02 July 2024: Original Paper
Clonal Hematopoiesis-Associated Gene Mutations Affect Acute Graft-Versus-Host Disease After Hematopoietic Stem Cell Transplantation in AML Patients
Xiaoxuan Wei12ABCDEF, Sai Huang1ABF, Zhenyang Gu1ADEF, Jing Liu1ADEF, Meng Li1AF, Xiangshu Jin1AF, Jian Bo1AF, Fei Li1A, Yu Jing1A, Xiaoning Gao1A, Liping Dou1AB, Daihong Liu1A, Chunji Gao1ADEF*DOI: 10.12659/AOT.943688
Ann Transplant 2024; 29:e943688






Abstract
BACKGROUND: The relationship between clonal hematopoiesis (CH)-associated gene mutations and allogeneic hematopoietic stem cell transplantation (allo-HSCT) has been extensively studied since next-generation sequencing (NGS) technology became widely available. However, research has mainly focused on the relationship between donor CH mutations and transplant prognosis, and research into the relationship between CH mutations in the recipient and acute graft-versus-host disease (aGVHD) is lacking.
MATERIAL AND METHODS: We analyzed NGS results and their correlation with aGVHD and prognosis in 196 AML patients undergoing allo-HSCT.
RESULTS: A total of 93 (47.4%) patients had CH mutations. The most frequently mutated genes were DNMT3A (28 of 196; 14.3%), TET2 (22 of 196; 11.2%), IDH1 (15 of 196; 7.7%), IDH2 (14 of 196; 7.1%), and ASXL1 (13 of 196; 6.6%). The incidence of aGVHD was higher in patients older than 45 years old with DTA mutations (DNMT3A, TET2 or ASXL1). DNMT3A mutation but not with TET2 or ASXL1 mutation was an independent risk factor for aGVHD in patients receiving allo-HSCT older than 45 years old. With a median follow-up of 42.7 months, CH mutations were not associated with overall survival and leukemia-free survival.
CONCLUSIONS: DNMT3A mutation, but not TET2 or ASXL1 mutation, was associated with higher incidence of aGVHD.
Keywords: Clonal Hematopoiesis, Graft vs Host Disease, Hematopoietic Stem Cell Transplantation, Leukemia, Myeloid, Acute, Humans, Male, Female, Middle Aged, adult, Mutation, young adult, Adolescent, DNA Methyltransferase 3A, Dioxygenases, DNA (Cytosine-5-)-Methyltransferases, Aged, Prognosis, Transplantation, Homologous, High-Throughput Nucleotide Sequencing, DNA-Binding Proteins, Repressor Proteins
Introduction
Clonal hematopoiesis (CH) is defined as the clonal expansion of single hematopoietic stem cells (HSCs) with driving somatic mutations or chromosomal abnormalities that give them a competitive advantage under positive selection pressure, resulting in clonal dominance [1]. Due to advancement of next-generation sequencing (NGS) technology in the past decade, more and more research groups found that CH is a common condition with aging and mutations in specific genes (eg,
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) remains the only curative therapy for AML. Unfortunately, successful outcomes of allo-HSCT are limited by graft-versus-host disease (GVHD) and malignant relapse. Transplantation and GVHD have been suggested to accelerate the aging of transplanted donor-derived HSPC, which in turn could foster the emergence of CH [6]. Studies on CH and HSCT have mainly focused on the correlation between donor CH mutations and disease prognosis, with inconsistent results [7–12]. Further research on the relationship between CH and GVHD will help to determine the disease prognosis.
Another noteworthy issue is that allo-HSCT cannot clear all the mutations in recipients [7]. Kim found that chemotherapy and HSCT significantly reduced allelic burden, but 41 mutations (28.9%) were detected at post-HCT day 21, with
We analyzed NGS results and their association of aGVHD and prognosis in 196 AML patients undergoing allo-HSCT. This work focused on the relationship between recipient CH mutations and aGVHD, providing early warning biomarkers for aGVHD and discussing their possible therapeutic targets.
Material and Methods
PATIENTS:
We included 196 AML patients who received allo-HSCT at Chinese People’s Liberation Army General Hospital between January 2010 and May 2021. Before treatment, NGS test was performed on all patients’ peripheral blood or bone marrow samples. This study is based on the 2016 World Health Organization (WHO) standards for diagnosis and classification of AML. NCCN risk stratification is based on 2021 NCCN guidelines. Complex karyotype was defined as ≥3 unrelated chromosome abnormalities in the absence of other class-defining recurring genetic abnormalities, excluding hyperdiploid karyotypes with 3 or more trisomies (or polysomies), without structural abnormalities [15]. Cytomegalovirus (CMV) infection, Epstein-Barr virus (EBV) infection, and fungal infection were defined as infection before aGVHD or in the 100 days after transplantation in patients without aGVHD.
All patients received cyclosporine (CsA), short-term methotrexate (MTX), and mycophenolate mofetil (MMF) as prophylaxis against graft-versus-host disease (GVHD). CsA was administered intravenously at a dose of 3 mg/kg from day 10 and transitioned to oral administration at around day 20–30. CsA was discontinued in patients who did not show signs of aGVHD. MTX was administered intravenously at a dose of 15 mg/m2 on day 1 and 10 mg/m2 on days 3, 6, and 11. MMF was given orally at a dose of 250 mg every 12 h from day 10 until engraftment.
GENETIC STUDIES:
Analysis of mutations present in the genes
STATISTICAL ANALYSIS:
SPSS 26.0 software was used for statistical analysis. The primary endpoints were overall survival (OS) and leukemia-free survival (LFS). OS was defined as the time from diagnosis to death from any cause or the last follow-up (July 28, 2021). LFS was defined as the time from the first complete remission to recurrence or death or the last follow-up. OS and LFS were estimated using Kaplan-Meier analysis, and the difference was tested with log-rank tests. Univariate and multivariate analyses were performed on Cox models for LFS and OS. Continuous variables (age, white blood cell count, hemoglobin level, platelet count, proportion of bone marrow blasts) are expressed as median (range), which were compared by the Mann-Whitney U test. Chi-square tests and Fisher’s exact tests were used to compare the classification variables (sex, donor type, FAB classification, NCCN risk stratification, GVHD). Logistic regression was used to explore the risk factors of aGVHD. Factors with
Results
MUTATION LANDSCAPE OF CH MUTATIONS IN AML PATIENTS RECEIVED ALLO-HSCT:
CH mutations were detected in 93 of 196 (47.4%) patients who had NGS performed before treatment. The most frequently mutated genes were DNMT3A (28 of 196; 14.3%), TET2 (22 of 196; 11.2%), IDH1 (15 of 196; 7.7%), IDH2 (14 of 196; 7.1%), and ASXL1 (13 of 196; 6.6%; Figure 1A). Of the 93 patients with CH mutations, 58 (62.4%) had 1, 27 (29.0%) had 2, and 8 (8.6%) patients had 3 different CH mutations (Figure 1B).
CLINICAL AND GENETIC CHARACTERISTICS OF CH MUTATIONS:
CH prevalence increased with advancing age: median age 36 years vs 42 years for patients without and with CH mutations (P =0.003, Table 1). Patients with mutated DNMT3A and TET2 were older than those without CH mutations (Figure 1C). The presence of CH mutations was also associated with higher platelet levels (P=0.048). Aside from the above differences, there were no significant differences in sex, complex karyotypes, NCCN risk stratification, and disease status at transplantation (Table 1).
ASSOCIATIONS OF CH MUTATIONS AND AGVHD:
AGVHD occurred in 116 (59.2%) patients – 40 patients with grade I aGVHD, 53 patients with grade II aGVHD, 17 patients with grade III aGVHD, and 6 patients with grade IV aGVHD – and data were missing for 1 patient (Table 2).
Considering the association of CH with older age, we investigated the incidence of aGVHD in patients in various age groups. In haploidentical hematopoietic stem cell transplantation (haplo-HSCT), patients with CH mutations had a higher incidence of aGVHD (79.4% vs 63.3%, P=0.049, Table 3). Then we analyzed which kind of mutations would contribute to this phenomenon, but there were no statistically significant results (not shown). However, when we classified the mutations by their mechanisms, statistically significant correlations were found between DTA (mutated DNMT3A, TET2 or ASXL1) and aGVHD (80.0% vs 40.9%, P=0.010, Table 3) in patients over 45 years old who underwent haplo-HSCT. To further investigate which mutation of the 3 played the most important part, we analyzed the data of patients with DNMT3A mutation but no TET2 or ASXL1 mutations and patients without DTA mutation, and found that patients with DNMT3A mutation but not the other t2 mutations had a higher probability of aGVHD (81.8% vs 40.9%, P=0.026, Table 3).
The incidences of grade II–IV and grade III–IV aGVHD were 69.0% vs 45.0% (P=0.048) and 20.7% vs 17.5% (P=0.738) for patients over 45 years old undergoing allo-HSCT with and without CH mutations, respectively (Table 4). A similar conclusion was also drawn for patients over 45 years old undergoing allo-HSCT (Tables 3, 4).
In the logistic regression analysis in patients over 45 years old and receiving haplo-HSCT, DNMT3A (with DNMT3A mutation but no TET2 or ASXL1 mutations vs without DTA mutations: P=0.045, OR=25.443, 95% CI: 1.072–603.681, Table 5) was corelated with the higher risk of aGVHD. The same conclusion was also drawn in patients over 45 years old undergoing allo-HSCT (with DNMT3A mutation but no TET2 or ASXL1 mutations vs without DTA mutations: P=0.033, OR=5.274, 95% CI: 1.140–24.393, Table 6).
ANALYSIS OF FACTORS RELATED TO AGVHD:
In the logistic regression analysis in patients receiving allo-HSCT, including NCCN risk stratification, donor type and different pathogens infection as covariates, donor type (matched vs haploidentical: p<0.001, OR=3.760, 95% CI: 2.005–7.049, Table 6) was associated with higher risk of aGVHD. Meanwhile, in the logistic regression analysis in patients with haplo-HSCT, including age, bone marrow blasts, DTA mutations, mutation of methylation, and different pathogens infection as covariates, age (P=0.026, OR=0.952, 95% CI: 0.912–0.994, Table 5) was associated with aGVHD. In patients younger than 45 years old and receiving haplo-HSCT, CMV infection (vs no CMV infection: P=0.032, OR=0.288, 95% CI: 0.092–0.900, Table 5) was corelated with the lower risk of aGVHD.
IMPACT OF CH MUTATIONS ON THE PROGNOSIS OF AML PATIENTS:
The median follow-up was 42.7 months (4.6–145.8 months) in this study. The 5-year OS rate was 65.3%. Kaplan-Meier survival analysis did not show survival differences according to CH mutations regardless of the type of transplantation (Figure 2). The complication of transplantation-associated thrombotic microangiopathy (TA-TMA) was associated with a significantly shorter OS and LFS (Figures 3, 4) and a poor pretransplant disease status was associated with a significantly shorter LFS in patients undergoing allo-HSCT (Figure 4).
Univariate analysis of OS and LFS in patients undergoing allo-HSCT showed that CH mutations, DTA mutations, and mutated DNMT3A were not risk factors for poor prognosis of OS and LFS (Table 7). The risk factors include pretransplant disease status (OS: NR vs CR, P=0.006, HR=3.646, 95% CI: 1.457–9.121; LFS: NR vs CR, p=0.013, HR=3.570, 95% CI: 1.301–9.793, Rel vs CR, P=0.039, HR=2.182, 95% CI: 1.005–4.739; Table 7) and complication of TA-TMA (yes vs no, OS: P=0.010, HR=3.050, 95% CI: 1.313–7.083; LFS: P=0.009, HR=2.803, 95% CI: 1.287–6.101; Table 7). In allo-HSCT patients, multivariate analysis showed that patients with pretransplant NR tended to have worse OS than those with pretransplant CR (p=0.009, HR=3.444, 95% CI: 1.366–8.685; Table 7), and patients with pretransplant recurrence tended to have poorer LFS (Rel vs CR, p=0.023, HR=2.490, 95% CI: 1.134–5.467; Table 7). The risk factors of OS and LFS also include concurrent TA-TMA (yes vs no, OS: P=0.012, HR=3.000, 95% CI: 1.277–7.049; LFS: P=0.013, HR=2.703, 95% CI: 1.230–5.940; Table 7).
Discussion
GVHD results from immune cells transplanted from a non-identical donor recognizing the recipient as foreign, thereby initiating an immune response that causes disease. There has been fierce debate between CH and GVHD in previous studies. Frick found a high cumulative incidence of chronic GVHD (cGVHD) but not aGVHD in recipients allografted with donor CH [11]. Frick’s view was supported by Gibson, who concluded that
In our study,
The association between CH and aging is receiving increasing attention [5,18,19]. As expected, patients with
Furthermore, according to relevant studies on the pathogenesis of aGVHD and the function of
In our study, CH mutations were not associated with OS and LFS. There are different views on the impact of CH mutations on prognosis. In Heuser’s study, DTA mutations had no prognostic significance in cumulative incidence of relapses, relapse-free survival, or overall outcome, excluding donor origin [10]. Grimm concluded that the presence of CH did not negatively impact the outcome of an allo-HSCT [8]. Frick and Newell confirmed that donor CH had no effect on prognosis [11,13]. Conversely, Gibson showed that CH was associated with an adverse prognosis after autologous stem cell transplantation for lymphoma [14]. Upon successful allo-HSCT, the recipient’s hematopoiesis is replaced by the donor’s, thereby eliminating CH mutations. It has therefore been speculated that CH mutations are reliable markers of MRD after allo-HSCT, as they indicate the persistence or relapse of recipient hematopoiesis and the leukemic clone [31]. Unfortunately, there is insufficient evidence to prove that CH mutations can be used as MRD tests [15]. Based on our study, CH mutations are not associated with OS and LFS, which may be due to the following 2 factors. Inflammation as well as increased proliferation of HSPCs, which may promote expansion of clones with a proliferative advantage, are inevitable consequences of HSCT, resulting in poor prognosis [32], but chemotherapy and HSCT can eliminate CH clones and their negative effects [12]. Secondly, the enhanced GVL of the immune response mitigates the adverse outcome of the high inflammatory response [11].
This study has potential limitation. In our research, it was difficult to distinguish CH from AML clones. We could only report this phenomenon, and further exploration of the mechanism and efforts to distinguish CH and AML clones are still needed. When specific mutation is involved, such as only
Conclusions
Figures
 Figure 1. The landscape of CH mutations in 196 AML patients. (A) The most frequently mutated genes were DNMT3A, TET2, IDH1, IDH2 and ASXL1. (B) Co-mutation distribution in 93 patients with CH mutations. (C) The distribution of age on the basis of CH status and mutations in individual genes or groups of genes. Figure was created using GraphPad Prism 10 by Dotmatics.
Figure 1. The landscape of CH mutations in 196 AML patients. (A) The most frequently mutated genes were DNMT3A, TET2, IDH1, IDH2 and ASXL1. (B) Co-mutation distribution in 93 patients with CH mutations. (C) The distribution of age on the basis of CH status and mutations in individual genes or groups of genes. Figure was created using GraphPad Prism 10 by Dotmatics.  Figure 2. Kaplan-Meier curves depict the overall survival and leukemia-free survival. (A) For patients undergoing HSCT, CH mutation was not associated with OS. (B) The same conclusion was drawn for patients who had haplo-HSCT. (C, D) The same conclusion was drawn for LFS. CH mutations – clonal hematopoiesis-associated mutation; HSCT – hematopoietic stem cell transplantation; OS – overall survival; haplo-HSCT – haploidentical hematopoietic stem cell transplantation; LFS – leukemia-free survival. Figure was created using GraphPad Prism 10 by Dotmatics.
Figure 2. Kaplan-Meier curves depict the overall survival and leukemia-free survival. (A) For patients undergoing HSCT, CH mutation was not associated with OS. (B) The same conclusion was drawn for patients who had haplo-HSCT. (C, D) The same conclusion was drawn for LFS. CH mutations – clonal hematopoiesis-associated mutation; HSCT – hematopoietic stem cell transplantation; OS – overall survival; haplo-HSCT – haploidentical hematopoietic stem cell transplantation; LFS – leukemia-free survival. Figure was created using GraphPad Prism 10 by Dotmatics.  Figure 3. Kaplan-Meier curves depict the overall survival. (A) For patients undergoing HSCT, TA-TMA was associated with a significantly shorter OS. (B) The same conclusion was drawn for patients who had haplo-HSCT. HSCT – hematopoietic stem cell transplantation; TA-TMA – transplantation-associated thrombotic microangiopathy; OS – overall survival; haplo-HSCT – haploidentical hematopoietic stem cell transplantation. Figure was created using GraphPad Prism 10 by Dotmatics.
Figure 3. Kaplan-Meier curves depict the overall survival. (A) For patients undergoing HSCT, TA-TMA was associated with a significantly shorter OS. (B) The same conclusion was drawn for patients who had haplo-HSCT. HSCT – hematopoietic stem cell transplantation; TA-TMA – transplantation-associated thrombotic microangiopathy; OS – overall survival; haplo-HSCT – haploidentical hematopoietic stem cell transplantation. Figure was created using GraphPad Prism 10 by Dotmatics.  Figure 4. Kaplan-Meier curves depict the leukemia-free survival. (A, B) For patients undergoing HSCT, TA-TMA, and a poor pretransplant status were associated with a significantly shorter LFS. (C, D) Only TA-TMA was connected to a shorter LFS in patients had haplo-HSCT. HSCT – hematopoietic stem cell transplantation; TA-TMA – transplantation-associated thrombotic microangiopathy; LFS – leukemia-free survival; haplo-HSCT – haploidentical hematopoietic stem cell transplantation; CR – complete remission; PR – partial response; NR – no response. Figure was created using GraphPad Prism 10 by Dotmatics.
Figure 4. Kaplan-Meier curves depict the leukemia-free survival. (A, B) For patients undergoing HSCT, TA-TMA, and a poor pretransplant status were associated with a significantly shorter LFS. (C, D) Only TA-TMA was connected to a shorter LFS in patients had haplo-HSCT. HSCT – hematopoietic stem cell transplantation; TA-TMA – transplantation-associated thrombotic microangiopathy; LFS – leukemia-free survival; haplo-HSCT – haploidentical hematopoietic stem cell transplantation; CR – complete remission; PR – partial response; NR – no response. Figure was created using GraphPad Prism 10 by Dotmatics. Tables
Table 1. Characteristics of patients.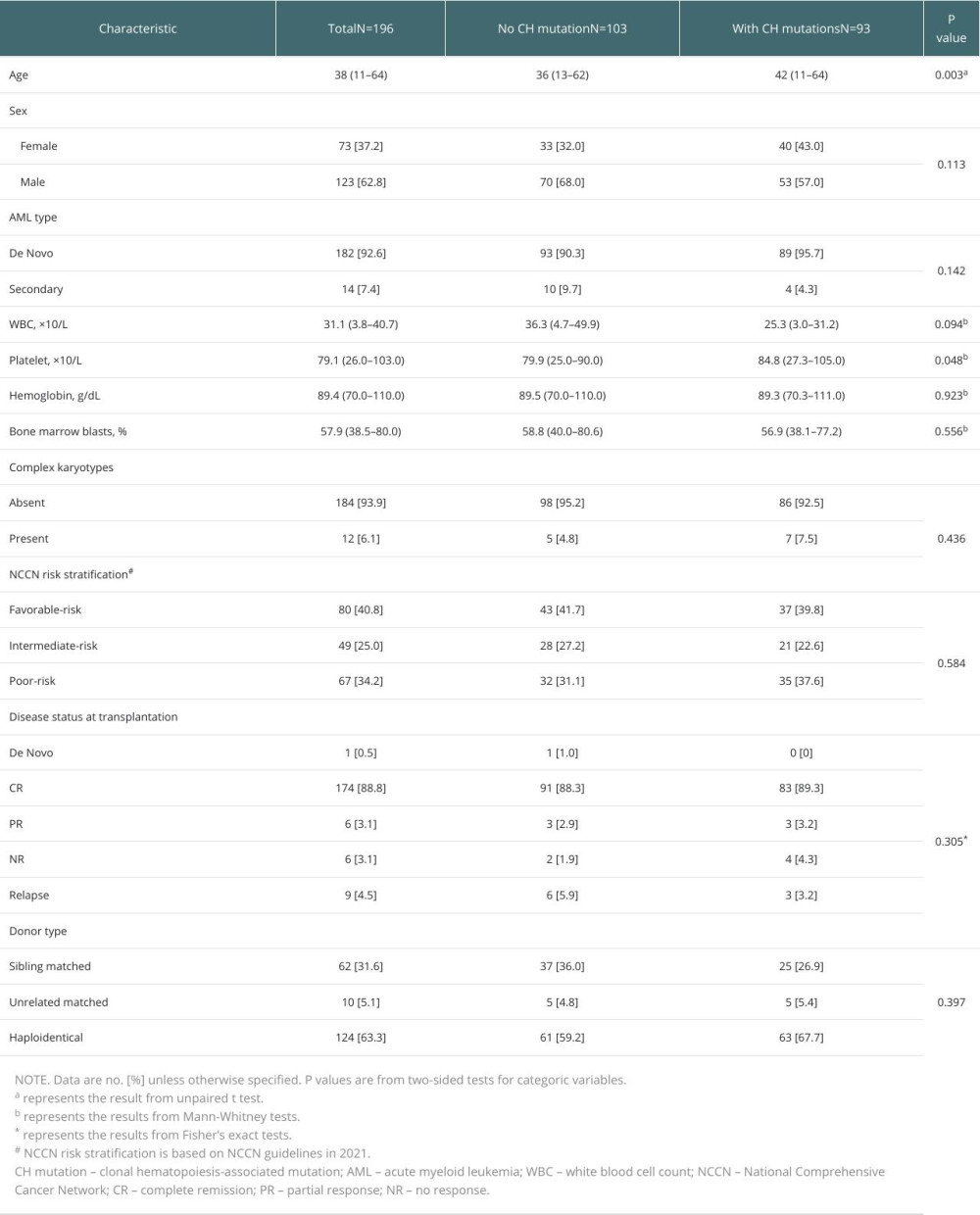 Table 2. Incidence of aGVHD.
Table 2. Incidence of aGVHD. Table 3. DNMT3A but not TET2 or ASXL1 mutation was associated with increased risk of aGVHD in patients over 45 years old.
Table 3. DNMT3A but not TET2 or ASXL1 mutation was associated with increased risk of aGVHD in patients over 45 years old. Table 4. The risk of aGVHD.
Table 4. The risk of aGVHD. Table 5. Univariate and Multivariate analysis of the association of various clinical features with aGVHD in patients receiving haplo-HSCT.
Table 5. Univariate and Multivariate analysis of the association of various clinical features with aGVHD in patients receiving haplo-HSCT. Table 6. Univariate and Multivariate analysis of the association of various clinical features with aGVHD in patients receiving allo-HSCT.
Table 6. Univariate and Multivariate analysis of the association of various clinical features with aGVHD in patients receiving allo-HSCT. Table 7. Univariate and multivariate analyses for OS and PFS in 196 patients receiving allo-HSCT.
Table 7. Univariate and multivariate analyses for OS and PFS in 196 patients receiving allo-HSCT.
References
1. Ye B, Sheng Y, Zhang M, Early detection and intervention of clonal hematopoiesis for preventing hematological malignancies: Cancer Letters, 2022; 538; 215691
2. Genovese G, Kähler AK, Handsaker RE, Clonal hematopoiesis and blood-cancer risk inferred from blood DNA sequence: N Engl J Med, 2014; 371; 2477-87
3. Tsai FD, Lindsley RC, Clonal hematopoiesis in the inherited bone marrow failure syndromes: Blood, 2020; 136; 1615-22
4. Kjær L, Clonal hematopoiesis and mutations of myeloproliferative neoplasms: Cancers (Basel), 2020; 12(8); 2100
5. Cupit-Link MC, Arora M, Wood WA, Relationship between aging and hematopoietic cell transplantation: Biol Blood Marrow Transplant, 2018; 24; 1965-70
6. von Bonin M, Jambor HK, Teipel R, Clonal hematopoiesis and its emerging effects on cellular therapies: Leukemia, 2021; 35; 2752-58
7. Gaidzik VI, Weber D, Paschka P, DNMT3A mutant transcript levels persist in remission and do not predict outcome in patients with acute myeloid leukemia: Leukemia, 2018; 32; 30-37
8. Grimm J, Bill M, Jentzsch M, Clinical impact of clonal hematopoiesis in acute myeloid leukemia patients receiving allogeneic transplantation: Bone Marrow Transplant, 2019; 54; 1189-97
9. Hasserjian RP, Steensma DP, Graubert TA, Clonal hematopoiesis and measurable residual disease assessment in acute myeloid leukemia: Blood, 2020; 135; 1729-38
10. Heuser M, Heida B, Büttner K, Posttransplantation MRD monitoring in patients with AML by next-generation sequencing using DTA and non-DTA mutations: Blood Advances, 2021; 5; 2294-304
11. Frick M, Chan W, Arends CM, Role of donor clonal hematopoiesis in allogeneic hematopoietic stem-cell transplantation: J Clin Oncol, 2019; 37; 375-85
12. Kim T, Moon JH, Ahn J-S, Next-generation sequencing-based posttransplant monitoring of acute myeloid leukemia identifies patients at high risk of relapse: Blood, 2018; 132; 1604-13
13. Newell LF, Williams T, Liu J, Engrafted donor-derived clonal hematopoiesis after allogenic hematopoietic cell transplantation is associated with chronic graft-versus-host disease requiring immunosuppressive therapy, but no adverse impact on overall survival or relapse: Transplant Cell Ther, 2021; 27; 662.e1-e9
14. Gibson CJ, Lindsley RC, Tchekmedyian V, Clonal hematopoiesis associated with adverse outcomes after autologous stem-cell transplantation for lymphoma: J Clin Oncol, 2017; 35; 1598-605
15. Döhner H, Wei AH, Appelbaum FR, Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN: Blood, 2022; 140; 1345-77
16. Gibson CJ, Kim HT, Zhao L, Donor clonal hematopoiesis and recipient outcomes after transplantation: J Clin Oncol, 2022; 40; 189-201
17. Oran B, Champlin RE, Wang F, Donor clonal hematopoiesis increases risk of acute graft versus host disease after matched sibling transplantation: Leukemia, 2022; 36; 257-62
18. Ahmad H, Jahn N, Jaiswal S, Clonal hematopoiesis and its impact on human health: Annu Rev Med, 2023; 74; 249-60
19. Miller PG, Steensma DP, Implications of clonal hematopoiesis for precision oncology: JCO Precis Oncol, 2020; 4; 639-46
20. Nassereddine S, Rafei H, Elbahesh E, Acute graft versus host disease: A comprehensive review: Anticancer Res, 2017; 37; 1547-55
21. Cook EK, Luo M, Rauh MJ, Clonal hematopoiesis and inflammation: Partners in leukemogenesis and comorbidity: Exp Hematol, 2020; 83; 85-94
22. Khrabrova DA, Yakubovskaya MG, Gromova ES, AML-associated mutations in DNA methyltransferase DNMT3A: Biochemistry (Mosc), 2021; 86; 307-18
23. Yu Q, Zhou B, Zhang Y, DNA methyltransferase 3a limits the expression of interleukin-13 in T helper 2 cells and allergic airway inflammation: Proc Natl Acad Sci USA, 2012; 109; 541-46
24. Gamper CJ, Agoston AT, Nelson WG, Identification of DNA methyltransferase 3a as a T cell receptor-induced regulator of Th1 and Th2 differentiation: J Immunol, 2009; 183; 2267-76
25. Ktena YP, Koldobskiy MA, Barbato MI, Donor T cell DNMT3a regulates alloreactivity in mouse models of hematopoietic stem cell transplantation: J Clin Invest, 2022; 132(13); e158047
26. Reddy V, Winer AG, Eksioglu E, Interleukin 12 is associated with reduced relapse without increased incidence of graft-versus-host disease after allogeneic hematopoietic stem cell transplantation: Biol Blood Marrow Transplant, 2005; 11; 1014-21
27. Darlak KA, Wang Y, Li J-M, Enrichment of IL-12-producing plasmacytoid dendritic cells in donor bone marrow grafts enhances graft-versus-leukemia activity in allogeneic hematopoietic stem cell transplantation: Biol Blood Marrow Transplant, 2013; 19; 1331-39
28. Božić T, Frobel J, Raic A, Variants of DNMT3A cause transcript-specific DNA methylation patterns and affect hematopoiesis: Life Sci Alliance, 2018; 1; e201800153
29. SanMiguel JM, Eudy E, Loberg MA, Distinct tumor necrosis factor alpha receptors dictate stem cell fitness versus lineage output in Dnmt3a-mutant clonal hematopoiesis: Cancer Discovery, 2022; 12; 2763-73
30. Husby S, Jørgensen GØ, Favero F, Level of unique T cell clonotypes is associated with clonal hematopoiesis and survival in patients with lymphoma undergoing ASCT: Bone Marrow Transplant, 2022; 57; 674-47
31. Schuurhuis GJ, Heuser M, Freeman S, Minimal/measurable residual disease in AML: A consensus document from the European LeukemiaNet MRD Working Party: Blood, 2018; 131; 1275-91
32. Wilk CM, Manz MG, Boettcher S, Clonal hematopoiesis in hematopoietic stem cell transplantation: Curr Opin Hematol, 2021; 28; 94-100
33. Brunetti L, Gundry MC, Goodell MA, DNMT3A in leukemia: Cold Spring Harb Perspect Med, 2017; 7; a030320
Figures
Figure 1. The landscape of CH mutations in 196 AML patients. (A) The most frequently mutated genes were DNMT3A, TET2, IDH1, IDH2 and ASXL1. (B) Co-mutation distribution in 93 patients with CH mutations. (C) The distribution of age on the basis of CH status and mutations in individual genes or groups of genes. Figure was created using GraphPad Prism 10 by Dotmatics.Figure 2. Kaplan-Meier curves depict the overall survival and leukemia-free survival. (A) For patients undergoing HSCT, CH mutation was not associated with OS. (B) The same conclusion was drawn for patients who had haplo-HSCT. (C, D) The same conclusion was drawn for LFS. CH mutations – clonal hematopoiesis-associated mutation; HSCT – hematopoietic stem cell transplantation; OS – overall survival; haplo-HSCT – haploidentical hematopoietic stem cell transplantation; LFS – leukemia-free survival. Figure was created using GraphPad Prism 10 by Dotmatics.Figure 3. Kaplan-Meier curves depict the overall survival. (A) For patients undergoing HSCT, TA-TMA was associated with a significantly shorter OS. (B) The same conclusion was drawn for patients who had haplo-HSCT. HSCT – hematopoietic stem cell transplantation; TA-TMA – transplantation-associated thrombotic microangiopathy; OS – overall survival; haplo-HSCT – haploidentical hematopoietic stem cell transplantation. Figure was created using GraphPad Prism 10 by Dotmatics.Figure 4. Kaplan-Meier curves depict the leukemia-free survival. (A, B) For patients undergoing HSCT, TA-TMA, and a poor pretransplant status were associated with a significantly shorter LFS. (C, D) Only TA-TMA was connected to a shorter LFS in patients had haplo-HSCT. HSCT – hematopoietic stem cell transplantation; TA-TMA – transplantation-associated thrombotic microangiopathy; LFS – leukemia-free survival; haplo-HSCT – haploidentical hematopoietic stem cell transplantation; CR – complete remission; PR – partial response; NR – no response. Figure was created using GraphPad Prism 10 by Dotmatics. Tables
Table 1. Characteristics of patients.Table 2. Incidence of aGVHD.Table 3. DNMT3A but not TET2 or ASXL1 mutation was associated with increased risk of aGVHD in patients over 45 years old.Table 4. The risk of aGVHD.Table 5. Univariate and Multivariate analysis of the association of various clinical features with aGVHD in patients receiving haplo-HSCT.Table 6. Univariate and Multivariate analysis of the association of various clinical features with aGVHD in patients receiving allo-HSCT.Table 7. Univariate and multivariate analyses for OS and PFS in 196 patients receiving allo-HSCT.Table 1. Characteristics of patients.Table 2. Incidence of aGVHD.Table 3. DNMT3A but not TET2 or ASXL1 mutation was associated with increased risk of aGVHD in patients over 45 years old.Table 4. The risk of aGVHD.Table 5. Univariate and Multivariate analysis of the association of various clinical features with aGVHD in patients receiving haplo-HSCT.Table 6. Univariate and Multivariate analysis of the association of various clinical features with aGVHD in patients receiving allo-HSCT.Table 7. Univariate and multivariate analyses for OS and PFS in 196 patients receiving allo-HSCT. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988