17 July 2020: Original Paper
Kidney Transplantation and “Sex Mismatch”: A 10-Year Single-Center Analysis
Karol Graňák1ABCDE, Lea Kováčiková1ABC, Petra Skálová1AB, Matej Vnučák1BDE, Juraj Miklušica1ABCD, Ľudovít Laca1ABC, Marián Mokáň2FG, Ivana Dedinská1ACEF*DOI: 10.12659/AOT.921117
Ann Transplant 2020; 25:e921117






Abstract
BACKGROUND: The effect of a relative disproportion in the size of a transplanted kidney (KT) on graft function and survival is well documented. However, the importance of the H-Y antigen (male donor and female recipient) has not been unambiguously confirmed.
MATERIAL AND METHODS: Our retrospective analysis consists of 230 deceased donor/recipient pairs. The aim of the study was to determine the effect of sex mismatch between donors and recipients on the function of the graft and the graft and patient survival.
RESULTS: In the group of male donors, a statistically significantly lower value of the eGFR (estimated glomerular filtration rate) was recorded for female recipients in the fifth year after the KT (=0.0047). The male donor/female recipient group was an independent risk factor for: eGFR (<60 ml/min (CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration) in the third year after KT [HR 0.1618; (P=0.0004)], acute rejection in the first year after KT [HR 1.8992; (P=0.0387)], and the 5-year graft survival was significantly worse in this group. By adjusting the results for age and induction, this group was at significantly higher risk for decreased graft function (eGFR <30 ml/min) if the age of the donor was ≤50 years old and the recipient was >45 years old in the fifth year [HR 11.1676; (P=0.0139)], the age of the donor was ≤50 years old/recipient was ≤45 years old in the third year [HR 1.2500; (P=0.0050)], and also in the fifth year after KT [HR 8.1993; (P=0.0183)].
CONCLUSIONS: Based on our analysis, the differences in the incidence of acute rejection episodes as well as in graft survival among the different groups of patients were confirmed. The group with the highest risk, in cases of an acute rejection episode, is a male donor/female recipient.
Keywords: Gender Identity, Graft Survival, Kidney Transplantation, Delayed Graft Function, Graft Rejection, H-Y Antigen, Renal Insufficiency, Chronic, Risk Factors, Tissue Donors
Background
Due to the current lack of organ donors, the system of kidney allocation does not take into account the sex differences between the donor and the recipient. A large percentage of patients included in the waiting list (WL) for kidney transplantation (KT) consists of men, despite the fact that women suffer more from chronic kidney disease [1]. More than 60% of men were active on a WL in the USA at the end of 2017; this percentage correlated with the number of transplanted male patients [2]. Data from European countries are almost identical [3]. In the case of transplantations from living donors, women form almost two-thirds of the kidney donor pool, but men are more often the recipients [2].
“Sex-specific medicine”, as the science of sex and gender difference, gives us the option to see how a disease can show itself differently in males and females, and how the disease can have different a pathophysiological basis, a different reaction to the administered treatment, or a different ability to cope with the disease in males and females [1]. The influence of sex, as one of the still growing number of factors, on the process of effective kidney transplantation has been a subject of study for a long time. A female kidney is generally smaller with a smaller mass of nephrons, which might lead to hyperfiltration, a reduction of the nephron mass, or even a loss of the graft function on the basis of chronic renal graft nephropathy [4]. On the other hand, a smaller body surface leads, in the case of women, to a lower metabolic impact on the kidney, which represents an advantage in graft survival [5]; these are non-immunological factors. Immunity responses, both humoral and cellular, are activated in the female body to a larger degree due to the immunity-stimulating effect of oestrogens and the suppressive impact of androgens [6,7]. The significance of a sex-determined minor histocompatibility antigen (H-Y antigen) was described for the first time in 1976 in the case of a women who rejected bone marrow from her HLA-identical brother [8]. Its recognition by the immunity system of the female recipient of a male kidney can result in a higher risk of the loss of graft function. During recent years, the highest number of H-Y antibodies was detected in the blood of female recipients who received a kidney from a male donor, as compared to other sex combinations. The occurrence of these antibodies is significantly correlated with the occurrence of acute rejection [9]. Recently, the association of sex difference on the development of post-transplant diabetes mellitus (PTDM), a complication with a significant negative impact on morbidity and mortality of patients after KT, was confirmed [10]. In addition to the sex of the donors and recipients, the age category of both patient groups also plays a crucial role. Immunity system activity and behavior of the individual are both affected by sex and gender and by a person’s age and maturity [11]. The compliance of the patient after a KT and the adherence to immunosuppression therapy influence the occurrence of rejection and survival of the graft after a KT [12]. The influence and significance of these factors also depends on the sex and age of the recipient [13,14]. So far there was only one analysis that dealt with the current impact of the different sex and age category of donors and recipients on graft survival after a KT [11]; the majority of the published studies assessed the relationship between these factors and the graft survival in isolation.
The aim of our extensive study was to determine the influence of sex mismatch between the donor and the recipient on graft function, graft survival, and patient survival after a KT. Another aim was to identify the impact of a sex mismatch on the function and the survival of graft and patient after a KT adjusted to the age category of the donors/recipients and the induction of treatment with thymoglobulin.
Material and Methods
The present 10-year retrospective analysis consists of 230 deceased donors after brain death-recipient pairs who underwent a primary KT from a dead donor in the Martin Transplant Center from 2003 to 2013.
For all donors before procurement we determined: age at time of procurement, sex of donor, type of donor (percentage of donors with extended criteria), eGFR (estimated glomerular filtration rate) before procurement determined by CKD-EPI formula (Chronic Kidney Disease Epidemiology Collaboration), body mass index (BMI), and proteinuria for 12 hours. Good graft function was defined as eGFR above 60 ml/min according to KDIGO definition for chronic kidney disease [15].
For the recipients we recorded: age at time of KT, sex, time of cold ischemia, start of graft function (primary or delayed – defined as the need of dialysis treatment in the first week after the KT), occurrence of acute rejection in the first year after KT verified by biopsy, the type of induction (IL-2 inhibitor–basiliximab/daclizumab or anti-thymocyte globulin), and maintenance of immunosuppression treatment (tacrolimus or cyclosporine A). The graft function was determined on the basis of the serum creatinine on the seventh day (D7), first, third, sixth month (M), first, third, fifth year (Y), and the value of the eGFR in M1, M3, M6, Y1, Y3, and Y5 after the KT (Table 1). Methylprednisolone 500 mg was administered to all recipients before transplantation and on D1. Anti-thymocyte globulin was used for high-risk patients (panel-reactive antibody >20%) or those with history of positive cross-match test or PRA less than 20% with cold ischemia time more than 12 hours, and extended-criteria donors. We used anti-thymocyte globulin in a cumulative dose of 3.5 mg/kg, divided into 3 doses). Basiliximab was used in low-risk patients (PRA less than 20%, cold ischemia time less than 12 hours, standard-criteria donor). No induction was used for patients with very low risk (maximum of one mismatch and a 0% panel-reactive antibody). Tacrolimus or cyclosporine A in combination with mycophenolic acid and corticosteroids were used in the maintenance of immunosuppression.
Patients/recipients were divided into 2 groups according to donor sex. Furthermore, we identified each group of male and female recipients by age at CT.
We used a certified statistical program, MedCalc version 13.1.2. (MedCalc Software VAT registration number BE 0809 344 640, member of the International Association of Statistical Computations, Ostend, Belgium). Comparison of continuous variables between groups was performed using parametric (t-test) or non-parametric (Mann-Whitney) tests; associations between categorical variables were analyzed using chi-square test and Fisher’s exact test, as appropriate. We identified independent risk factors for acute rejection and reduced graft function using the Cox proportional risk model tailored to the age category of donors, recipients, and induction therapy with anti-thymocyte globulin. P <0.05 was considered statistically significant.
Ethics approval: All procedures involving human participants were approved in accordance with the ethical standards of the Institutional and/or National Research Committee, including the Helsinki Declaration of 1964 and its subsequent amendments or comparable ethical standards.
The reported clinical and research activities are in line with the principles of the Istanbul Declaration as set out in the Istanbul Declaration on Organ Trafficking and Transplant Tourism.
Results
UNIVARIATE ANALYSIS:
The group of donors (n=230) consisted of significantly more men (n=162) than women (n=68). The average age of the donors was 45±15.3 years old. We determined in the group of female donors, a significantly lower value of creatinine in the third, sixth month, first and third year after KT if the recipient was a woman, but the eGFR was without any statistically significant difference (Figure 1). In the group of male donors, a statistically significantly lower value of the eGFR was recorded for female recipients in the fifth year after the KT (P=0.0047) with a significantly lower value of creatinine in M1, M3, M6, Y1 and Y5 after KT, Figure 2.
The group of recipients (n=230) consisted of 154 men and 76 women. The average age of the recipients was 47.4±11.6 years old (Table 1). Tables 2 and 3 show basic characteristics in all groups of recipients (separately for female donors and male donors).
There was no significant difference in induction among recipients in the group of male donors, but we recorded significantly lower percentages of female recipients with anti-thymocyte globulin induction in male donors and significantly lower average PRA in this group of recipients, which means that these female recipients were not at high immunological risk at the beginning (Table 3).
END-POINT: GOOD GRAFT FUNCTION (EGFR >60 ML/MIN PURSUANT TO CKD-EPI): We identified independent protective factors contributing to the development of good graft function in the first year after KT: the eGFR of the donor at the time of procurement above 60 ml/min [HR 6.0955; (P<0.0126)] and induction with thymoglobulin [HR 2.0532; (P<0.0044)] (Table 4). The protective effect of thymoglobulin continues in the third year [HR 7.1777; (P<0.0001)], as well as in the fifth year after KT [HR 4.7703; (P=0.0001)]) (Tables 5, 6). On the other hand, independent risk factors include the eGFR of the donor at the time of procurement 30–59 ml/min [HR 0.1148; (P=0.0028)], induction of IL-2 with an inhibitor [HR 0.5489; (P=0.0196)], and acute rejection in the first year after KT [HR 0.3421; (P=0.0229)] (Table 4). We confirmed that the third year after KT is an independent risk factor for the graft function of the sex mismatch in the male donor/female recipient [HR 0.1618; (P=0.0004)] and acute rejection in the first year after KT [HR 0.3099; (P=0.0019)] (Table 5). The male donor/female recipient combination [HR 0.1282; (P<0.0001)], acute rejection in the first year after KT [HR 0.3942; (P=0.0008)], and induction with an IL-2 inhibitor [HR 0.4347; (P<0.0001)] are risk factors for graft function in the fifth year after KT (Table 6).
END-POINT: SIGNIFICANTLY REDUCED GRAFT FUNCTION (EGFR <30 ML/MIN PURSUANT TO CKD – EPI): We stipulated risk factors for the development of significantly reduced graft function (eGFR <30 ml/min) adjusted to the age category of donors and recipients and induction treatment with anti-thymocyte globulin in Y1, Y3, and Y5. We did not identify any significant differences from the perspective of sex in monitored years in the age category donor >50/recipient >45. We determined that the female donor/male recipient combination in the age category donor >50/recipient ≤45 years was a significant risk factor for reduced graft function in Y1 [HR 2.0626; (P=0.0264)], Y3 [HR 3.0451; (P=0.0315)] and Y5 [HR 5.8214; (P=0.0312)] (Figure 3).
In the group donor ≤50/recipient >45 years, a significant negative predictor is acute rejection [HR 3.8872; (P=0.0119)] and the eGFR of the donor at the time of procurement ≤60 ml/min [HR 3.4870; (P=0.0481)] in Y1; from the perspective of sex, there was significantly worse graft function in the case of male donor/female recipient combination, especially in Y5 [HR 11.1676; (P=0.0139)] (Figure 4). Similarly, this type of sex mismatch represents a risk of significantly reduced graft function in the age category donor ≤50/recipient ≤45 years in Y3 [HR 1.2500; (P=0.0050)] and in Y5 [HR 8.1993; (P=0.0183)]; the eGFR of the donor at the time of procurement ≤60 ml/min is a significant negative predictor in this age category in Y1 [HR 6.8874; (P=0.0172)] and in Y3 [HR 7.6859; (P=0.0347)] (Figure 5).
END-POINT: ACUTE REJECTION IN THE FIRST YEAR AFTER KT: Delayed graft function [HR 1.9845; (P=0.0495)] and sex mismatch type male donor/female recipient [HR 1.8992; (P=0.0387)] were independent risk factors for the occurrence of acute rejection in the first year after KT. Induction with thymoglobulin significantly reduces the risk of acute rejection development in the first year after KT [HR 0.2108; (P=0.0033)] (Table 7).
AGE CATEGORY (25–44, ≥45): We divided patients/recipients into 2 groups according to the donor’s sex. We identified each group of male and female recipients according to the age at the time of the KT and we found significantly worse graft function in the male donor/female recipient combination in the age category ≥45 years in the third (P=0.0025) and fifth year after KT (P=0.0005). No significant differences were found in female donors (Figure 6).
GRAFT AND PATIENT SURVIVAL: Figures 7 and 8 show the total 1-, 3-, and 5-year graft and patient survival after KT. A significantly worse 5-year graft survival was shown in the male donor/female recipient combination (P=0.0047). The survival of patients in these years was only numerically worse.
Discussion
The development of graft function and graft survival after KT depends on the sex of the donor and the age at the time of transplantation.
We found that the sex mismatch type of male donor/female recipient had the highest risk group graft function in the third and fifth year after KT. Studies examining the issues of sex matching and its impact on graft survival after KT agree with our conclusions [4,8,16]. Our univariate analysis showed a significantly lower EFR in this group in the 5-year monitoring, despite significantly lower values of creatinine, when compared to the male recipients. The male donor/female recipient combination in the multivariate analysis independently reduces the occurrence of good graft function (eGFR >60 ml/min) in the third and fifth year after KT. We did not find any significant effect of sex on graft function in the early post-transplant period. This mismatch leads to a significantly higher occurrence of acute rejection in the first year after KT, although this group had lower immunological risk according to the induction treatment used (significantly lower percentage of patients with anti-thymocyte globulin induction with significantly lower average PRA). The most important conclusion of our analysis was the finding that women showed a significantly lower 5-year survival of the graft in the case of a kidney allocation from a male donor. We assume that these conclusions have an immunological basis. Tan et al. confirmed a significantly higher occurrence of antibodies against H-Y antigens in female recipients who received the kidney from a male donor; this fact is strongly correlated with the occurrence of acute rejection after KT [9]. The significant impact of H-Y antibodies on the failure of graft function is documented by Gratwohl et al. on a sample of more than 190 000 recipients from dead kidney donors in the first and subsequent second to tenth year after KT [8]. McGee et al. discussed the impact of BMI and the size of the donor’s kidney, when the negative impact of sex mismatch is significantly reduced by a relatively higher value of BMI of the donor as compared to the recipient. BMI is reported to be correlated with kidney size [16]. Many analyses have confirmed the indisputable significant impact of non-immunological factors (such as the graft size) on the function of the transplanted kidney [4,17,18]. An important finding in our analysis was the strong dependence of the development of good graft function in the monitored years on the type of induction used (protective effect of anti-thymocyte globulin, IL-2 inhibitor as an independent risk factor). We also think it is very important, when evaluating the effect of sex on the graft function, to evaluate it in combination with age, as the impact of both immunological and non-immunological factors is diversely represented in the body during life. We have, therefore, adjusted the analysis to the induction with anti-thymocyte globulin and age categories of donors and recipients.
We found that the mentioned risk of the male donor/female recipient combination represents a significantly higher risk of significantly reduced graft function (eGFR <30 ml/min) in the case of a kidney allocation between younger individuals (donor ≤50 years, recipient ≤45 years) in the third and fifth year after KT. Lepeytre et al. found that the combined effect of age and sex on graft function led to a worse graft outcome in women in all age categories if the donor was male. The outcome was significantly worse in the category of 15–24 years old, even without any effect from the sex of the donor [11]; it is especially evident in younger individuals, probably due to the effect of sex-determined H-Y antigens, with higher sensitising of female recipients. The effect of the genital system plays an important role, as it reaches the peak of its activity in this period, affecting immunity responses of the body. The immunosuppressive effect of testosterone and the immunomodulatory effect of estrogens are well described in the literature [6,7,19]. We found that the same combination of sexes (male donor/female recipient) has a significant negative effect on graft function in donor ≤50 years and recipient >45 years, but only in the late post-transplant period – Y5. This result is a little surprising, as a younger male kidney should provide the female recipient with a functional and structural advantage, with a smaller metabolic impact of the body. Also, the power of sex and immunity determinants should gradually decrease with age, but we cannot ascribe a zero effect to it with any certainty.
We did not record any impact of the mismatch on the development of significantly reduced graft function in a higher age category (donor >50 years, recipient >45 years). The effect of sex hormones on the immunity system gradually weakens until it disappears completely in older women, especially after menopause [20], which we considered to be the main reason for this finding.
Kidneys from older donors have a smaller functional mass of nephrons, which over the course of life gradually reduces with growing nephrosclerosis [21,22], and they have less ability to adequately respond to physiological and pathological changes and thus lead to a quicker reduction of renal reserves [23]. Tan et al. compared the functionality and structure of kidneys in donors >55 years and <40 years and found a significantly lower number of functional glomeruli with a significantly higher sclerotization in “older” donors [24]. In our analysis, a clearly high-risk combination for the significant reduction of graft function was the female donor/male recipient combination in the group of younger recipients (≤45 years) who were transplanted with an older kidney (donor >50 years), and that applied in all the monitored years. We consider this result to be expected and logical. In this case, an important role is played by the mismatch in graft size, as smaller and older kidneys cannot adequately meet the metabolic demands of the recipient.
From the perspective of sex, we consider the male donor/female recipient combination to be the combination with the highest risk. At the same time, it is important to associate the differences in sex with the age of the donors and recipients as well as the type of induction immunosuppression. It should be noted that there are also other factors not included in our study that have an impact on the function and survival of the graft after KT, including mismatch in the size of the transplanted kidney and in the BMI, with a different metabolic impact.
Conclusions
Based on our analysis, we confirmed that sex differences between the donor and the recipient have a significant effect on graft function, graft survival, and occurrence of acute rejection after KT. It is not possible to take these factors into account for kidney allocation in clinical practice due to the persisting shortage of organ donors. However, the sex mismatch should be the subject of interest in the post-transplant period in the sense of the thorough monitoring of these pairs by taking preventive measures such as a protocolar biopsy or the determination of donor-specific antibodies to prevent the development of acute rejection or early graft failure.
Figures
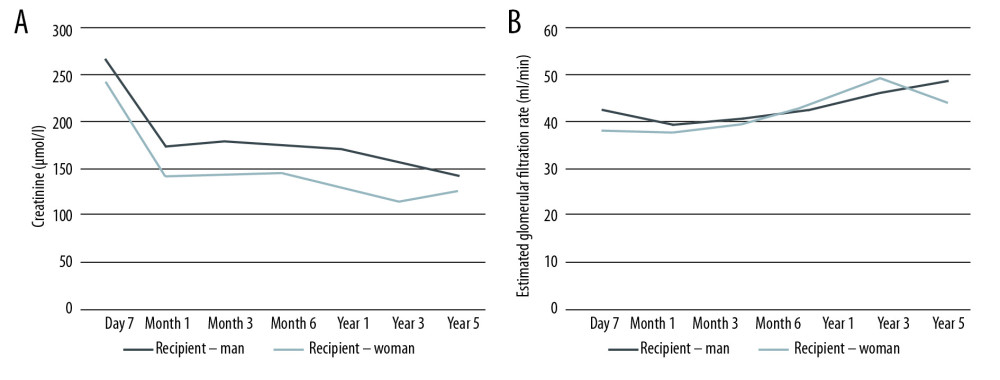 Figure 1. Development of the value of creatinine (A) and the eGFR (B) over time (donor – woman).
Figure 1. Development of the value of creatinine (A) and the eGFR (B) over time (donor – woman). 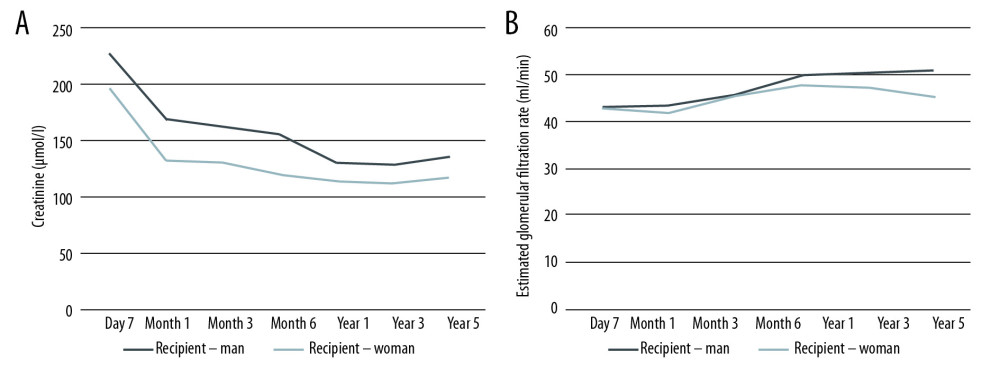 Figure 2. Development of the value of creatinine (A) and the eGFR (B) over time (donor – man).
Figure 2. Development of the value of creatinine (A) and the eGFR (B) over time (donor – man). 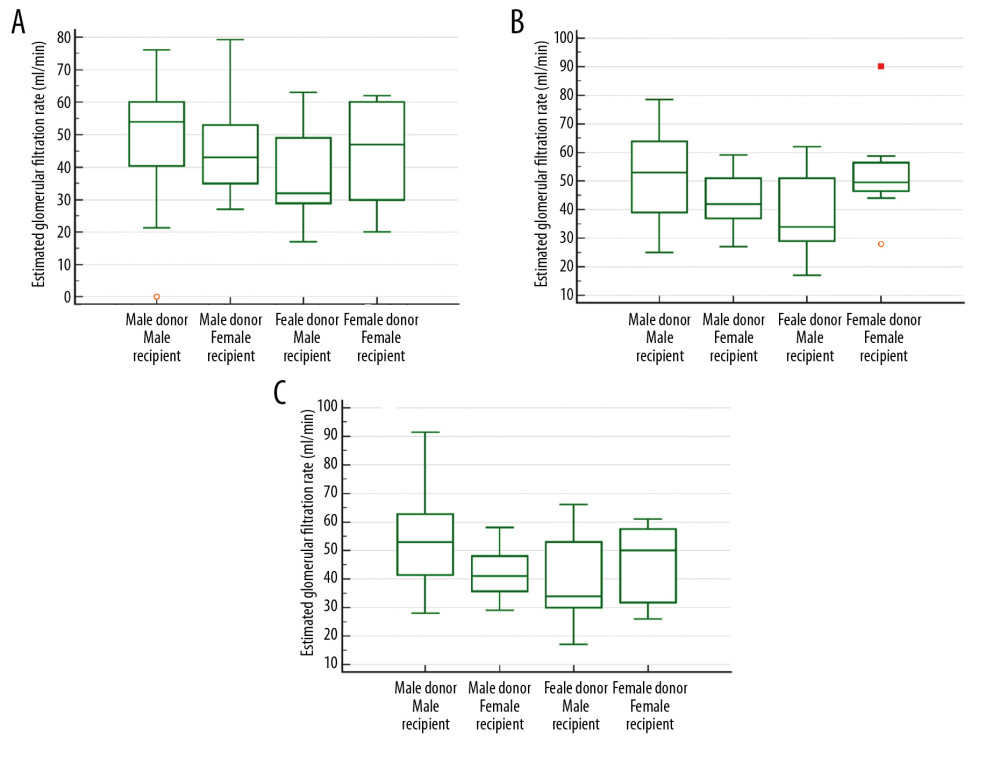 Figure 3. The eGFR in year 1 (A), year 3 (B) and year 5 (C) after kidney transplantation (donor >50 years old, recipient ≤45 years old).
Figure 3. The eGFR in year 1 (A), year 3 (B) and year 5 (C) after kidney transplantation (donor >50 years old, recipient ≤45 years old). 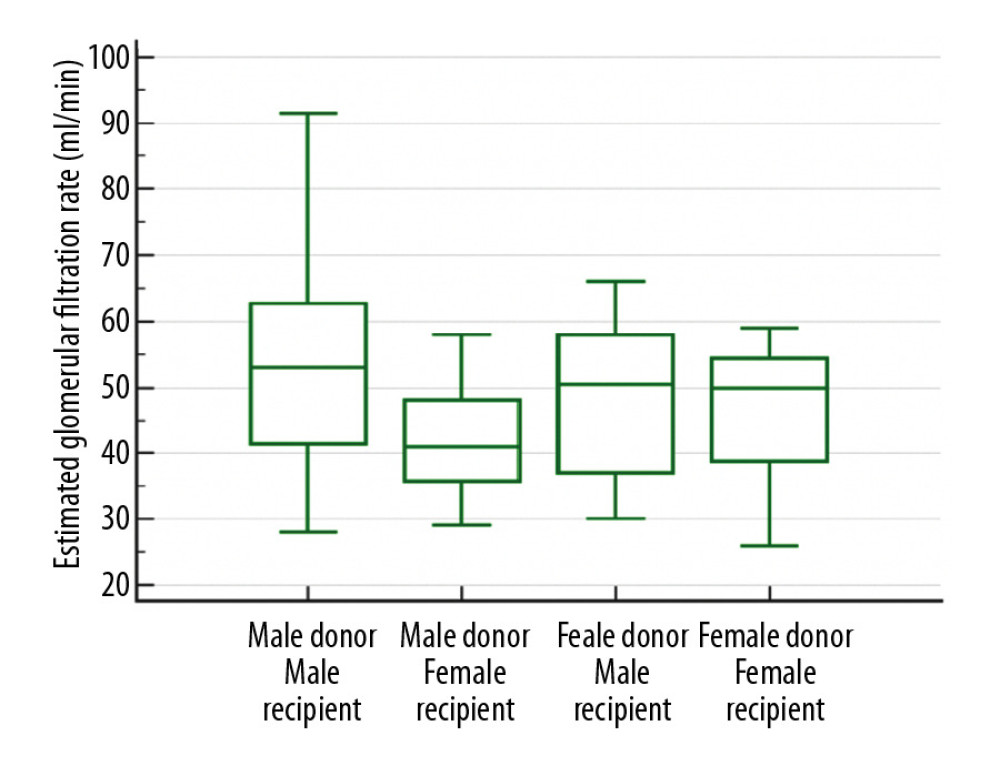 Figure 4. The eGFR in year5 after kidney transplantation (donor ≤50 years old, recipient >45 years old).
Figure 4. The eGFR in year5 after kidney transplantation (donor ≤50 years old, recipient >45 years old). 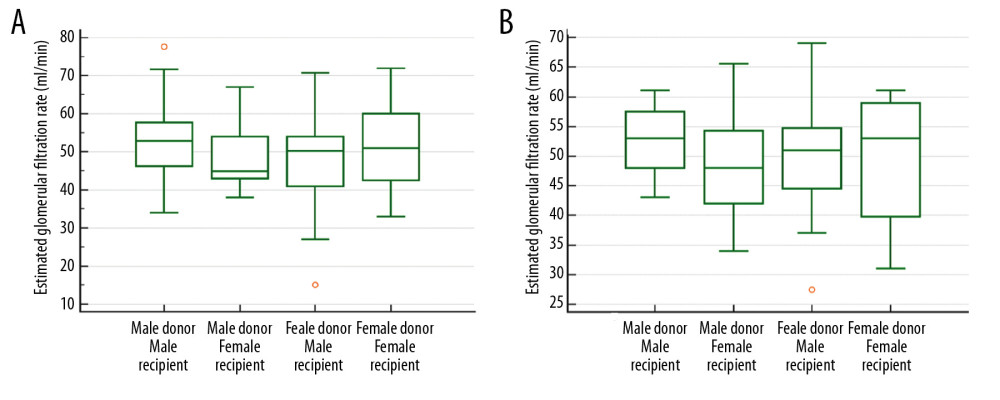 Figure 5. The eGFR in year 3 (A) and year5 (B) after kidney transplantation (donor ≤50 years old, recipient ≤45 years old).
Figure 5. The eGFR in year 3 (A) and year5 (B) after kidney transplantation (donor ≤50 years old, recipient ≤45 years old). 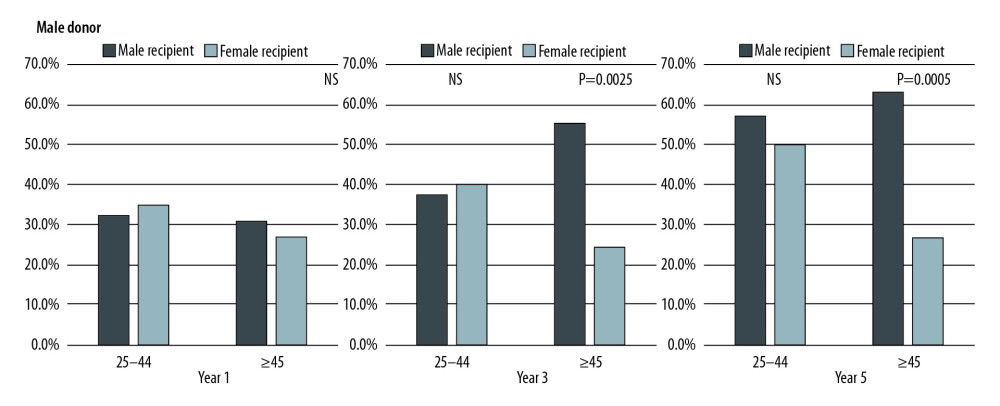 Figure 6. The eGFR in year 1, year 3, and year 5 after kidney transplantation (displays the percentage of patients with an eGFR >60 ml/min).
Figure 6. The eGFR in year 1, year 3, and year 5 after kidney transplantation (displays the percentage of patients with an eGFR >60 ml/min). 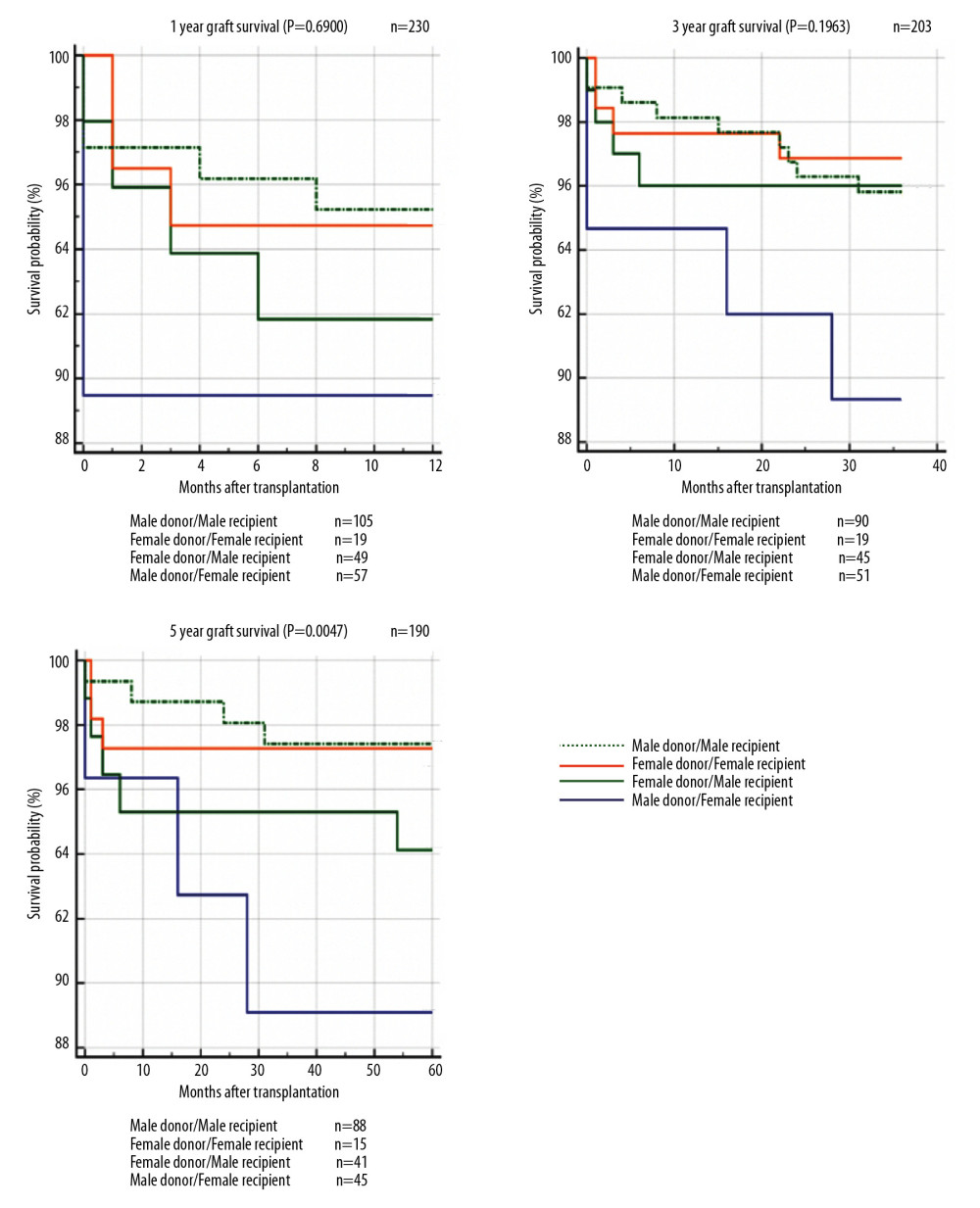 Figure 7. The 1-year, 3-year, and 5-year graft survival after kidney transplantation.
Figure 7. The 1-year, 3-year, and 5-year graft survival after kidney transplantation. 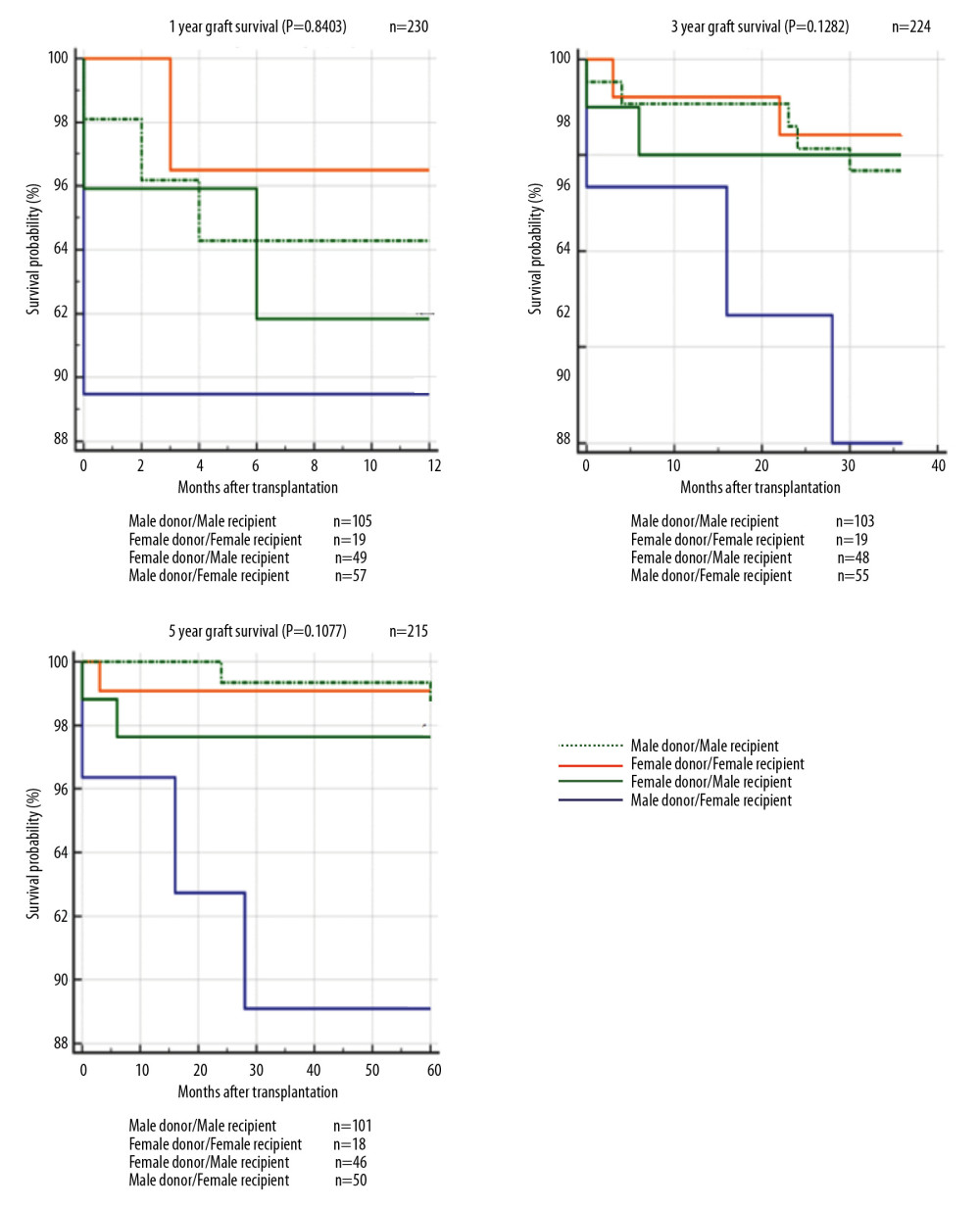 Figure 8. The 1-year, 3-year, and 5-year patient survival after kidney transplantation.
Figure 8. The 1-year, 3-year, and 5-year patient survival after kidney transplantation. Tables
Table 1. Group characteristics.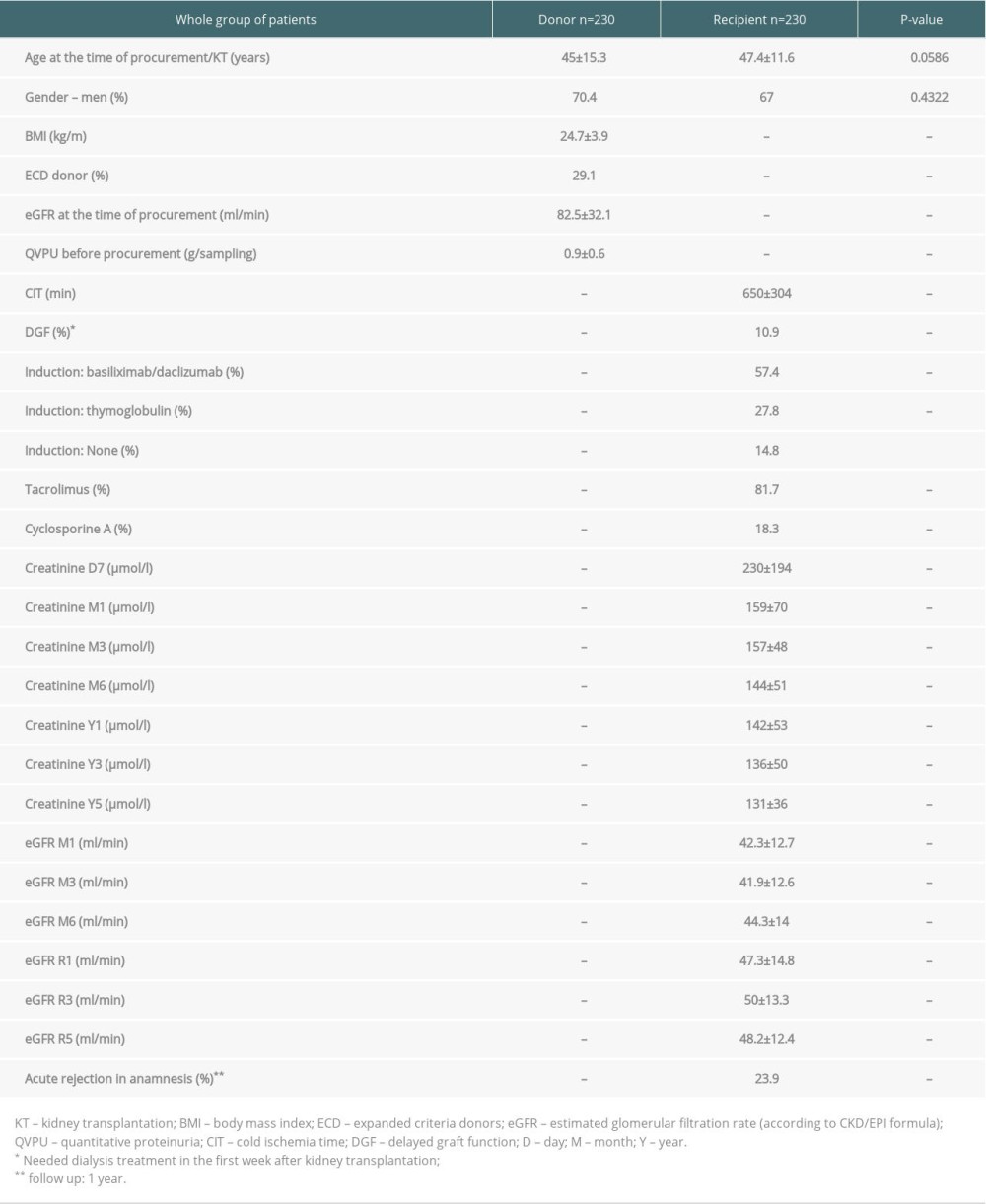 Table 2. Group characteristics – female donor.
Table 2. Group characteristics – female donor.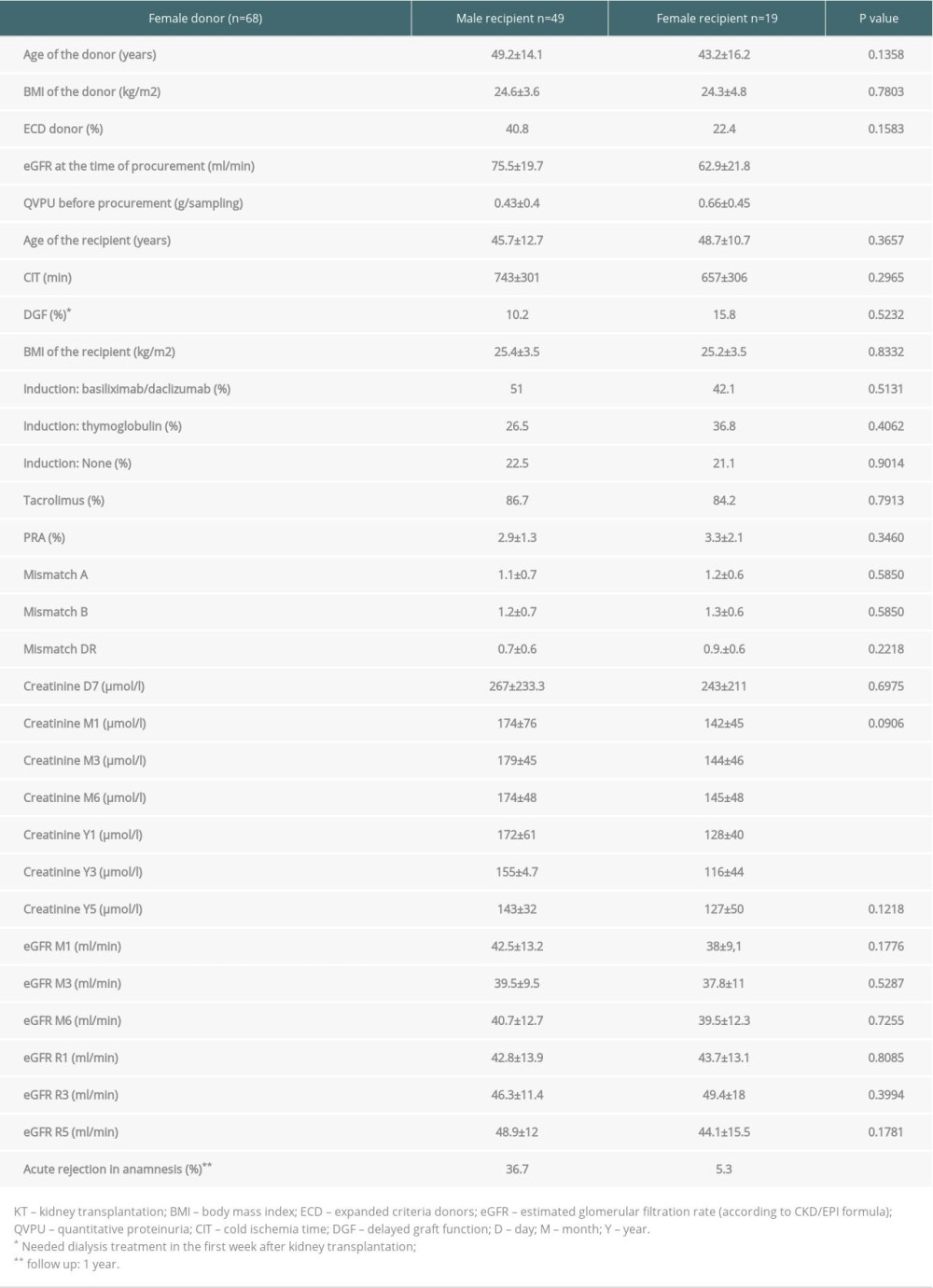 Table 3. Group characteristics – male donor.
Table 3. Group characteristics – male donor.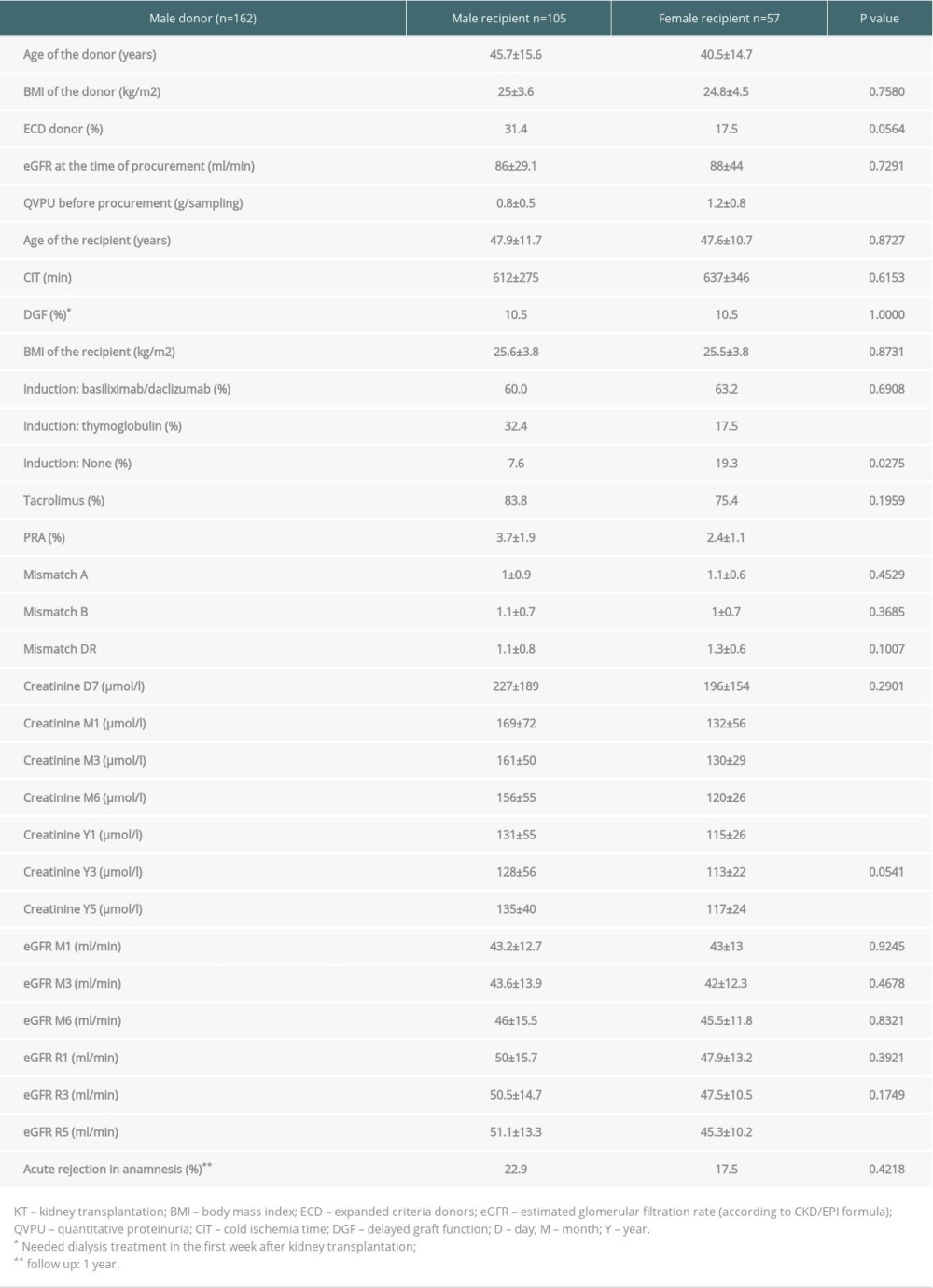 Table 4. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 1st year after KT).
Table 4. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 1st year after KT).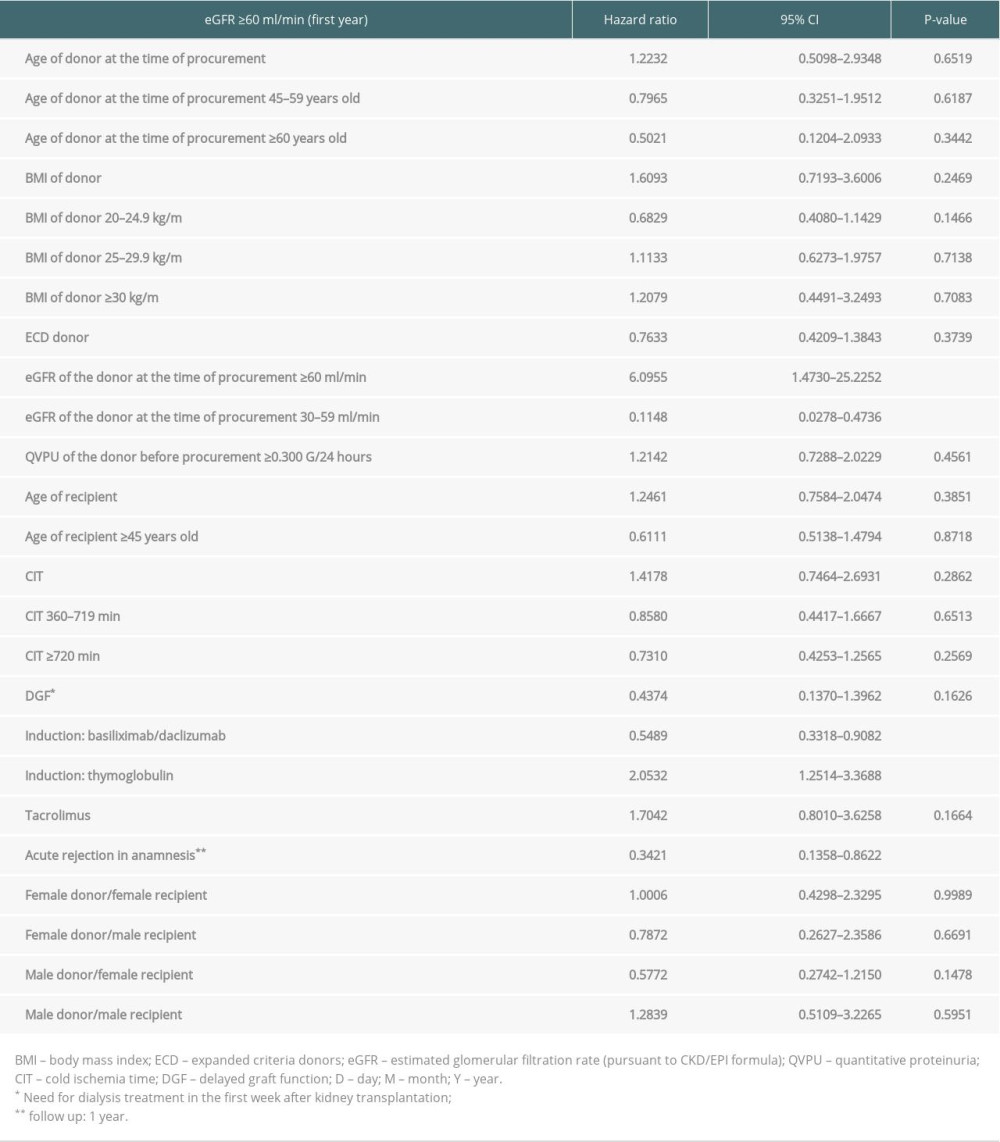 Table 5. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 3rd year after KT).
Table 5. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 3rd year after KT).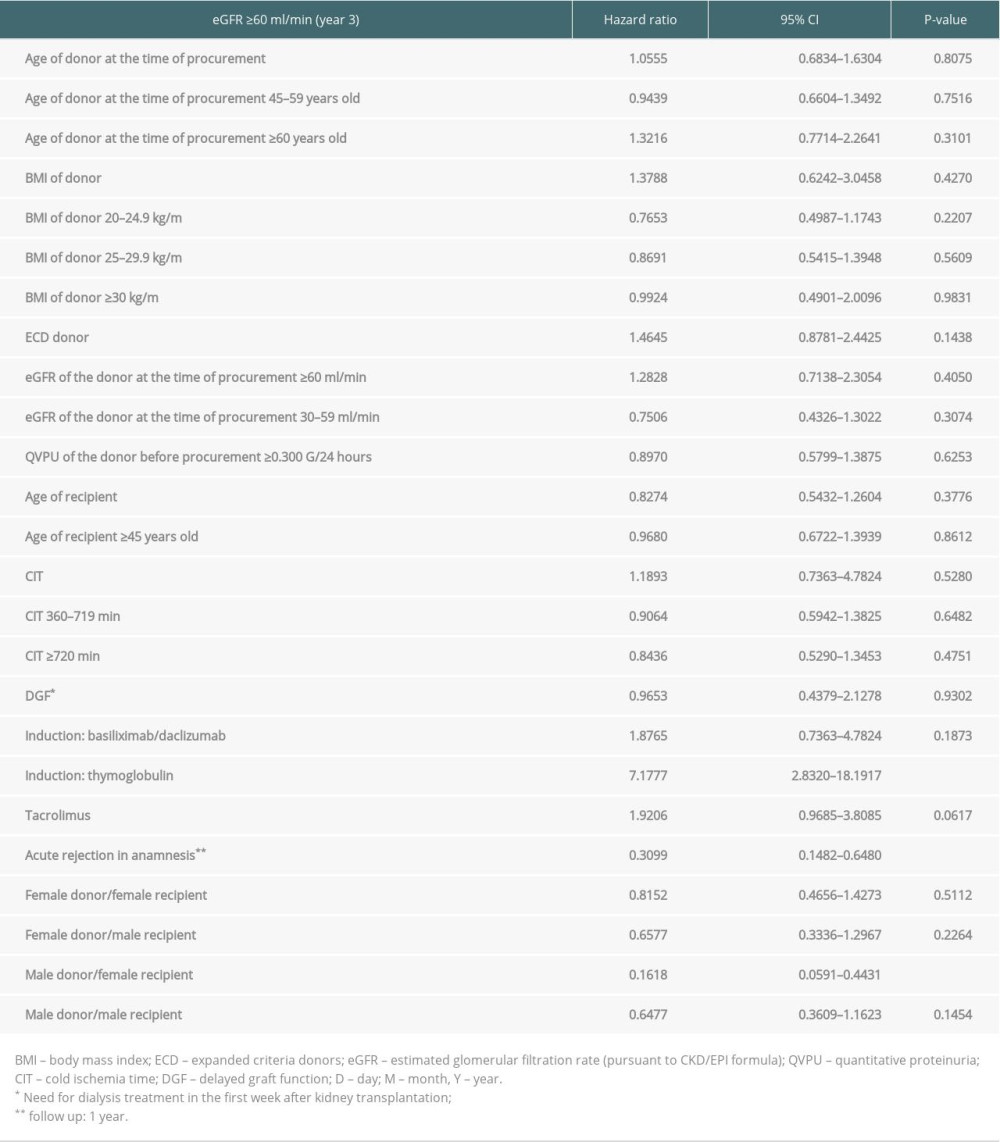 Table 6. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 5th year after KT).
Table 6. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 5th year after KT).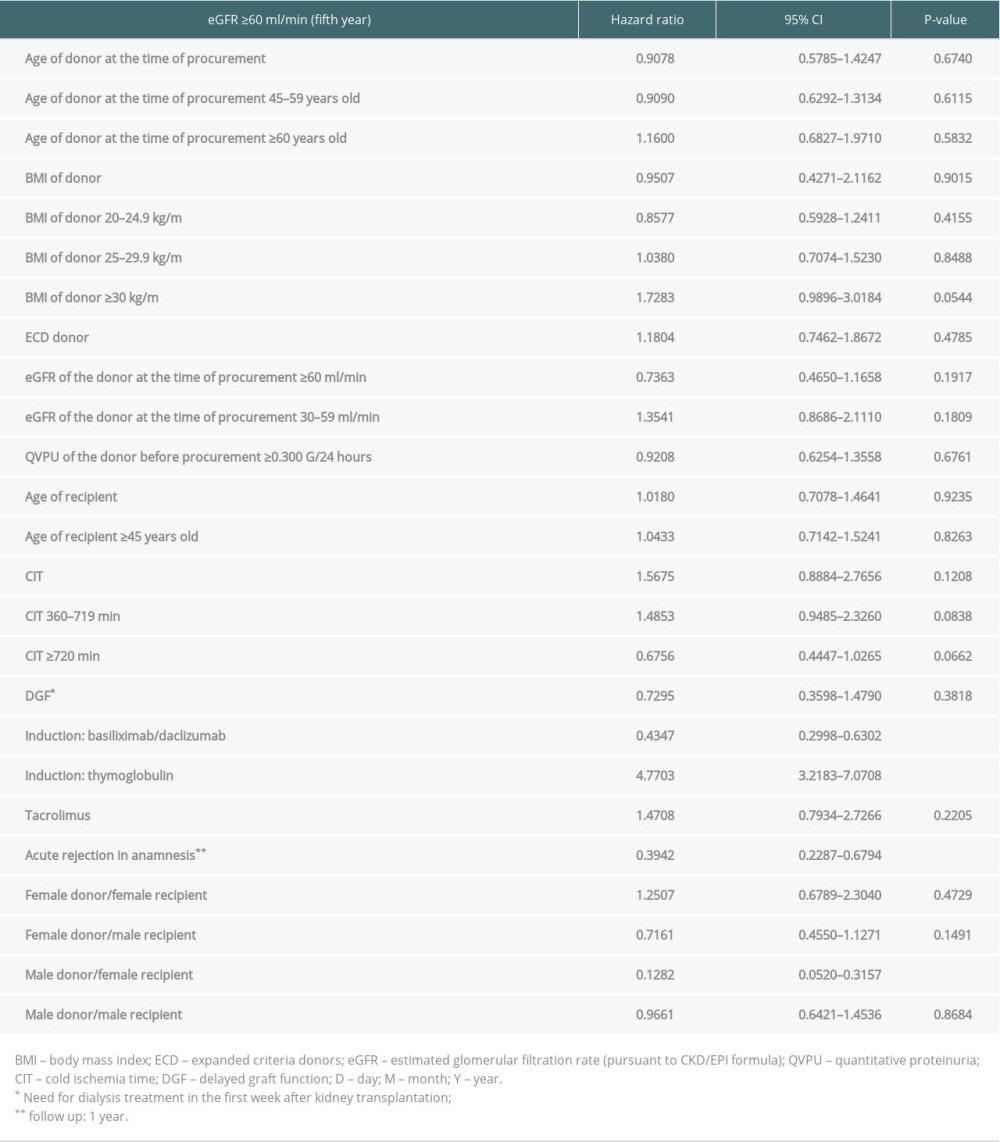 Table 7. Cox proportional hazards model (acute rejection in 1st year after KT).
Table 7. Cox proportional hazards model (acute rejection in 1st year after KT).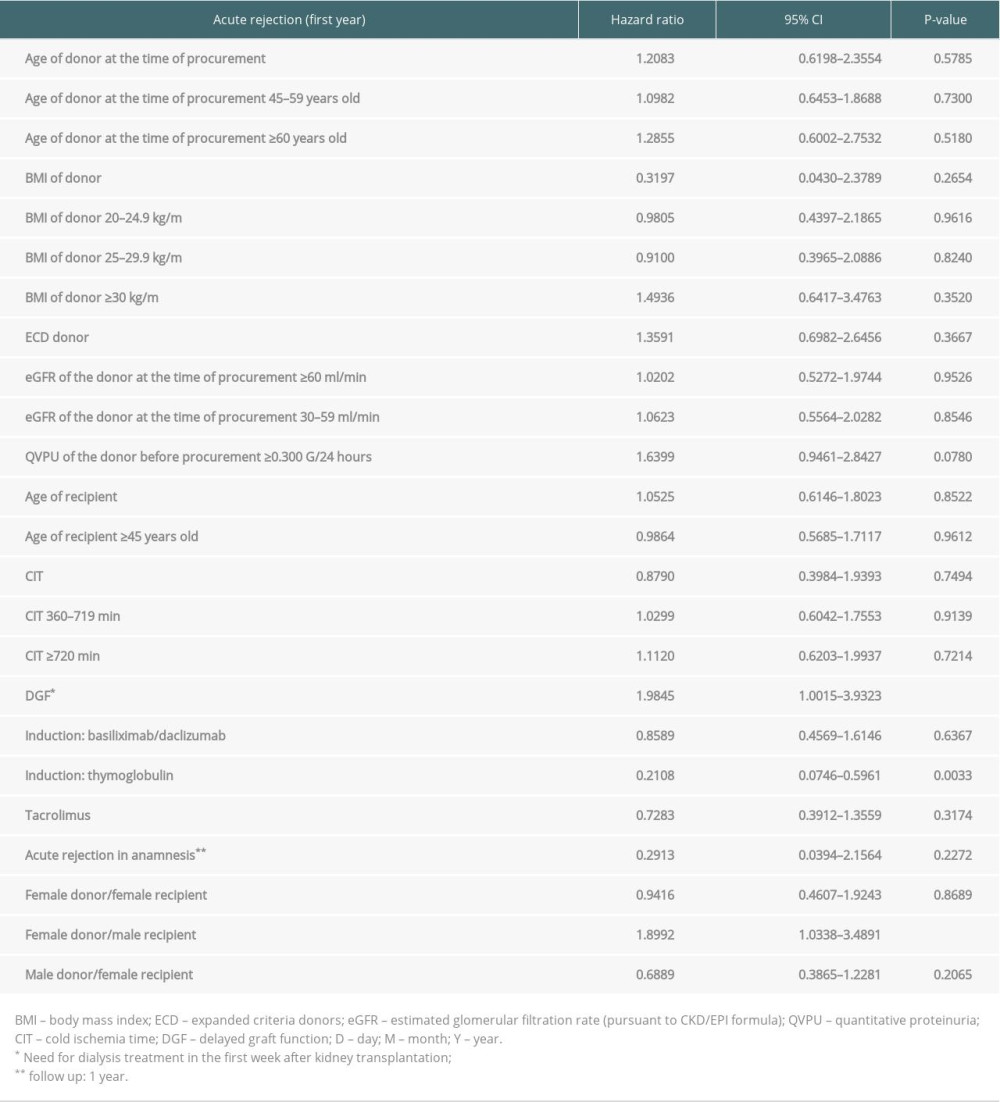
References
1. Cobo G, Hecking M, Port FK, Sex and gender differences in chronic kidney disease: progression to end-stage renal disease and haemodialysis: Clin Sci, 2016; 130; 1147-63
2. Hart A, Smith JM, Skeans MA, OPTN/SRTR 2017 annual data report: Kidney: Am J Transplant, 2019; 19-123
3. Krammer A, Pippias M, Noordzij M, The European Renal Association – European Dialysis and Transplant Association (ERA-EDTA) registry annual report 2015: A aummary: Clin Kidney J, 2018; 11(1); 108-22
4. Miller AJ, Kiberd BA, Alwayn IP, Donor-recipient weight and sex mismatch and the risk of graft loss in renal transplantation: J Am Soc Nephrol, 2017; 12(4); 669-76
5. Oh CK, Lee BM, Jeon KO, Gender-Related differences of renal mass supply and metabolic demand after living donor kidney transplantation: Clin Transplant, 2006; 20(2); 163-70
6. Klein SL, Marriott I, Fish EN, Sex-based differences in immune function and responses to vaccination: Trans R Soc Trop Med Hyg, 2015; 109(1); 9-15
7. Nadkarni S, McArthur S, Oestrogen and immunomodulation: New mechanisms that impact on peripheral and central immunity: Curr Opin Pharmacol, 2013; 13; 576-81
8. Gratwohl A, Döhler B, Stern M, Opelz G, H-Y as a minor histocompatibility antigen in kidney transplantation: A retrospective cohort study: Lancet, 2008; 372(9632); 49-53
9. Tan JC, Wadia PP, Coram M, H-Y antibody development associates with acute rejection in female patients with male kidney transplants: Transplantation, 2008; 86(1); 75-81
10. Dedinská I, Graňák K, Vnučák M, Role of sex in post-transplant diabetes mellitus development: Are men and women equal?: J Diabetes Complications, 2019; 33(4); 315-22
11. Lepeytre F, Dahhou M, Zhang X, Association of sex with risk of kidney graft failure differs by age: J Am Soc Nephrol, 2017; 28(10); 3014-23
12. Scheel J, Reber S, Stoessel L, Patient-reported non-adherence and immunosuppressant trough levels are associated with rejection after renal transplantation: BMC Nephrol, 2017; 18; 107
13. Denhaerynck K, Steiger J, Bock A, Prevalence and risk factors of non-adherence with immunosuppressive medication in kidney transplant patients: Am J Transplant, 2007; 7(1); 108-16
14. Scheel JF, Schieber K, Reber S, Psychosocial variables associated with immunosuppressive medication non-adherence after renal transplantation: Front Psychiatry, 2018; 9; 23
15. Levey AS, Eckardt KU, Tsukamoto Y, Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO): Kidney Int, 2005; 67(6); 2089-100
16. McGee J, Magnus JH, Islam TM, Donor-recipient gender and size mismatch affects graft success after kidney transplantation: J Am Coll Surg, 2010; 210(5); 718-25
17. Giral M, Foucher Y, Karam G, Kidney and recipient weight incompatibility reduces long-term graft survival: J Am Soc Nephrol, 2010; 21(6); 1022-29
18. el-Agroudy AE, Hassan NA, Bakr MA, Effect of donor/recipient body weight mismatch on patient and graft outcome in living-donor kidney transplantation: Am J Transplant, 2003; 23(5); 294-99
19. Foo YZ, Nakagawa S, Rhodes G, Simmons LW, The effects of sex hormones on immune function: A meta-analysis: Biol Rev Camb Philos Soc, 2017; 92(1); 551-71
20. Giefing-Kröll C, Berger P, Lepperdinger G, Grubeck-Loebenstein B, How sex and age affects immune responses, susceptibility to infections, and response to vaccination: Aging Cell, 2015; 14(3); 309-21
21. Tan JC, Busque S, Workeneh B, Effects of aging on glomerular function and number in living kidney donors: Kidney Int, 2010; 78(7); 686-92
22. Fulladosa X, Moreso F, Narvaez JA, Estimation of total glomerular number in stable renal transplants: J Am Soc Nephrol, 2003; 14(10); 2662-68
23. Ferrari P, Lim W, Dent H, McDonald SP, Effect of donor-recipient age difference on graft function and survival in live-donor kidney transplantation: Nephrol Dial Transplant, 2011; 26(22); 702-8
24. Tan JC, Workeneh B, Busque S, Glomerular function, structure, and number in renal allografts from older deceased donors: J Am Soc Nephrol, 2009; 20(1); 181-88
Figures
Figure 1. Development of the value of creatinine (A) and the eGFR (B) over time (donor – woman).Figure 2. Development of the value of creatinine (A) and the eGFR (B) over time (donor – man).Figure 3. The eGFR in year 1 (A), year 3 (B) and year 5 (C) after kidney transplantation (donor >50 years old, recipient ≤45 years old).Figure 4. The eGFR in year5 after kidney transplantation (donor ≤50 years old, recipient >45 years old).Figure 5. The eGFR in year 3 (A) and year5 (B) after kidney transplantation (donor ≤50 years old, recipient ≤45 years old).Figure 6. The eGFR in year 1, year 3, and year 5 after kidney transplantation (displays the percentage of patients with an eGFR >60 ml/min).Figure 7. The 1-year, 3-year, and 5-year graft survival after kidney transplantation.Figure 8. The 1-year, 3-year, and 5-year patient survival after kidney transplantation. Tables
Table 1. Group characteristics.Table 2. Group characteristics – female donor.Table 3. Group characteristics – male donor.Table 4. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 1st year after KT).Table 5. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 3rd year after KT).Table 6. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 5th year after KT).Table 7. Cox proportional hazards model (acute rejection in 1st year after KT).Table 1. Group characteristics.Table 2. Group characteristics – female donor.Table 3. Group characteristics – male donor.Table 4. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 1st year after KT).Table 5. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 3rd year after KT).Table 6. Cox proportional hazards model (end-point eGFR ≥60 ml/min in the 5th year after KT).Table 7. Cox proportional hazards model (acute rejection in 1st year after KT). In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988