morbidity, mortality and alloimmunization: Int Urol Nephrol, 2018; 50; 1787-93
4. Secin FP, Rovegno AR, del Rosario Brunet M, Cumulative incidence, indications, morbidity and mortality of transplant nephrectomy and the most appropriate time for graft removal: Only nonfunctioning transplants that cause intractable complications should be excised: J Urol, 2003; 169; 1242-46
5. Touma NJ, Sener A, Caumartin Y, Extracapsular versus intracapsular allograft nephrectomy: Impact on allosensitization and surgical outcomes: Can Urol Assoc J, 2011; 5; 49-52
6. Mazzucchi E, Nahas WC, Antonopoulos IM, Surgical complications of graft nephrectomy in the modern transplant era: J Urol, 2003; 170; 734-37
7. Clavien PA, Barkun J, de Oliveira ML, The Clavien-Dindo classification of surgical complications: Five-year experience: Ann Surg, 2009; 250; 187-96
8. Sharma DK, Pandey AP, Nath V, Gopalakrishnan G, Allograft nephrectomy – a 16-year experience: Br J Urol, 1989; 64; 122-24
9. O’Sullivan DC, Murphy DM, McLean P, Donovan MG, Transplant nephrectomy over 20 years: Factors involved in associated morbidity and mortality: J Urol, 1994; 151; 855-58
10. Zargar MA, Kamali K, Reasons for transplant nephrectomy: A retrospective study of 60 cases: Transplant Proc, 2001; 33; 2655-56
11. Vanrenterghem Y, Khamis S, The management of the failed renal allograft: Nephrol Dial Transplant, 1996; 11; 955-57
12. Johnston O, Rose C, Landsberg D, Nephrectomy after transplant failure: Current practice and outcomes: Am J Transplant, 2007; 7; 1961-67
13. Alberts VP, Minnee RC, Bemelman FJ, van Donselaar-van der Pant KA, Idu MM, Transplant nephrectomy: What are the surgical risks?: Ann Transplant, 2013; 18; 174-81
14. Sun IO, Hong YA, Park HS, Comparison of the clinical characteristics of renal transplant recipients who underwent early versus late graft nephrectomy: Transplant Proc, 2013; 45; 2953-56
15. Grochowiecki T, Szmidt J, Galazka Z, Influence of timing of transplant nephrectomy on surgical complications: Transplant Proc, 2000; 32; 1381
16. Freitas R, Malheiro J, Santos C, Allograft nephrectomy: A single-institution, 10-year experience: Transplant Proc, 2015; 47; 992-95
17. Rose C, Schaeffner E, Frei U, A lifetime of allograft function with kidneys from older donors: J Am Soc Nephrol, 2015; 26; 248393
18. Eng MM, Power RE, Hickey DP, Little DM, Vascular complications of allograft nephrectomy: Eur J Vasc Endovasc Surg, 2006; 32; 212-16
In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988