18 March 2025: Original Paper
Effect of a Nursing Program on Anxiety, Depression, and Insomnia in Patients After Liver Transplantation: A Randomized Controlled Trial
Shuang-Mei Xi ABCDEF 1, Yan-Mei Gu ABCDEF 1, Hui-Min Guo ABCDEF 2, Xin Liu ABCDEF 1, Yu-Lin Zheng ABCDEF 1, Guang-Ming Li ABCDEFG 3*, Li-Li Zhang ABCDEF 2
DOI: 10.12659/AOT.947351
Ann Transplant 2025; 30:e947351






Abstract
BACKGROUND: The incidence of anxiety, depression, and sleep disturbances is high among patients after liver transplantation, significantly impacting their quality of life. However, existing nursing programs often lack a comprehensive focus on psychological and physical health outcomes. This study aimed to evaluate the effectiveness of a targeted nursing program in reducing anxiety, depression, and sleep disturbances among liver transplantation patients through psychological care, lifestyle guidance, pain management, and rehabilitation training.
MATERIAL AND METHODS: A randomized controlled trial was conducted with 80 liver transplantation patients at Beijing Youan Hospital (2021-2023). Patients were randomly assigned to the control group (traditional nursing, n=40) or the intervention group (targeted nursing, n=40). The intervention included psychological care, lifestyle guidance, pain management, and rehabilitation training. Anxiety, depression, and sleep quality were assessed using the SDS, HAMA, and PSQI at 4 time points: 0-60, 61-120, 121-180, and 181-360 days after surgery.
RESULTS: The incidence of anxiety, depression, and insomnia at 0-60, 61-120, 121-180, and 181-360 days after liver transplantation was 42.50%, 37.50%, 35.00%, and 30.00%; 14.50%, 9.40%, 3.20%, and 1.20%; and 15.80%, 12.10%, 7.30%, and 6.50%, respectively. After the care program, the depression, anxiety, and sleep scores were lower in the intervention group than in the control group and gradually decreased over time (p<0.05).
CONCLUSIONS: The nursing program after liver transplantation includes postoperative psychology, pain care, life strategies, and rehabilitation training, which can effectively reduce the depression, anxiety, and sleep scores of patients and is recommended for wide use.
Keywords: Anxiety, Incidence, Transplantation, Humans, Liver Transplantation, Female, Male, Sleep Initiation and Maintenance Disorders, Depression, Middle Aged, adult, Quality of Life, Postoperative Complications
Introduction
Liver transplantation is an important and complex surgical procedure that is commonly used to treat various liver diseases, including cirrhosis, liver cancer, and acute liver failure [1]. Because liver transplantation is a highly stressful and risky process, both the operation itself and the postoperative recovery process can have a serious impact on the physical and mental health of patients, including the occurrence of anxiety and depressive symptoms [2]. Patients also often experience sleep problems after surgery, such as difficulty falling asleep, shallow sleep, and waking up at night [3]; such problems increase the risk of anxiety and depression. The study found high rates of anxiety, depression, and insomnia after liver transplantation, at 29%, 25%, and 28%, respectively. Psychological complications following liver transplantation are associated with many factors [4], such as the patient’s age, gender, and education, surgical procedures, and postoperative care; they may also be associated with physical and psychological stress caused by surgery [5–7]. Factors such as uncertainty during recovery, pain, and medication adverse effects may also aggravate patient anxiety [8,9]. Anxiety and depression not only reduce the quality of life of patients but may also affect their rehabilitation process and the survival of transplanted organs.
In summary, healthcare professionals must pay close attention to the psychological and physical condition of patients and the support of their families and community, and should provide individualized care programs to help patients relieve anxiety and promote their physical recovery [10]. Previous studies have focused on psychological interventions in liver transplant patients [11,12], and few systematic nursing programs after liver transplantation have intervened in other aspects of patient care. One study [11] used mindfulness training to intervene in the anxiety and depression levels and sleep quality of patients after liver transplantation and found that it could reduce their anxiety and depression levels and improve sleep quality. However, the study was primarily psychological and did not involve other programs, and the number of interventions was small. Other nursing studies [13] have focused on the nursing period in the hospital and did not follow up on their psychological status after discharge to study their long-term effects.
While these previous studies have provided valuable insights into the psychological challenges faced by liver transplantation patients, they lack a comprehensive approach that integrates multiple facets of patient care. Postoperative recovery is a complex process involving not only psychological adjustment but also physical rehabilitation, pain management, and lifestyle modifications. Addressing these interconnected aspects is essential for achieving sustainable improvements in patients’ quality of life. This highlights an unmet need for a systematic and multifaceted nursing program that goes beyond psychological interventions to encompass a broader spectrum of postoperative care.
Therefore, we performed the present randomized controlled trial to assess a nursing program after liver transplantation that includes training in psychology, pain management, life strategies, and rehabilitation, as a holistic intervention for patients and follow-up to observe its long-term effects. The aim was to investigate whether the nursing program can effectively reduce anxiety, depression, and sleep scores of patients after liver transplantation.
Material and Methods
RESEARCH PARTICIPANTS:
This was a randomized controlled trial. A total of 80 patients who underwent liver transplantation at the surgery center of Beijing Youan Hospital between January 2021 and December 2023 were selected as the study participants using convenience sampling. All methods were carried out in accordance with relevant guidelines and regulations.
Randomization was performed according to the random number table method. A random number table was used to generate random numbers for each participant, and participants with odd numbers were assigned to the control group, which followed the traditional care protocol (n=40 patients). Participants with even numbers were assigned to the intervention group, which followed the post-liver transplantation care protocol (n=40 patients). This process was performed manually by a researcher to ensure the randomness of the allocation while maintaining balance between the groups. The inclusion criteria were as follows: (1) Adults aged 18–75 years who can independently complete self-reported psychological and sleep assessments; (2) first-time liver transplantation, as these patients experience higher levels of emotional and psychological stress related to the surgery and are thus more representative for studying post-transplant anxiety and depression; and postoperative consciousness with basic communication skills; and (3) able to perceive emotions linked to anxiety and depression and to describe sleeping conditions. The exclusion criteria were as follows: (1) suffering from other serious physical illnesses that may affect anxiety levels (eg, advanced cancer, heart disease); (2) a history of other mental disorders (eg, schizophrenia, bipolar disorder) or inability to understand and answer research questions; (3) prescribed and taking anti-anxiety or other medications during the study that may affect anxiety symptoms; (4) substance abuse (eg, alcohol, drugs) or a history/current symptoms of mental illness; or (5) unstable postoperative signs (eg, primary nonfunction, haemorrhage, vascular complications, biliary complications, metabolic complications, and renal insufficiency). The suspension criteria were as follows (consideration of participant safety; it was not deemed appropriate for the participant to continue the study): (1) voluntary withdrawal; (2) experiencing a serious adverse event during the study, such as a serious drug adverse effect or physical impairment; (3) loss of contact with the study team or unavailable for follow up; (4) severe illness deterioration during the study period, inability to continue participation in the study or inability to assess anxiety scores; and (5) ethical regulations or ethical requirements of the study protocol were violated by the participant during the study. The study was approved by the hospital’s ethics committee (Ethics Archive Number: LL-2023-135-K) and all patients who participated in the study provided informed consent. The clinical study registration number is CHiCTR1900024561.
The R 4.2.1 (Beijing, China) package was used for sample estimation and power analysis and employed the following settings: target power=0.90; alpha=0.15; group allocation equal (N1=N2); experience difference δ=1; standard deviation σ=1.5; N1=N2=34; dropout rate=15%; N1’=N2’=40 and N’=80. Missing data were handled using simple imputation based on available values from the baseline and follow-up, which helped maximize data use while preserving result validity.
INTERVENTION AND CONTROL:
The intervention and control groups were treated by 2 nurses of the same age, with the same title and from traditional nursing programs. To ensure the competency of the nurses, all were trained on the intervention components (psychological care, pain management, postoperative care, rehabilitation) by senior specialists before the study began. Nurses were regularly assessed to ensure consistent implementation. Routine care practices, including nutritional therapy and skin care, followed standardized protocols to avoid any variations in care. The incidence of postoperative anxiety, depression, and sleep problems in patients after liver transplant in the control group and the intervention group were measured to assess the effectiveness of the nursing mode in the intervention group.
CONTROL GROUP:
Traditional care regimens were used, including routine monitoring of vital signs, attention to changes in condition, nutritional support, keeping the skin clean, preventing complications, and regular computed tomography (CT) examinations.
Electrocardiogram and oxygen saturation output were monitored postoperatively, and any changes in vital signs were closely observed to prevent critical symptoms. Body temperature was monitored closely, and a doctor was notified immediately if it exceeded 38°C, particularly if accompanied by chills, nausea, vomiting, diarrhea, or a rash. Concurrently, nursing staff paid attention to possible dangerous situations, such as excessive drainage flow, bleeding around the puncture point on the skin, and increased ecchymosis within 24–48 hours after the operation. Nutritional supportive therapy was given to the patients and their skin was kept clean, particularly where active and passive movement of the limbs occurred during bed rest, to prevent the occurrence of deep vein thrombosis, muscle atrophy, or joint contracture. Regular liver function review and abdominal CT examinations were performed to determine the status of postoperative recovery.
DATA COLLECTION:
Patients who underwent liver transplantation were divided into 4 different time periods: 0–60, 61–120, 121–180, and 181–360 days. Follow-up staff collected questionnaires in 4 time periods through door-to-door calls, telephone, or WeChat in the home or the hospital. The duration of the continuous intervention was 1 year. During these periods, the researchers and nurses used the double-blind trial method to ensure the objectivity of this study. During the 1-year follow-up period for data collection, all study participants were highly cooperative, and all data were acquired after issuing the questionnaire.
HAMILTON ANXIETY SCALE:
The Hamilton Anxiety Scale (HAMA) was developed by Hamilton in 1959 and is mainly used to assess the severity of anxiety symptoms in patients [14]. It measures both mental anxiety and somatic anxiety. The scale ranges from 0 to 4, with 0 indicating no anxiety symptoms and 4 indicating a concentration of anxiety symptoms. The total score is divided into the following intervals: >29 points (considered severe anxiety); >21 points (definite significant anxiety); >14 points (definite anxiety); >7 points (considered anxiety); and <7 points (no anxiety symptoms). According to Tang Yuhua et al [15], HAMA has good reliability and validity, with a reliability coefficient r of 0.93 for the total score assessment, 0.83 to 1.00 for each single symptom score, and 0.36 for the validity coefficient.
SELF-RATING DEPRESSION SCALE:
The Self-Rating Depression Scale was compiled by W.W. Zung to assess depression severity [16]. The scale contains 20 items divided into 4 factors: affective symptoms, somatic symptoms, psychomotor disorders, and psychological disorders. The answer options for each item are ‘no or little time’, ‘a small part of the time’, ‘considerable time’ and ‘the vast majority of the time’, which are recorded as 1–4 points, respectively. A total score of ≤52 is considered normal, 53–62 is considered mild depression, 63–72 is considered moderate depression, and ≥73 is considered severe depression. Correlation studies performed on SDS showed correlation coefficients >0.7 for all 20 items of the scale. The test-retest reliability of each item ranged from 0.730 to 1.000, and the Cronbach’s α coefficient ranged from 0.782 to 0.784, indicating that the reliability and validity of this scale were good [17].
PITTSBURGH SLEEP QUALITY INDEX:
The Pittsburgh Sleep Quality Index is used to evaluate sleep quality [18]. The scale has 7 factors: sleep quality, sleep onset time, sleep duration, sleep efficiency, sleep disturbance, hypnotic drugs used, and daytime dysfunction. Each factor is scored from 0 to 3. The total score on the scale is 0–21, and the score is negatively correlated with sleep quality. A score of 0–5 indicates good sleep quality, a score of 6–10 indicates average sleep quality, a score of 11–15 indicates fair sleep quality and a score of 16–21 indicates poor sleep quality. A study by Lu Taoying et al [19] showed that Cronbach’s α of this scale was 0.845, with high intrinsic consistency. The confirmatory factor analysis showed that the fit index χ2/df, square root of approximate error (RMSEA), non-norm fitting index (NNFI), comparative fitting index (CFI), and goodness-of-fit index (GFI) were 4.83, 0.09, 0.96, 0.98, and 0.97, respectively, indicating good validity [19].
The above questionnaires were translated into Chinese and administered by trained nurses during these follow-ups, with face-to-face interviews being prioritized. Telephone and WeChat interviews were used as alternatives when in-person visits were not possible, ensuring consistent application of the scale. The demographic and general clinical characteristics of the patients were also collected, including age, gender, marital status, education, place of residence, history of previous anxiety, history of previous depression, and type of liver disease.
STATISTICAL METHODS:
The data analysis was performed using SPSS 26.0 (IBM, Armonk, NY, USA) statistical software. First, continuous data were statistically described by mean±standard deviation (M±SD), and qualitative data were described by case number or percentage (%). Then, the
Results
BASELINE CHARACTERISTICS OF PARTICIPANTS:
During the 1-year follow-up period, all study participants were highly cooperative, and no participants were lost or suspended. The mean age of patients was 56.79 years in the intervention group and 57.34 years in the control group. Previous histories of anxiety and depression were 17.5% and 7.5%, respectively, in the intervention group, and 22.5% and 5.0%, respectively, in the control group. Patients with previous sleep disorders accounted for 15.0% in the intervention group and 17.5% in the control group. There were no significant differences in the baseline characteristics between the 2 groups (p≥0.05) (Table 1).
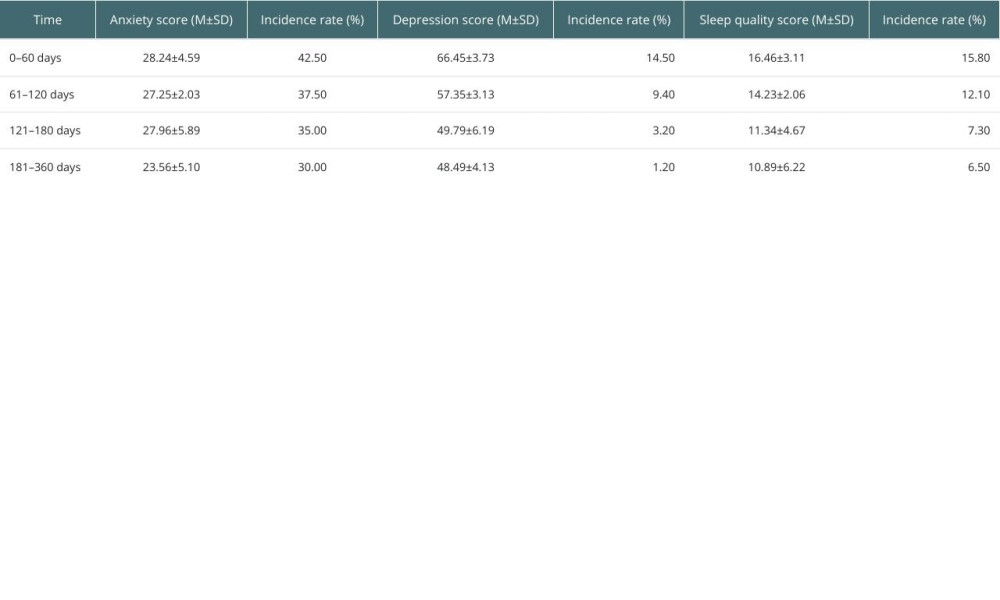
INCIDENCE OF ANXIETY, DEPRESSION, AND SLEEP DISORDERS AFTER LIVER TRANSPLANTATION:
The incidence of anxiety at 0–60, 61–120, 121–180, and 181–360 days following liver transplantation was 42.50%, 37.50%, 35.00%, and 30.00%, respectively. The incidence of depression was 14.5%, 9.4%, 3.2%, and 1.2%, respectively. The incidence of sleep disorders was 15.8%, 12.1%, 7.3%, and 6.5%, respectively (Table 2).
TIME AND INTERVENTION EFFECTS ON ANXIETY, DEPRESSION, AND SLEEP DISORDERS:
The results of the ANOVA for repeated-measures data showed that the anxiety and depression scores were lower in the intervention group than in the control group, and the difference was statistically significant (Fgroup=8.771, 16.821, p<0.001). Anxiety and depression scores gradually decreased in the intervention and control groups over time (Ftime=4.283, 9.278, p<0.05). The quality of sleep scores was lower in the intervention compared with the control group, the difference was statistically significant (Fgroup=8.166, p<0.001) and the quality of sleep scores gradually decreased over time (Ftime=10.827, p<0.001) (Table 3).
Discussion
LIMITATIONS:
This study has several limitations. First, the small sample size may limit the generalizability of the results and affect subgroup analyses. Larger, multi-center studies are needed for further validation. Second, while the study compared nursing interventions, it did not explore the underlying mechanisms of anxiety and depression, which future research could address. Additionally, missing data or attrition during follow-up may have influenced the results, and we did not apply methods like sensitivity analysis. Lastly, the scales used only measure symptom severity, not clinical diagnoses, so the reported prevalence of anxiety and depression should be interpreted with caution.
Conclusions
Compared with traditional care programs, relevant nursing strategies can effectively reduce the occurrence of anxiety, depression, and sleep disorders in patients undergoing liver transplantation and improve their quality of life. Healthcare professionals should focus on the psychological and physical well-being of patients, provide personalized nursing care, and strengthen mental health education post-transplant. This can help improve patients’ understanding of their condition, enhance coping abilities, reduce anxiety, and support physical recovery. Future research should explore the mechanisms of post-transplant anxiety, refine interventions, and consider strategies to address missing data and sample size limitations. Clinically, a comprehensive, patient-centered care model should be adopted to promote long-term well-being and recovery following liver transplantation.
Data and Code Availability
Data related to the study were not stored in a publicly available repository. Data will be made available on request.


References
1. Biyyala D, Joseph R, Varadharajan N, Incidence and prevalence of depressive, anxiety, and insomnia symptoms among adult liver transplant recipients: A systematic review and meta-analysis: Gen Hosp Psychiatry, 2023; 80; 26-34
2. Li T, Zhang QQ, Li H, Influence of stage 1 exercise rehabilitation combined psychological intervention on anxiety and depression in patients after CABG: Chinese Journal of Cardiovascular Rehabilitation Medicine, 2022; 31(3); 270-74
3. Li XN, Shen CY, Lin T, Effect of mindfulness training on anxiety and depression levels and sleep quality in patients after liver transplantation//Nanjing Society of Rehabilitation Medicine: Proceedings of the Sixth National Academic Exchange Conference on Rehabilitation and Clinical Pharmacy (III), 2023; 6; 087167
4. Mendes KDS, Relevance of anxiety and stress levels on sleep quality after liver transplantation: Transplant Proc, 2014; 46(6); 1822-26
5. Yeung KS, Hernandez M, Mao JJ, Herbal medicine for depression and anxiety: A systematic review with assessment of potential psycho-oncologic relevance: Phytother Res, 2018; 32(5); 865-91
6. Fluharty M, Taylor AE, Grabski M, Munafò MR, The association of cigarette smoking with depression and anxiety: A systematic review: Nicotine Tob Res, 2017; 19(1); 3-13
7. Götze H, Friedrich M, Taubenheim S, Depression and anxiety in long-term survivors 5 and 10 years after cancer diagnosis: Support Care Cancer, 2020; 28(1); 211-20
8. Marroni CA, Fleck AM, Fernandes SA, Liver transplantation and alcoholic liver disease: History, controversies, and considerations: World J Gastroenterol, 2018; 24(26); 2785-805
9. Albayrak B, Ozcan H, Aksungur N, Cankaya E, Depression and anxiety symptoms in patients with cirrhosis: A prospective study before and after liver transplantation: Transplant Proc, 2023; 55(7); 1644-48
10. Lu HF, Gu HF, Investigation of bedtime delay, depression and anxiety in donor liver transplantation and analysis of influencing factors: Liver, 2023; 28(07); 827-32
11. Chen Y, Effects of mindfulness training on anxiety and depression level and sleep quality in patients after liver transplantation: Nursing Practice and Research, 2017; 14(13); 134-36
12. Wang X, Zhang WJ, Xue GH, Methods and experience of psychological nursing for patients after liver transplantation: Psychological Monthly, 2022; 17(20); 159-61
13. Zhao WF, Guo ZL, Guo J, Application of standardized work flow under ERAS concept in patient nursing after liver transplantation: Chinese Evidence-Based Nursing, 2022; 8(2); 267-70
14. Thompson E, Hamilton Rating Scale for Anxiety (HAM-A): Occup Med (Lond), 2015; 65(7); 601
15. Tang YH, Zhang MY, Hamilton Depression Scale (HAMD): Shanghai Psychiatric Journal, 1984(2); 61-64
16. Zung WW, A Self-Rating Depression Scale: Arch Gen Psychiatry, 1965; 12; 63-70
17. Yuan G, Zhao J, Zheng D, Liu BY, Study on distinguishing the severity of depression with Self-Rating Depression Scale and Beck Depression Inventory: Journal of Neuroscience and Mental Health, 2021; 21(12); 868-73
18. Zitser J, Allen IE, Falgàs N, Pittsburgh Sleep Quality Index (PSQI) responses are modulated by total sleep time and wake after sleep onset in healthy older adults: PLoS One, 2022; 17(6); e0270095
19. Lu TY, Li Y, Xia P, Analysis on reliability and validity of the Pittsburgh Sleep Quality Index: Chongqing Medicine, 2014; 43(3); 260-63
20. Jin YX, Liu J, Xuan FF, Lu JF, Application of the concept of accelerated rehabilitation surgery in the nursing of liver transplantation: Zhejiang Medical, 2023; 45(13); 1431-37
21. Yıldız E, The relationship between anxiety and intolerance of uncertainty levels in individuals who received liver transplant: A descriptive cross-sectional study: Clin Nurs Res, 2021; 30(5); 548-57
22. Zhang BL, Construction of nursing quality evaluation index system and primary application of index monitoring after adult liver transplantation: Qingdao University, 2022; 2022; 000105
23. Gu YM, Zhang LL, Guo HM, Effects of comprehensive nursing mode on postoperative mental symptoms of patients with liver transplantation: Chinese Nursing Research, 2022; 36(16); 2988-91
24. Krenzien F, Krezdorn N, Morgül MH, The elderly liver transplant recipients: Anxiety, depression, fatigue and life satisfaction: Z Gastroenterol, 2017; 55(6); 557-63
25. Zhang ZM, Nursing intervention of diet after liver transplantation: Chinese Journal of Woman and Child Health Research, 2017; 28(S4); 252-53
26. Han LQ, Shen MY, Progress in emotion related symptom cluster assessment and non-drug intervention in adult liver transplant recipients: Nursing Research, 2024; 38(13); 2318-22
27. Gao JH, Guo Y, Progress in sleep disorders in liver transplant recipients: Nursing Research, 2022; 36(2); 280-84
28. Lu WQ, Lu HF, Ren XF, Effect of laparoscopic liver donor acquisition on quality of life after living donor liver transplantation in children: Chinese General Practice Nursing, 2022; 20(14); 1877-80
29. Stine JG, Stukenborg GJ, Wang J, Liver transplant candidates have impaired quality of life across health domains as assessed by computerized testing: Ann Hepatol, 2020; 19(1); 62-68
30. Stewart KE, Hart RP, Gibson DP, Fisher RA, Illness apprehension, depression, anxiety, and quality of life in liver transplant candidates: Implications for psychosocial interventions: Psychosomatics, 2014; 55(6); 650-58
In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988