05 November 2024: Original Paper
The Long-Acting Glucagon-Like Peptide-2 Analog Apraglutide Enhances Intestinal Protection and Survival After Chemotherapy and Allogeneic Transplantation in Mice
Mark D. Minden1ABCDE, Cindy Audiger23BCDE, Geneviève Chabot-Roy2BCDE, Sylvie LesageDOI: 10.12659/AOT.945249
Ann Transplant 2024; 29:e945249






Abstract
BACKGROUND: The gastrointestinal (GI) barrier can be damaged by chemotherapy or radiation therapy, causing fatigue, malnutrition, sepsis, dose-limiting toxicity, and, occasionally, death. Glucagon-like peptide-2 (GLP-2) promotes mucosal epithelium growth and repair in the GI tract. Here, we examined the GI-protective effects of apraglutide, a long-acting peptide GLP-2 analog, in murine models of chemotherapy, and total body irradiation followed by allogeneic transplantation.
MATERIAL AND METHODS: The impact of apraglutide on cytarabine or melphalan chemotherapy-induced intestinal damage was assessed in BALB/c mice, and the effect on allogeneic transplantation in BALB/cJ and C57BL/6J mice. Outcomes included survival, and changes in body weight, intestinal function and morphology, including colon length and bacterial composition of the intestinal microbiota.
RESULTS: Adding apraglutide to chemotherapy significantly improved survival rates and reduced weight loss, with no impact on leukocyte counts (and, therefore, no effect on chemotherapy-induced immunosuppression), compared with chemotherapy alone in mice. These benefits were associated with preservation of the morphological integrity of the GI mucosa, attenuation of the negative impact of cytarabine on the intestinal microbiota, and significant improvement in plasma levels of citrulline. In addition, in a model of irradiation followed by allogeneic transplantation, mice in groups receiving apraglutide had improved survival, reduced weight loss, and increased colon length compared with those that did not.
CONCLUSIONS: Apraglutide protects intestinal function and improves survival in mice following allogeneic transplantation or chemotherapy with cytarabine or melphalan. The potential effect of apraglutide on chemotherapy efficacy and on engraftment following allogeneic transplantation has been investigated in a parallel manuscript.
Keywords: apraglutide, Cytarabine, glucagon-like peptide-2 (3-33), Immunosuppression Therapy, Animals, Mice, Glucagon-Like Peptide 2, Mice, Inbred BALB C, Mice, Inbred C57BL, Transplantation, Homologous, Melphalan, Male, Intestinal Mucosa, Gastrointestinal Microbiome, Intestines
Introduction
Acute graft-versus-host disease (aGvHD) is a frequent complication of allogeneic hematopoietic stem cell transplantation (allo-HSCT) that may be life-threatening [1–4]. Every year, approximately 26,000 patients receive allo-HSCT, a standard of care and a potentially curative treatment for many hematological cancers [5–8], across the US, Europe, and Japan [1,9]. The proportion of patients who develop aGvHD after allo-HSCT despite prophylaxis with immunosuppressive therapy [10] varies from 20% to 80% [11,12].
Gastrointestinal (GI) tract involvement in aGvHD is associated with significant morbidity and mortality [13]. The vital intestinal L-cells are directly impacted by tissue damage triggered by conditioning chemotherapy or aGvHD; these cells secrete glucagon-like peptide-2 (GLP-2), an essential endocrine hormone that maintains GI integrity and nutrient/fluid absorption and repairs and regenerates cells that sustain healthy intestinal epithelium [14].
Endogenous GLP-2 is a 33-amino acid peptide derived from post-translational processing of proglucagon in intestinal L-cells that is released into the circulation following nutrient ingestion [15–18]. GLP-2 acts locally to stimulate intestinal nutrient transport and intestinal blood flow, while enhancing gut barrier function. GLP-2 also promotes organ-specific stimulation of intestinal growth through increased proliferation and decreased apoptosis of mucosal epithelial cells [19–23]. A decline in endogenous GLP-2 secretion disrupts the repair and regeneration of intestinal stem cells, Paneth cells, and goblet cells [14,24].
This profound deletion of intestinal stem cells and Paneth cells associated with aGvHD leads to disrupted GI homeostasis and a higher incidence of steroid-refractory aGvHD in patients who have less than one L-cell per crypt [14,24]. Additionally, low Paneth cell count at the onset of aGvHD in the GI tract (GI aGvHD) is an important risk factor for increased non-relapse mortality [25,26].
Consequently, GLP-2-based therapy is of interest as a protective approach in pathologic conditions where the integrity of the intestinal mucosa or its absorptive function are compromised by disease or cytotoxic therapy, to protect from the secondary life-threatening consequences of these regimens [25,26].
High-dose chemotherapy, in particular, and radiotherapy, given alone or as part of bone marrow transplantation (BMT) conditioning, act on rapidly dividing cells of the gut and induce profound damage of the GI epithelium [27] This results in a breakdown of functional epithelial cells, which, in turn, contributes to symptoms such as vomiting, abdominal pain, and diarrhea [13,28]. Critically, loss of the GI-protective barrier permits the translocation of intestinal bacteria into the systemic circulation [27]. Coupled with drug- or radiotherapy-induced neutropenia, this frequently results in life-threatening sepsis and, occasionally, death [29]. In addition, the use of antibiotics as prophylaxis or therapy for sepsis results in the development of multidrug-resistant bacteria and changes in the microbiome, which consequently alters the functioning of the immune system [27,30].
Preclinical and clinical data have shown that GLP-2 analogs improve intestinal absorption and clinical signs of GI aGvHD [31,32]. Apraglutide (Ironwood Pharmaceuticals, Basel, Switzerland) is a synthetic GLP2 analog with a unique pharmacologic profile, rationally designed to be more potent, selective, and longer acting than human GLP-2 (hGLP-2) and other GLP-2 analogs, resulting in enhanced intestinotrophic effect [33]. Apraglutide also binds to rat, monkey and pig GLP-2 receptors with a potency similar to, or within approximately twice, that of native hGLP-2 and with 90% maximal efficacy [33]. The selectivity of apraglutide for the GLP-2 receptor has been further confirmed using a panel of 80 receptors, ion channels, and transporters. Apraglutide was specifically designed to be resistant to cleavage by dipeptidyl peptidase-4 (DPP4) and to have increased protein binding, which significantly prolonged the in vivo half-life of the peptide (72 hours in rats) vs native hGLP-2 (7 minutes) [33].
In this study, we investigated how pretreatment with apraglutide preserved intestinal function in murine models of chemotherapy (cytarabine or melphalan) and of irradiation followed by allogeneic transplantation. The GI-protective effect of apraglutide against chemotherapy-induced GI damage was assessed by multiple modalities, including citrulline measurements – a plasma biomarker of enterocyte mass that is reduced after intestinal mucosal damage [34–36] – in 2 different animal models for cytarabine and high-dose melphalan – 2 chemotherapeutic agents that are routinely used in the treatment of various hematological cancers (eg leukemia, multiple myeloma, and lymphomas) [37–39].
Material and Methods
ANIMALS AND HOUSING:
Studies were conducted at the Department of Medical Oncology and Hematology of the Princess Margaret Hospital (University Health Network, Toronto, Canada; impact of apraglutide on cytarabine-induced intestinal damage) and at ITR Laboratories (ITR Laboratories Canada Inc, Montreal, Québec, Canada; impact of apraglutide on melphalan-induced intestinal damage and effect on allogeneic transplantation). Study plans and in-life procedures were approved by the local Animal Care Committees and studies were conducted according to the Canadian Council on Animal Care’s Guide to the Care and Use of Experimental Animals and the US National Institutes of Health’s Guide for the Care and Use of Laboratory Animals [40,41]. Female and male BALB/cAnNCRL mice (Charles River Canada Inc, St-Constant, Québec, Canada, and The Jackson Laboratory, Maine, USA) were used in the studies of chemotherapy-induced gastrointestinal (GI) damage.
The study investigating the effect of apraglutide in a model of GI damage resulting from allogeneic transplantation after total body irradiation was conducted at the Maisonneuve-Rosemont Hospital (Montreal, Québec, Canada). BALB/cJ (n=20 for Experiment 1 [8.5 Gy] and n=25 for Experiment 2 [7.0 Gy]) and C57BL/6J male mice (n=10 for each experiment) aged 7–8 weeks (The Jackson Laboratory, Maine, USA) were maintained in a specific pathogen-free barrier facility. All experimental procedures were approved by the local ethics committee, overseen by the Canadian Council for Animal Protection.
HOUSING CONDITIONS:
Mice were held at no more than 4 mice per cage in ventilated cages with appropriate bedding material (Envigo [Harlan] Teklad Sani-Chips 7090) as well as food (Envigo [Harlan] Teklad 2018) and water ad libitum. Sterile water was purified and filtered at 0.2 μm, with pH adjusted to 2.5. Housing rooms had controlled environmental conditions of temperature (23.5±2°C) and humidity (60±12%), with a 12-hour light/dark cycle and with ad libitum access to standard certified commercial rodent chow and water, in HEPA-filtered air (8–12 air exchanges per hour with no recirculation). During the acclimation period, animals were assigned to their respective dose groups by block randomization based on body weights.
ANIMAL MONITORING:
Mortality checks were performed at least twice a day during all study phases. Mice were weighed daily from day +1 to day +14 during the treatment period, between 10am and 11am. Weight control protocols followed established guidelines for diet control in laboratory animals from the Canadian Council on Animal Care’s Guide to the Care and Use of Experimental Animals and the US National Institutes of Health’s Guide for the Care and Use of Laboratory Animals [40,41]. Following ethical guidelines, mice with weight loss ≥25% or reaching other limit points were sacrificed. Cage side clinical signs were monitored daily, except on days of detailed clinical examination. Specific attention was paid to diarrhea, signs of dehydration, and cachexia (wasting syndrome). Animals whose health status was judged to warrant additional evaluation were examined by a clinical veterinarian or by a technician working under the supervision of a clinical veterinarian.
EUTHANASIA:
Euthanasia of animals at the facility in Toronto was performed by gas anesthesia over-dosage (isoflurane) followed by exsanguination. Euthanasia of animals at the Montreal facility was performed by cervical dislocation.
TREATMENTS:
Treatments, dosing regimens, and group sizes are shown in Table 1. Apraglutide was provided by the manufacturer as a lyophilized powder and was reconstituted with vehicle (sterile water containing 4.5% D-Mannitol, 20mM glycine, 20mM L-histidine; pH 8.6–8.8).
Cytarabine and melphalan were both purchased from Sigma-Aldrich (Missouri, USA). Cytarabine was dissolved in sterile 0.9% NaCl solution with the pH adjusted to 7.35, while melphalan was prepared in acidified alcohol.
ETHICAL APPROVAL:
In-life procedures were approved by the Canadian Council for Animal Care Committee of the University Health Network, Toronto, Canada, under Animal Utilization Protocol #: 859.14, and of the Canadian Council for Animal Care Committee of the CIUSSS of l’Est-de-l’Ile-de-Montréal, Montréal, Canada, under protocols numbers 2017-MA-012 and 2017-MA-013.
EFFECT OF APRAGLUTIDE ON CHEMOTHERAPY-INDUCED GI DAMAGE: Sixty-two BALB/c male mice (21–26 g) aged 12–18 weeks were assigned to 1 of 4 treatment groups of 6–18 animals each, to compare the efficacy of apraglutide in reducing intestinal damage and protecting from bacterial infection of intestinal mucositis induced by cytarabine. Apraglutide 3.3 mg/kg [42] was administered subcutaneously before and during chemotherapy (from day −4 to day +12; either once daily or every 48–72 hours) or after initiation of treatment with cytarabine (from day 0 to day +12). Cytarabine (30 mg/kg) was administered to all groups twice a day for 5 consecutive days (days 0 to day +4). To evaluate recovery from neutropenia, 3 additional animals were added in selected groups (Table 1, Experiment 1).
The intestine-protective effect of apraglutide during preconditioning was also assessed in a different animal model, using 34 BALB/c male mice (10 animals per group); immunoablation was achieved by intraperitoneal administration of a single high dose of melphalan (17.5 mg/kg) on day 0, alone or in combination with apraglutide, and was compared with vehicle controls. The pharmacologic effect of subcutaneously administered apraglutide 3.3 mg/kg was assessed, with dosing every 48 hours starting at day −8 and continuing until day +6 (Table 1).
In a separate dose-response study, 132 BALB/c female mice (17–24 g) aged 8–11 weeks were assigned to 1 of 6 treatment groups of 16 animals each (plus 6 extra animals per group for serum citrulline measurements), to assess the pharmacologic effect of increasing doses of apraglutide (0.11, 0.3, and 1.1 mg/kg) administered subcutaneously. Cytarabine was administered intraperitoneally at 30 mg/kg twice daily for 5 days (day 0 to day +4). Apraglutide was administered daily (in all but 1 group, in which it was administered every 48–72 hours) for a total of 9 days, 4 days before and 5 days during the administration of chemotherapy (day −4 to day +4). The effect of apraglutide was compared with that of unmodified hGLP-2, which was administered twice daily from day −4 to day +4 at a nominal dose of 160 nmol/kg and combined with cytarabine (Table 1, Experiment 2).
MEASUREMENTS:
Parameters monitored during the in-life portion of these studies included mortality, clinical signs, and body weight. Mortality checks were performed once or twice daily for the duration of the studies. Clinical signs were recorded during daily cage side observations, and detailed clinical examination (DCE) was performed before initiation of treatment, during treatment days, and prior to autopsy. For animals in recovery groups, DCE was performed once weekly and before termination. The DCE focused on the presence of diarrhea, signs of dehydration, and cachexia wasting syndrome. Body weight was recorded on selected days during treatment and during the recovery period (when applicable), as well as at autopsy for all animals. Mice with weight loss greater than 25% or reaching other limit points were euthanized. All other mice were euthanized as previously scheduled. To perform bacterial phenotyping, fecal samples from selected animals were collected over approximately 24 hours pretreatment and on the day before scheduled euthanasia. Animals were euthanized the day after the last scheduled dose of apraglutide. At the end of the study, blood samples were collected (0.3 mL in K3EDTA) to measure the levels of circulating citrulline, which is known as a biomarker proportional to the intestinal mass. The analytical method for determining citrulline levels in mouse plasma was validated at York Bioanalytical Solutions (York, UK). The method employed protein precipitation with tandem mass spectrometry using turbo ionspray, in positive ion, multiple reaction monitoring mode. The lower limit of quantification of the method was 0.500 μg/mL; the sample aliquot volume was 25 μL.
Other blood samples (0.75 mL in EDTA) were dedicated to hematologic analysis. The impact of apraglutide on recovery from cytarabine-induced neutropenia was also assessed, by comparing the evolution of hematologic parameters for white blood cells following a 4-week recovery period for designated groups.
The composition of the fecal bacterial microbiota was investigated using high-throughput sequencing of variable regions of the 16S rDNA bacteria gene (taxonomic metasequencing analysis). Representations of the relative proportions of taxons in each sample were shown according to Phylum, Family, and Genus.
External examination, including identification of all clinically recorded lesions, and detailed internal examination were performed during autopsy. Intestinal segments were evaluated for signs of hemorrhage or inflammation, weighed, and their length measured; they were then fixed in formalin, paraffin embedded, sectioned, and stained with hematoxylin and eosin, to evaluate intestinal mucosa integrity.
EFFECT OF APRAGLUTIDE ON IRRADIATION- OR TRANSPLANTATION-INDUCED GI DAMAGE: Using a mouse model previously described by Thompson et al [43], the effect of apraglutide on GI protection following irradiation and allogeneic transplantation was assessed. Twenty (Experiment 1 [8.5 Gy]) and 25 (Experiment 2 [7.0 Gy]) BALB/cJ mice were weighed and randomized into 3 groups based on matching weights, so that each group contained a similar distribution of mouse weights. Mice received subcutaneous injections of apraglutide 3 mg/kg or vehicle from day −9 to day +7 post-allogenic transplantation. At day −1, all BALB/cJ mice from 2 out of the 3 groups were irradiated (7.0 or 8.5 Gy, LINAC X-ray source). At day 0, bone marrow and spleen T cells from C57BL/6J mice were collected, prepared, and transplanted into BALB/cJ mice (intravenous injection of 10 million bone marrow cells extracted from femurs and 2.5 million spleen cells; due to dehydration, intravenous injection was not possible in the mice receiving the cells by subcutaneous injection). To quantify the proportion of T cells in the spleen, 1×106 spleen cells were stained with anti-TCRβ PE antibody (control: 1×106 unstained spleen cells) and quantified by flow cytometry. The percentage of TCR+ cells was quantified with FlowJo Software (Becton, Dickinson and Company, USA). On the day of euthanasia, chimerism in BALB/c mice was measured by flow cytometry, by staining blood or spleen cells with antibodies to H2b (C57BL/6). The samples were assessed by flow cytometry at the Maisonneuve-Rosemont Hospital Research Center (Québec, Canada). The percentage of H2b+ cells was quantified with FlowJo Software. All irradiated mice showed presence of chimerism. The mice from the third group were neither irradiated nor transplanted, and they received subcutaneous injections of vehicle every second day starting from day −9 to day +7, matched with the irradiated groups (Table 1).
Intestinal symptoms, such as diarrhea and/or presence of blood in the feces, were recorded. At autopsy, the intestine was examined macroscopically for the presence of inflammation, necrosis, blood, or other alteration. Intestinal segments were collected and prepared for histopathology analysis. Results were presented as percentages of animals with pathologic severity scores from 0 to 4, with 4 being the most severe.
STATISTICAL ANALYSIS:
Animal survival data were analyzed using Kaplan-Meier plots (GraphPad Prism), with a log-rank test for trend and a log-rank (Mantel-Cox) test used to compare treatment groups. Mean and standard error of the mean (SEM) values were calculated for animal body weight throughout the studies. The body weight change on day 7 was calculated as:
Data for day 7 body weight change were statistically analyzed by one-way analysis of variance (ANOVA) with a Newman-Keuls multiple comparison post hoc test. Mean and SEM values for serum citrulline concentration were calculated for each of the 6 treatment groups and statistically analyzed, using one-way ANOVA with a Newman-Keuls multiple comparison post hoc test. Mean and SEM values for blood polymorphonuclear (PMN) cell count were calculated for each of the 6 treatment groups.
Results
Effect of Apraglutide on Chemotherapy-Induced GI Damage
IMPACT ON SURVIVAL: In the group treated with cytarabine only, some animals began to die 1 day after the last dose of chemotherapy, and no mice in this group were alive at 3 days. In all other groups (except control group), all animals had died by day +8, either due to toxicity or due to being euthanized for weight loss or other severe symptoms; mean survival was 7 days from start of treatment (Figure 1A).
Physical condition and survival rates were significantly (P<0.0001) improved when cytarabine treatment was combined with apraglutide injections administered prior to or at the same time as chemotherapy. When apraglutide treatment was initiated before chemotherapy and continued after initiation of chemotherapy, all animals but 1 survived to scheduled termination. However, when apraglutide administration was initiated on the first day of chemotherapy, 3/10 animals died on day 2 (Figure 1A).
Overall survival was significantly and dose dependently improved in the apraglutide treatment groups compared with animals treated with vehicle plus cytarabine. While only 5/16 animals survived in the vehicle plus cytarabine group at the end of the study, there were no deaths in the 3.3 mg/kg group (P<0.01), 14/16 survivors in the 1.1 mg/kg group (P<0.01), and 11/16 survivors in the 0.33 mg/kg group (P<0.05); 9/16 animals survived in the hGLP-2 plus cytarabine group (Figure 1B). No median survival time could be calculated. Improvement in survival with unmodified hGLP-2 was not statistically significant (Figure 1B).
Melphalan-only treatment resulted in premature euthanasia of 5/10 animals between days 4 and 7 post-chemotherapy, because of the severely compromised physical condition of the animals (Figure 1C). Survival was improved when melphalan was combined with pretreatment or concomitant treatment with apraglutide (Figure 1C).
EFFECT ON BODY WEIGHT: Cytarabine treatment alone induced body weight loss that was associated with a gradual deterioration in the clinical condition of the mice, and with a significant loss of body weight starting on the day following the first treatment with cytarabine (Figure 2A); body weight reached nadir on day 7. Preventive treatment with apraglutide 1.1 mg/kg or 3.3 mg/kg attenuated weight loss relative to cytarabine/vehicle-treated animals. On day 7, the body weight loss of the animals treated with the therapeutic regimens of apraglutide (1.1 mg/kg and 3.3 mg/kg) was significantly lower as compared with cytarabine alone. No difference was observed for the 0.33 mg/kg apraglutide dose level or for the group treated with hGLP-2 (Figure 2A). Treatment with apraglutide initiated pre-chemotherapy and continued after was associated with reduced body weight loss. Apraglutide treatment initiated concomitantly with cytarabine had no significant effect on the decrease of body weight (Figure 2B). Similar results were obtained when cytarabine was combined with increasing doses of apraglutide administered before initiation of chemotherapy and not continued after (data not shown). Overall survival was improved in the treatment groups relative to animals treated with vehicle plus cytarabine; a significant, dose-dependent difference compared with animals treated with vehicle plus cytarabine, as determined by a log-rank (Mantel-Cox) test, was observed for all apraglutide-treated groups but not for the group treated with hGLP-2. The median survival time for animals treated with vehicle plus cytarabine was 8 days, but it was not possible to calculate a survival time for the other groups because of the low level of mortality.
The mean body weight loss, between day 1 and day 4, of animals treated with melphalan alone was accompanied by a marked deterioration of clinical condition (Figure 2C). At day 4, the mean body weight of animals treated with melphalan 17.5 mg/kg was significantly decreased compared with controls (−17.3%; 20.9±2.3 g vs 27.0±0.9 g for controls; P<0.001). From day 5, mean body weight and clinical condition of surviving animals gradually improved. When the animals received melphalan in combination with apraglutide (3.3 mg/kg), body weight loss was less severe than for animals in the melphalan-only group at day 4 (−12.0%; 23.0±2.0 g vs 27.0±0.9 g for the controls; P<0.001). Body weight loss was further attenuated when animals were treated with melphalan in combination with apraglutide 17.5 mg/kg, with a mean body weight loss at day 4 of 2.5% (24.6±1.1 g vs 27.0±0.9 g for the control; P<0.001). In addition, mean body weight in this group was higher compared with that of the melphalan-only group (24.6±1.1 g vs 20.9±2.3 g).
EFFECT ON CYTARABINE-INDUCED LEUKOPENIA: Figure 3A shows the effect of cytarabine with and without apraglutide treatment on PMN cell count. With or without apraglutide administered before and during chemotherapy, there was an 80% decrease in leukocyte count at the end of cytarabine treatment (Figure 3B). The leukocyte counts returned to control levels after 4 weeks, indicating no detrimental effect of apraglutide on recovery of myelopoiesis and lymphocyte count. Similar results were also obtained with animals treated with melphalan 17.5 mg/kg, alone or in combination with apraglutide (not shown).
EFFECT ON INTESTINAL MORPHOLOGY: Treatment with cytarabine induced pathological changes in intestinal morphology, including villous atrophy (duodenum, jejunum, and ileum), villous epithelium vacuolation (duodenum, jejunum, and ileum), regenerative cryptal hyperplasia (jejunum), cryptal necrosis/degeneration (duodenum, jejunum, and ileum), cryptal atrophy (jejunum and ileum), and mucosal atrophy/submucosal edema (cecum) (Figure 4A). In mice that received cytarabine in combination with apraglutide 3.3 mg/kg, there were no duodenal findings and a low incidence and severity of jejunal changes. Intraperitoneal administration of melphalan was associated with degenerative/inflammatory mucosal changes in the intestine (duodenum, jejunum, ileum, cecum, and/or colon). The degenerative and inflammatory mucosal changes were characterized by degeneration and necrosis of the crypt epithelium, mixed or mononuclear infiltrate in the lamina propria, decreased number of crypts, shortening of villi (villous atrophy), vacuolation of the villous epithelium, regenerative cryptal hyperplasia, and/or mucosal erosion (Figure 4A). Such pathological features were greatly reduced or absent in mice treated with melphalan in combination with apraglutide and in control mice not treated with melphalan (Figure 4B).
EFFECT ON INTESTINAL EPITHELIUM MASS: Serum citrulline was significantly decreased in all mice receiving either cytarabine or melphalan (not shown) compared with control mice. Improvements in citrulline concentrations were observed when cytarabine was administered in combination with apraglutide 0.33 mg/kg or 1.1 mg/kg, compared with cytarabine alone (Figure 5).
Chemotherapy with melphalan was also associated with a 50% decrease in serum citrulline compared with control (29.2±19.3 μM vs 58.5±16.8 μM, respectively). Plasma levels of citrulline were unaffected when melphalan was given concomitantly with apraglutide (administered before and during chemotherapy).
EFFECT ON THE INTESTINAL MICROBIOTA: In laboratory mice, the intestinal microbiota is largely composed of Firmicutes spp. (gram-positive, aerobic and anaerobic bacteria) and Bacteroidetes spp. (gram-negative, anaerobic bacteria), the latter consisting of several families of opportunistic pathogenic bacteria. As intestinal microbiota and fecal microbiota have been shown to be closely related in other GI conditions, the fecal microbiota can be used as an indicative measure of the intestinal microbiota [44]. Treatment with cytarabine alone induced a profound modification of the composition of the intestinal microbiota in all taxonomic levels, with a significant decrease in the Firmicitus population and an increase in the Bacteroidetes at the Phylum level (Figure 6). In contrast, the relative proportion of fecal bacterial populations tended to normalize when treatment with cytarabine was combined with treatment with apraglutide starting before chemotherapy and continuing during chemotherapy. Preventive treatment with apraglutide also resulted in the physical preservation of the intestinal structure and in preservation of the global homeostatic environment of the intestinal microbiota.
EFFECT ON SURVIVAL FOLLOWING ALLO-HSCT: BALB/cJ mice that received no irradiation and no BMT had a survival of 100% at day 14 (Figure 7). All BALB/cJ mice that received pre-transplant total body irradiation (TBI) at a dose of 7 Gy and cells from C57BL/6J mice (TBI-BMT), but that did not receive apraglutide, died by day 9. These survival results are similar to those reported by Thompson et al [43]. TBI-BMT mice receiving apraglutide 3.3 mg/kg showed prolonged survival compared with mice not receiving apraglutide. Median survival was similar between the 2 groups: 9 days for the TBI-BMT plus apraglutide group (40% of apraglutide-treated animals survived after day 9) vs 8.5 days for the TBI-BMT group. Animals having long-term survival after day 9 also showed a gain in weight (data not shown).
Overall, the GI pathological score was more favorable in TBI-BMT animals treated with apraglutide 3.3 mg/kg (group A; 4/10 animals with score of 0) vs vehicle (group B; 1/10 animals with score of 0) (Figure 8).
At 8.5 Gy TBI, histological examination of the small intestine (jejunum only) showed that TBI treatment followed by allo-HSCT induced significant morphological modification of the cellular components characteristic of aGvHD (Figure 9). In TBI/transplanted animals treated with apraglutide 3.3 mg/kg, the overall mean severity score of mucosal degenerative/inflammatory changes (shortening of villi [villous atrophy], mononuclear [lymphohistiocytic]/neutrophilic cell infiltrate in the lamina propria/intra-cryptal epithelium, decreased number of crypts, and cryptal abscess) was decreased in the intestine compared with the TBI/transplanted animals treated with vehicle only. Additionally, the mean score of regenerative crypt hyperplasia was slightly increased compared with animals treated with vehicle only. The data presented in Figure 10 represent the percentages of animals corresponding to each histological grade (minimal [+1], mild [+2], moderate [+3], marked [+4], and severe [+5]) for each of the histological parameters (single cell necrosis, necrosis of all crypts, shortening of villi, cryptal hyperplasia, cell infiltrate, cryptal abscess, etc.).
EFFECT OF APRAGLUTIDE ON COLON LENGTH FOLLOWING IRRADIATION AND ALLOGENEIC TRANSPLANTATION:
Colon length measured at euthanasia is depicted for each mouse in Figure 11. The mean length of the colon of TBI-BMT mice (7.0 Gy) treated with apraglutide was similar to the length of animals that had not been irradiated and transplanted (8.6±0.35 cm vs 9.6±0.33, respectively). In contrast, the length of the colon of TBI-BMT mice treated only with vehicle was significantly shorter (7.19±0.10 cm) as compared with the 2 other groups.
Discussion
In allo-HSCT recipients, the GI tract is a tissue system damaged by conditioning regimens and aGvHD. These dual mechanisms of GI damage markedly contribute to the observed morbidity and mortality among patients with aGvHD after allo-HSCT [13,45]. The vital intestinal L-cells, which secrete GLP-2, an essential endocrine hormone that maintains GI integrity and nutrient/fluid absorption as well as that repairs and regenerates cells that sustain healthy intestinal epithelium, are directly impacted [31].
In the series of experiments presented here, the data show that the GLP-2 analog apraglutide, when administered in combination with chemotherapy, significantly improves the survival of chemotherapy-exposed mice, promotes recovery from chemotherapy-induced weight loss, exerts protective effects on epithelial structure by reducing chemotherapy-induced degenerative intestinal changes, maintains plasma citrulline levels, which is indicative of mucosal mass preservation, and preserves intestinal bacterial homeostasis during chemotherapy. In the context of chemotherapy alone, the administration of apraglutide preserved the intestinal epithelium from damage induced by standard clinical approaches used in the treatment of hematological cancers and significantly improved the physical condition of animals.
Apraglutide showed a significant protective effect against total body irradiation and allogeneic transplant-induced mortality, potentially through preserving intestinal integrity, as evidenced by reduced villi atrophy and decreased colon shortening.
Previous studies have examined the beneficial effects of GLP-2 on survival following radiation burn injuries in mice [46]. In the study presented here, adding apraglutide treatment to cytarabine or melphalan as well as to irradiation followed by allogeneic transplantation improved survival rates. As far as we are aware, this is the first time that improved survival with GLP-2 peptides has been reported for the chemotherapy agents cytarabine and melphalan, which are commonly used in the patient population of interest; however, improved survival has been reported with GLP-2 in mice following chemotherapy with irinotecan, a topoisomerase inhibitor [47].
Apraglutide treatment reduced body weight loss experienced with cytarabine or melphalan chemotherapy but did not impact weight loss following irradiation and allogeneic transplantation. The reduction of chemotherapy-induced weight loss did not appear to relate to food consumption; therefore, it is likely that this effect is due to preserved intestinal function in the way of nutrient absorption, and lack of chemotherapy-induced diarrhea, following apraglutide treatment. This is supported by evidence that endogenous GLP-1 and GLP-2 are key to gut healing after intestinal injury in mice [48], as demonstrated by preservation and/or restoration of citrulline levels, a biomarker indicative of the functional and mass integrity of the intestinal mucosa. It is unclear why apraglutide did not impact irradiation and allogeneic transplant-induced weight loss, as functional improvements in the intestine, in terms of increased colon length, were observed in this model.
In other studies, the authors have suggested that the protective effects of GLP-1 and GLP-2 on radiation-induced oxidative injury of the intestine are due to the inhibition of neutrophil infiltration and subsequent inflammatory responses [49]. The results presented here support an alternate explanation: apraglutide prevents direct drug- or irradiation-induced damage of epithelial cells and therefore preserves the intestinal mucosa, which maintains the normal microbiota structure and limits bacterial invasion below the epithelium [50] – the latter limits neutrophil response, infiltration, and further inflammation within the GI tract. The lack of protection seen with irradiation and allo-HSCT may be due to the damage to other parts of the GI tract, such as mouth, esophagus, and stomach and bladder, which are not protected by GLP-2, allowing for bacterial translocation and death due to sepsis.
Administration of cytarabine suppresses myelopoiesis and decreases blood counts, ie it elicits severe neutropenia. As noted, apraglutide did not affect the depletion of PMN cells when administered before and in conjunction with cytarabine. These results suggest that the improvements in animal survival and body weight do not result from improved neutrophil granulocyte count but, rather, from maintenance of GI integrity and a lack of neutrophil-induced inflammation and bacterial invasion that result in the death of animals.
Around 80% of individuals undergoing cancer treatment experience chemotherapy-induced GI toxicity (CIGT), which is thought to reflect the interaction of changes in the gut microbiome [51]. Apraglutide attenuates the negative impact of cytarabine on the intestinal microbiota, suggesting that it might have a beneficial impact on CIGT.
In addition to GI-associated infections, damage of intestinal tissue during preconditioning for allogeneic transplantation is reported as contributing to the ‘cytokine storm’ that is associated with the pathophysiologic mechanism leading to aGvHD. In fact, increasing evidence from experimental and clinical BMT settings suggests that damage to the GI tract plays a major pathophysiologic role in the development and amplification of aGvHD [52]. Studies have demonstrated that during aGvHD, the intestinal stem cell compartment is particularly injured, affecting several cell types, including the Paneth cells, which are responsible for the secretion of antimicrobial molecules (such as REG3A). Decrease in these cells levels correlates with the severity of the disease [52]. Therefore, a reduction in GI tract damage would be predicted to prevent systemic lipopolysaccharide translocation and thus reduce inflammatory cytokine production, culminating in decreased GI tract damage and mortality from GvHD [51,52].
Conclusions
In conclusion, apraglutide protects intestinal function and improves survival following chemotherapy with cytarabine or melphalan as well as after irradiation plus allogeneic transplant. Given that GI toxicity is a common problem with cancer treatments, the potential benefits of apraglutide in this area warrant further investigation.
Figures
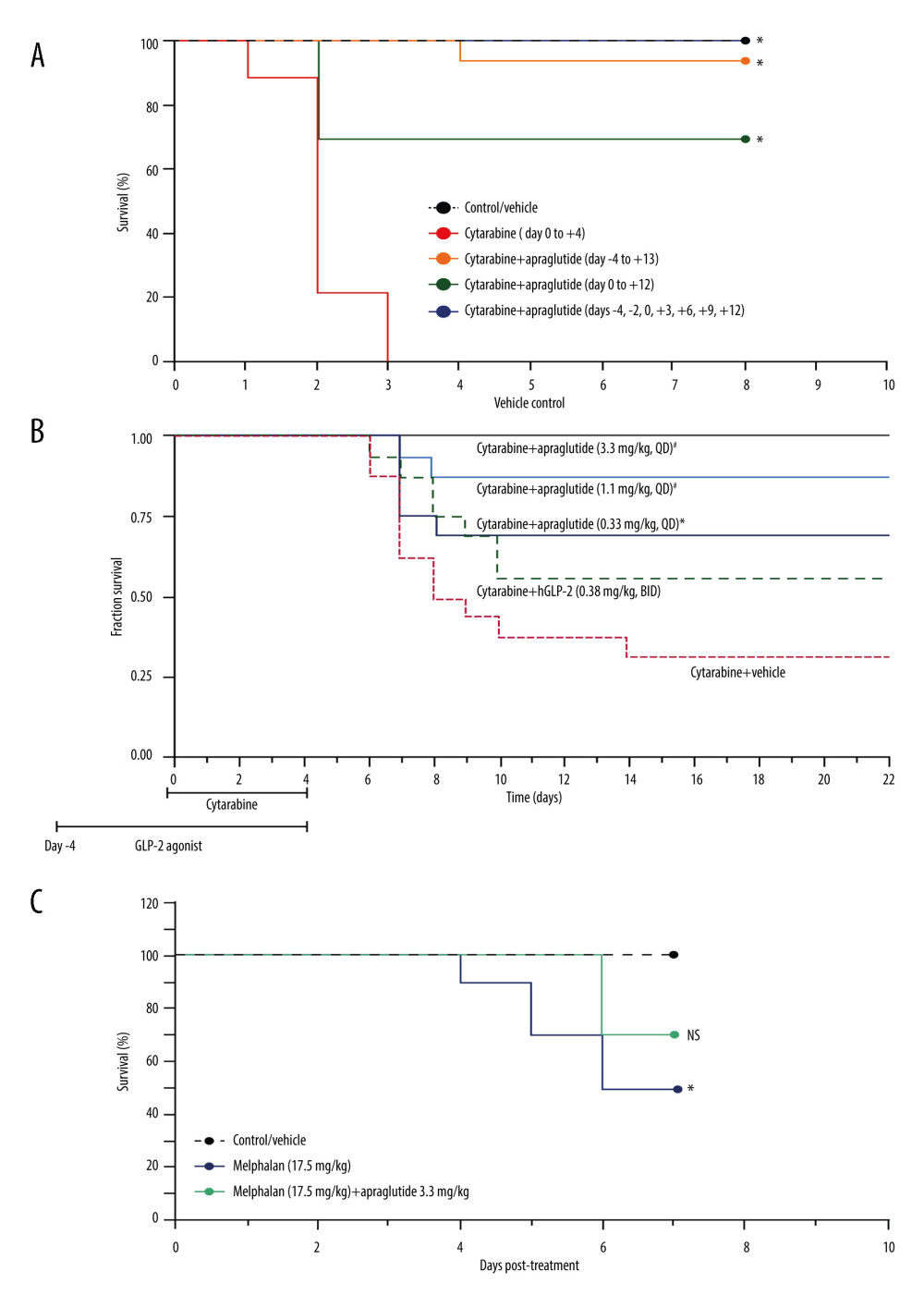 Figure 1. Effect of cytarabine or melphalan±apraglutide on survival. Effect of cytarabine with or without apraglutide (3.3 mg/kg) on survival (group with daily dosing of apraglutide from day −4 not shown) (A); effect of cytarabine without apraglutide or with different doses of apraglutide on survival (B); and effect of melphalan with or without apraglutide 3.3 mg/kg on survival (high dose group 17.5 mg/kg apraglutide not shown) (C). (A) Kaplan-Meier curves. Animal survival was monitored daily. n=6–18 at time=0 for each treatment group. Apraglutide treatment initiated either before or concomitantly with the chemotherapy, showed significant difference relative to animals treated with cytarabine alone, as determined by log-rank (Mantel-Cox) test. When comparing to the vehicle/control group, survival of animals treated with cytarabine only was significantly different, as determined by log-rank (Mantel-Cox) test. No statistical difference was observed between the vehicle/control group and the groups that were treated with apraglutide. * P<0.0001. (B) Kaplan-Meier curves. GLP-2 receptor agonists (apraglutide, hGLP-2) were administered 4 days before and 5 days during cytarabine chemotherapy treatment. Animal survival was monitored daily. n=16 at time=0 for each treatment group; significant difference relative to vehicle/cytarabine-treated animals as determined by log-rank (Mantel-Cox) test. * P<0.05, # P<0.01. (C) Kaplan-Meier curves. Animal survival was monitored daily. n=10 at time=0 for each treatment group. When comparing to the vehicle/control group, survival of animals treated only with melphalan was significantly different as determined by log-rank (Mantel-Cox) test. No statistical difference was observed between the vehicle/control group or the melphalan-only group and the group treated with apraglutide 3.3 mg/kg. * P≤0.001. BID – twice daily; QD – once daily.
Figure 1. Effect of cytarabine or melphalan±apraglutide on survival. Effect of cytarabine with or without apraglutide (3.3 mg/kg) on survival (group with daily dosing of apraglutide from day −4 not shown) (A); effect of cytarabine without apraglutide or with different doses of apraglutide on survival (B); and effect of melphalan with or without apraglutide 3.3 mg/kg on survival (high dose group 17.5 mg/kg apraglutide not shown) (C). (A) Kaplan-Meier curves. Animal survival was monitored daily. n=6–18 at time=0 for each treatment group. Apraglutide treatment initiated either before or concomitantly with the chemotherapy, showed significant difference relative to animals treated with cytarabine alone, as determined by log-rank (Mantel-Cox) test. When comparing to the vehicle/control group, survival of animals treated with cytarabine only was significantly different, as determined by log-rank (Mantel-Cox) test. No statistical difference was observed between the vehicle/control group and the groups that were treated with apraglutide. * P<0.0001. (B) Kaplan-Meier curves. GLP-2 receptor agonists (apraglutide, hGLP-2) were administered 4 days before and 5 days during cytarabine chemotherapy treatment. Animal survival was monitored daily. n=16 at time=0 for each treatment group; significant difference relative to vehicle/cytarabine-treated animals as determined by log-rank (Mantel-Cox) test. * P<0.05, # P<0.01. (C) Kaplan-Meier curves. Animal survival was monitored daily. n=10 at time=0 for each treatment group. When comparing to the vehicle/control group, survival of animals treated only with melphalan was significantly different as determined by log-rank (Mantel-Cox) test. No statistical difference was observed between the vehicle/control group or the melphalan-only group and the group treated with apraglutide 3.3 mg/kg. * P≤0.001. BID – twice daily; QD – once daily.  Figure 2. Effect of cytarabine or melphalan±apraglutide treatment on body weight change. Effect of cytarabine with or without apraglutide on body weight change at day 7 (A); effect of cytarabine with or without apraglutide on body weight change (B); and effect of melphalan with or without apraglutide on body weight change (C). (A) Data are presented as mean±SEM values (n=12–16 per group). * Significant difference relative to cytarabine/vehicle-treated animals as determined by one-way ANOVA and Newman-Keuls multiple comparison post hoc analysis. (B) Animal body weight was monitored daily. n=6–18 at time=0 for each treatment group. Data are shown as mean±SEM values. The body weight change of animals treated with cytarabine alone or in combination with apraglutide was significantly lower as compared with control/vehicle animals (statistics not shown). (C) Animal body weight was monitored daily. n=10 at time=0 for each treatment group. Data are shown as mean±SEM values. Data were analyzed using the unpaired t-test per row (plus Holm-Sidak method for multiple comparisons correction); indicates days of treatment with apraglutide. * P≤0.001 vs control. NS – non-significant; LYMPH – lymphocytes; NEUT – neutrophils; recov – recovery; WBC – white blood cells.
Figure 2. Effect of cytarabine or melphalan±apraglutide treatment on body weight change. Effect of cytarabine with or without apraglutide on body weight change at day 7 (A); effect of cytarabine with or without apraglutide on body weight change (B); and effect of melphalan with or without apraglutide on body weight change (C). (A) Data are presented as mean±SEM values (n=12–16 per group). * Significant difference relative to cytarabine/vehicle-treated animals as determined by one-way ANOVA and Newman-Keuls multiple comparison post hoc analysis. (B) Animal body weight was monitored daily. n=6–18 at time=0 for each treatment group. Data are shown as mean±SEM values. The body weight change of animals treated with cytarabine alone or in combination with apraglutide was significantly lower as compared with control/vehicle animals (statistics not shown). (C) Animal body weight was monitored daily. n=10 at time=0 for each treatment group. Data are shown as mean±SEM values. Data were analyzed using the unpaired t-test per row (plus Holm-Sidak method for multiple comparisons correction); indicates days of treatment with apraglutide. * P≤0.001 vs control. NS – non-significant; LYMPH – lymphocytes; NEUT – neutrophils; recov – recovery; WBC – white blood cells. 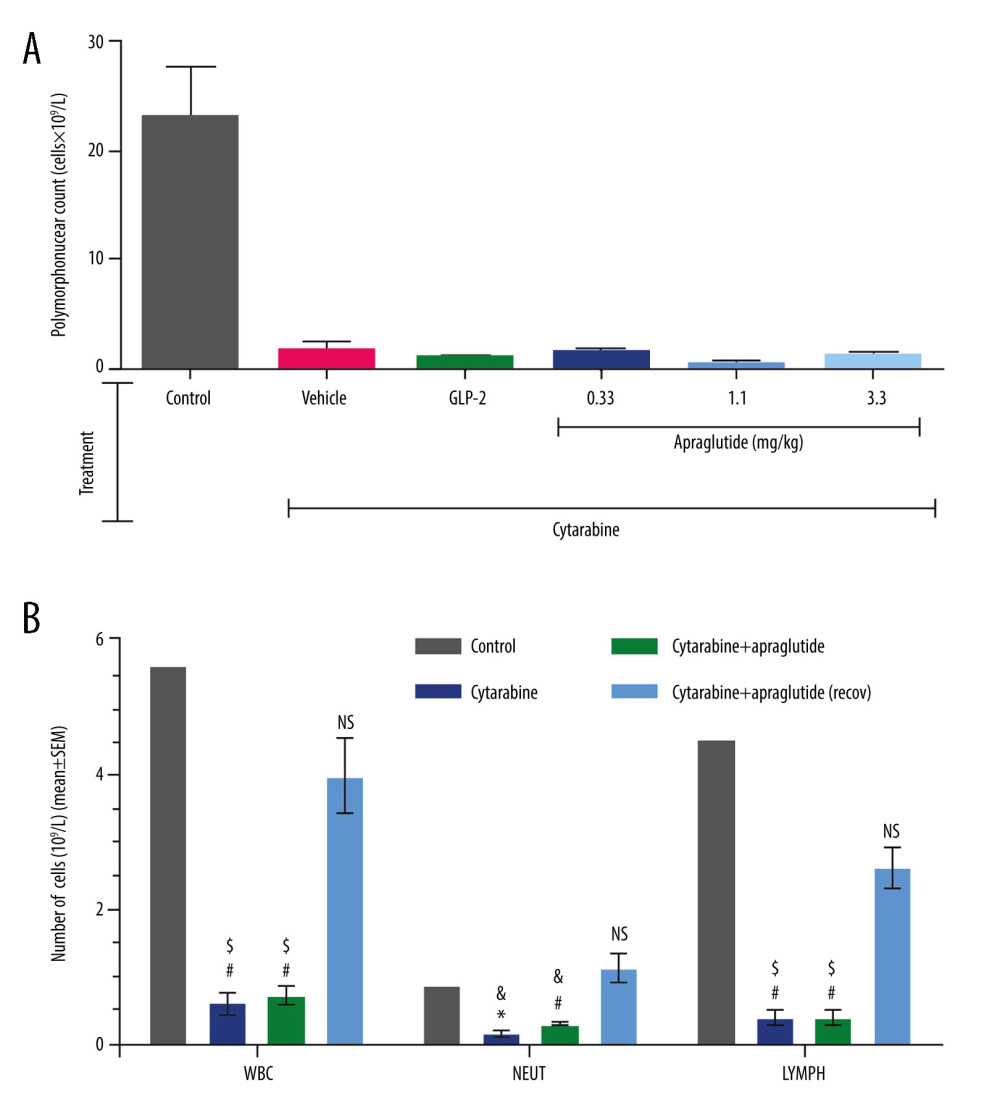 Figure 3. Effect of apraglutide on leukopenia in BALB/c mice. Effect on polymorphonuclear cell count following chemotherapy (A) and effect on the myelosuppressive activity of cytarabine (B). (A) Treatment group mean±SEM are shown (n=6 per treatment group); cell counts were determined in specifically designated animals. (B) Immunosuppressive activity was monitored at the end of the study. Samples were collected at euthanasia (n=3). Data are shown as mean±SEM values. As determined by the unpaired t-test according to the Holm-Sidak method for multiple comparisons, the mean number of WBC, NEUT, and LYMPH was significantly decreased in animals treated with cytarabine alone or in combination with apraglutide, compared with the control (* P<0.05, # P<0.01) and recovery groups (& P<0.05, $ P<0.01). No difference was observed between animals treated with cytarabine alone or in combination with apraglutide. No difference was observed either between the control mice and those in the recovery group treated with cytarabine plus apraglutide (NS).
Figure 3. Effect of apraglutide on leukopenia in BALB/c mice. Effect on polymorphonuclear cell count following chemotherapy (A) and effect on the myelosuppressive activity of cytarabine (B). (A) Treatment group mean±SEM are shown (n=6 per treatment group); cell counts were determined in specifically designated animals. (B) Immunosuppressive activity was monitored at the end of the study. Samples were collected at euthanasia (n=3). Data are shown as mean±SEM values. As determined by the unpaired t-test according to the Holm-Sidak method for multiple comparisons, the mean number of WBC, NEUT, and LYMPH was significantly decreased in animals treated with cytarabine alone or in combination with apraglutide, compared with the control (* P<0.05, # P<0.01) and recovery groups (& P<0.05, $ P<0.01). No difference was observed between animals treated with cytarabine alone or in combination with apraglutide. No difference was observed either between the control mice and those in the recovery group treated with cytarabine plus apraglutide (NS). 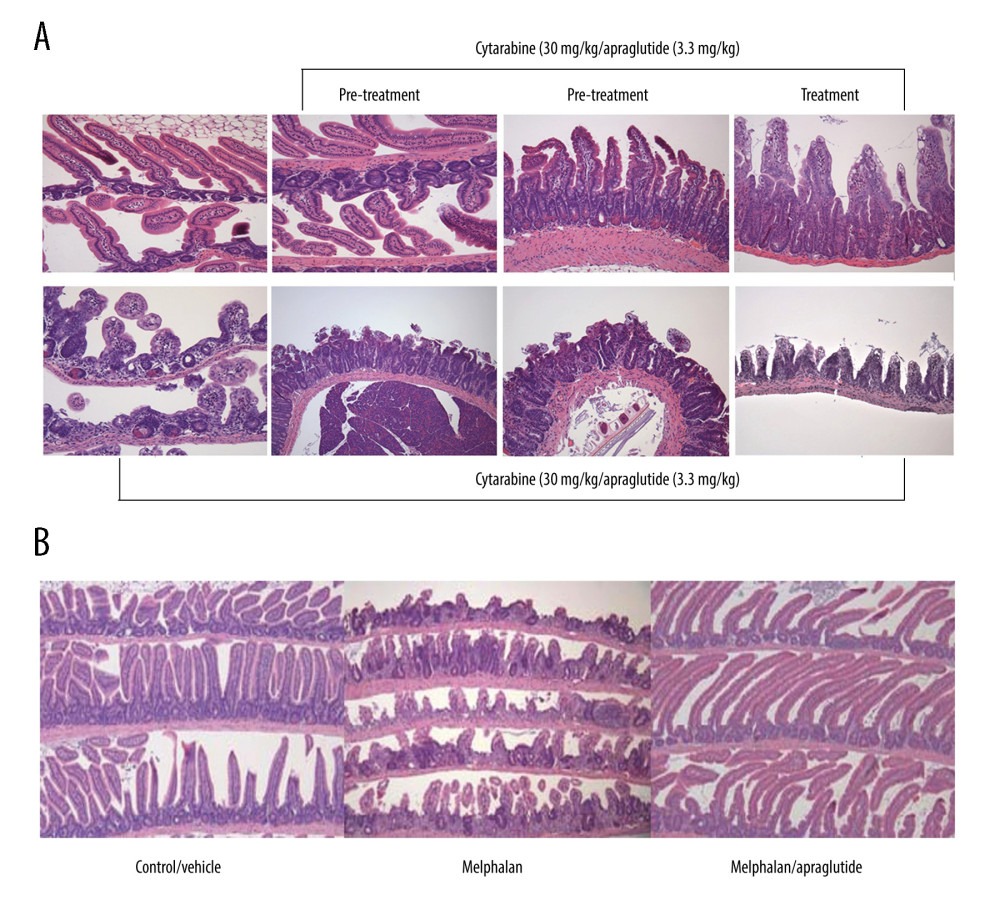 Figure 4. Apraglutide protects gastrointestinal epithelium structure from chemotherapy-induced injury. Representative micrographs of small intestine from animals treated with cytarabine (A) or melphalan (B), with and without apraglutide.
Figure 4. Apraglutide protects gastrointestinal epithelium structure from chemotherapy-induced injury. Representative micrographs of small intestine from animals treated with cytarabine (A) or melphalan (B), with and without apraglutide. 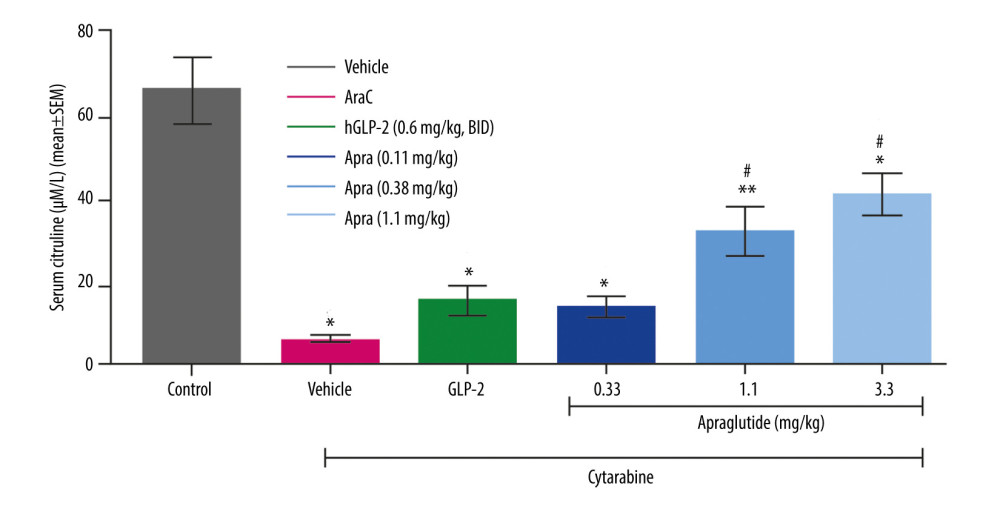 Figure 5. Dose-dependent effect of apraglutide on serum citrulline concentration following treatment with cytarabine. Data are shown as treatment group mean±SEM values. n=3 per treatment group; citrulline levels were only determined in specifically designated animals. * Significant difference relative to vehicle-only control animals. # Significant difference relative to the cytarabine/vehicle-treated animals, as determined by one-way ANOVA and Newman-Keuls multiple comparison post hoc analysis. BID – twice daily; SEM – standard error of mean.
Figure 5. Dose-dependent effect of apraglutide on serum citrulline concentration following treatment with cytarabine. Data are shown as treatment group mean±SEM values. n=3 per treatment group; citrulline levels were only determined in specifically designated animals. * Significant difference relative to vehicle-only control animals. # Significant difference relative to the cytarabine/vehicle-treated animals, as determined by one-way ANOVA and Newman-Keuls multiple comparison post hoc analysis. BID – twice daily; SEM – standard error of mean. 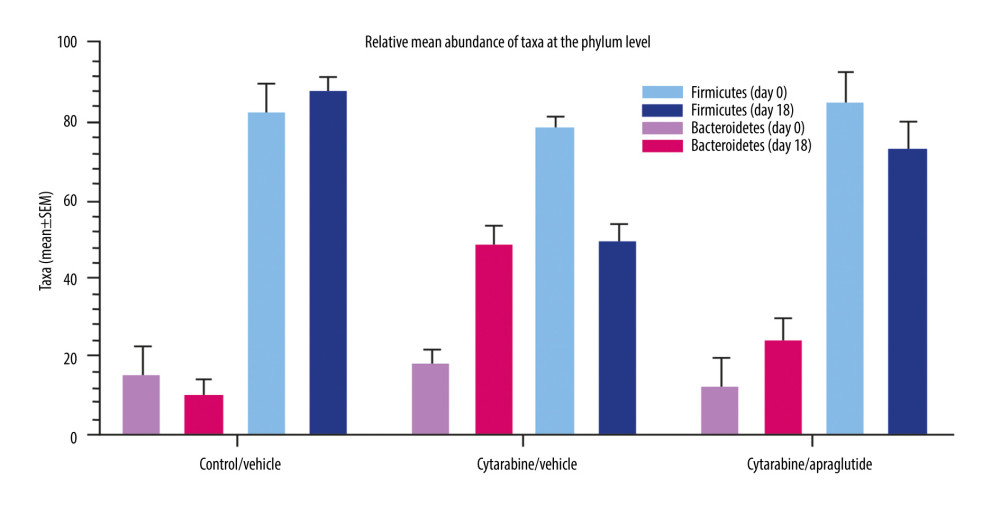 Figure 6. Effect of apraglutide on the diversity of the intestinal microbiota after chemotherapy (relative mean abundance of taxa in feces at the phylum level). SD – standard deviation; SEM – standard error of mean.
Figure 6. Effect of apraglutide on the diversity of the intestinal microbiota after chemotherapy (relative mean abundance of taxa in feces at the phylum level). SD – standard deviation; SEM – standard error of mean.  Figure 7. Effect of apraglutide on survival in TBI/BMT-treated mice (TBI 7 Gy). Kaplan-Meier curves. Animal survival was monitored daily. n=10 at time=0 for the irradiated groups and n=5 for the control group. Survival of animals treated with apraglutide initiated before TBI/BMT showed significant difference relative to TBI/BMT animals, as determined by log-rank (Mantel-Cox) test, but the difference was not significant compared with control animals. When comparing to the control group, survival of TBI/BMT was significantly different. TBI/BMT – total body irradiation/bone marrow transplantation.
Figure 7. Effect of apraglutide on survival in TBI/BMT-treated mice (TBI 7 Gy). Kaplan-Meier curves. Animal survival was monitored daily. n=10 at time=0 for the irradiated groups and n=5 for the control group. Survival of animals treated with apraglutide initiated before TBI/BMT showed significant difference relative to TBI/BMT animals, as determined by log-rank (Mantel-Cox) test, but the difference was not significant compared with control animals. When comparing to the control group, survival of TBI/BMT was significantly different. TBI/BMT – total body irradiation/bone marrow transplantation. 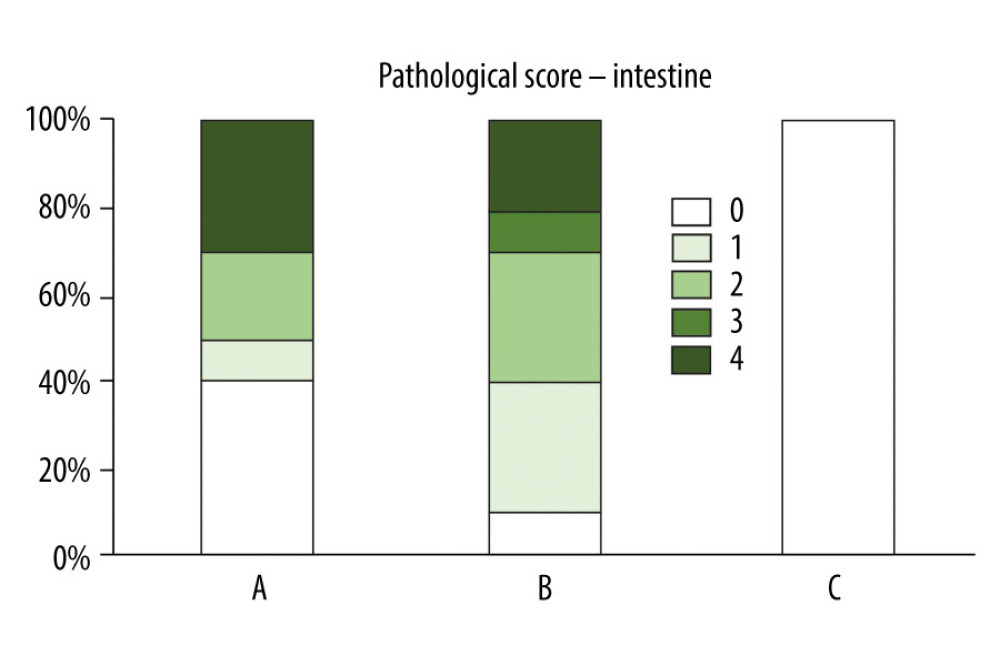 Figure 8. Apraglutide improves gastrointestinal pathological score following induction of aGvHD (TBI 7 Gy). Group A: TBI/transplanted mice treated with apraglutide; Group B: TBI/transplanted mice treated with vehicle; Group C: control mice treated with vehicle only and no transplantation. GvHD – graft-versus-host disease; TBI – total body radiation.
Figure 8. Apraglutide improves gastrointestinal pathological score following induction of aGvHD (TBI 7 Gy). Group A: TBI/transplanted mice treated with apraglutide; Group B: TBI/transplanted mice treated with vehicle; Group C: control mice treated with vehicle only and no transplantation. GvHD – graft-versus-host disease; TBI – total body radiation. 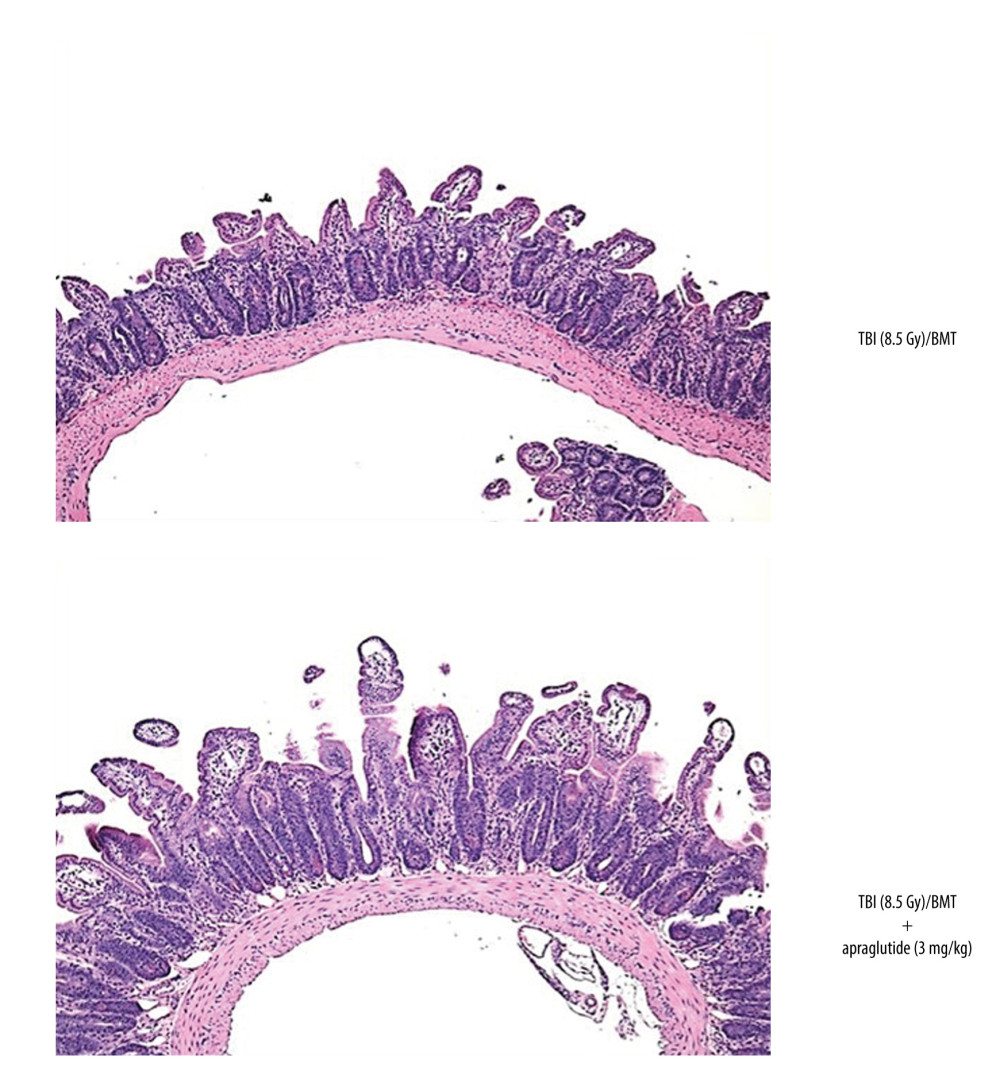 Figure 9. Morphological changes induced by total body irradiation followed by allogenic bone marrow transplantation and protective effect of apraglutide (TBI 8.5 Gy).
Figure 9. Morphological changes induced by total body irradiation followed by allogenic bone marrow transplantation and protective effect of apraglutide (TBI 8.5 Gy). 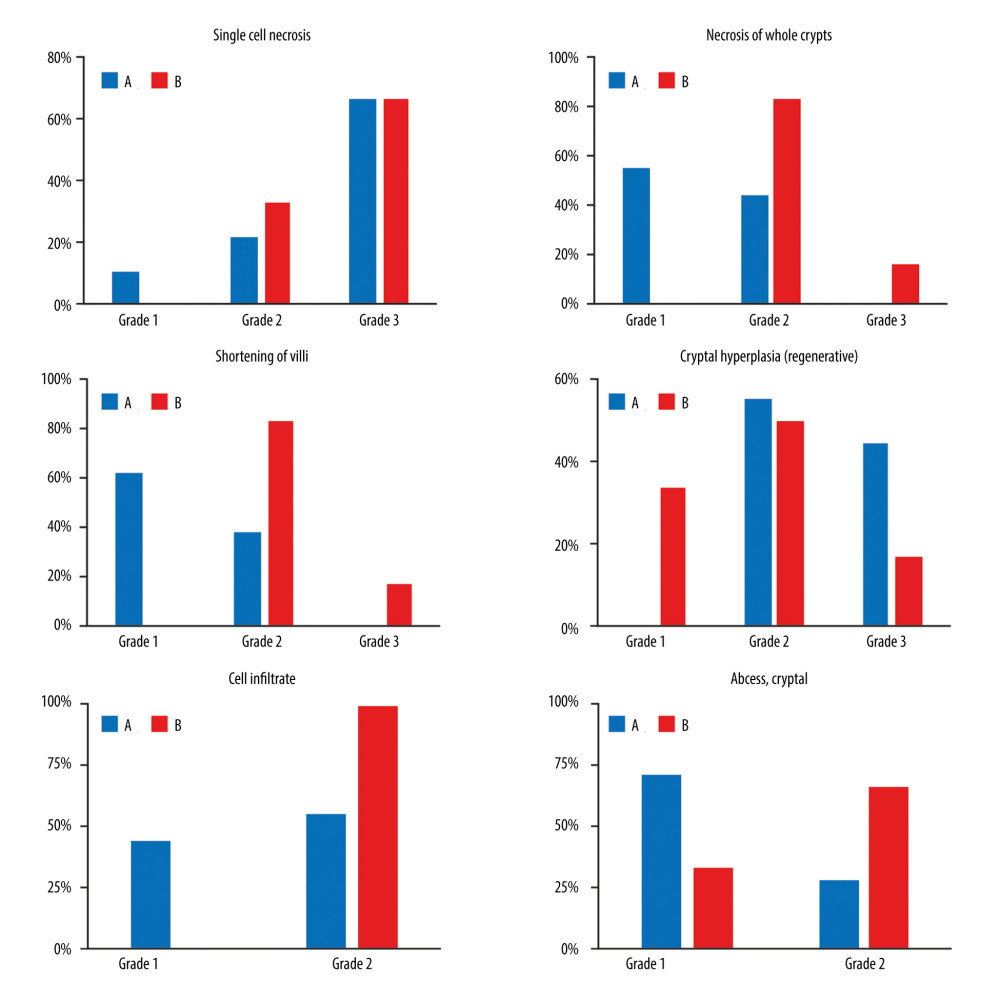 Figure 10. Effect of apraglutide on morphological damage of the jejunum and histological score induced by TBI (8.5 Gy) followed by allogeneic transplantation. Group A: TBI/transplanted mice treated with apraglutide; Group B: TBI/transplanted mice treated with vehicle. TBI at 8.5 Gy was applied. TBI – total body irradiation.
Figure 10. Effect of apraglutide on morphological damage of the jejunum and histological score induced by TBI (8.5 Gy) followed by allogeneic transplantation. Group A: TBI/transplanted mice treated with apraglutide; Group B: TBI/transplanted mice treated with vehicle. TBI at 8.5 Gy was applied. TBI – total body irradiation. 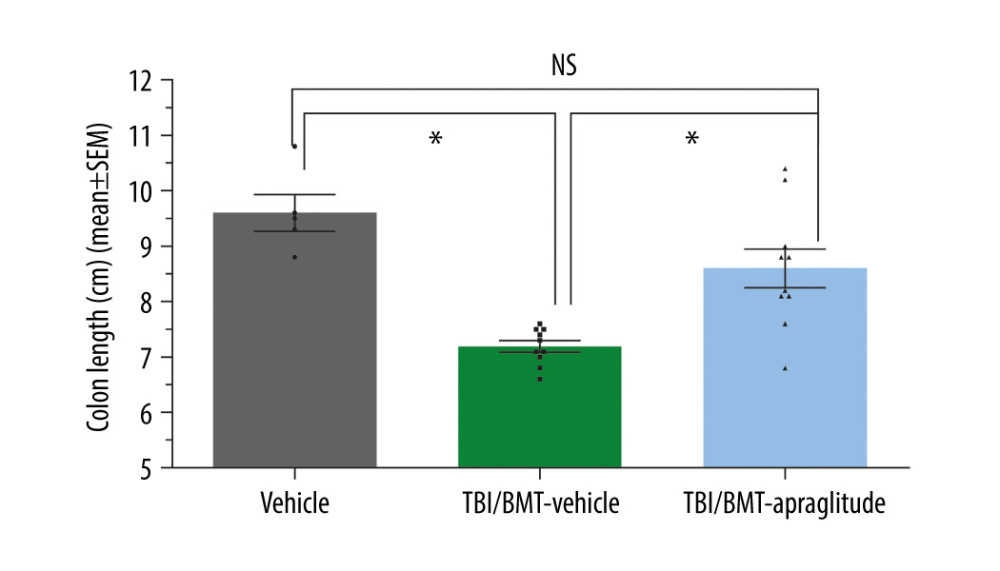 Figure 11. Effect of apraglutide on colon length following TBI and allogeneic transplantation. Data are shown as mean±SEM values for length of intestinal colon. n=5–10 per group. Each dot represents data for one mouse. Data show that the length of the colon of TBI/BMT animals was significantly shorter as compared with the vehicle group or the TBI/BMT group treated with apraglutide (Brown-Forsythe and Welch ANOVA tests). No difference was observed between the vehicle group and the TBI/BMT animals treated with apraglutide. TBI at 7.0 Gy was applied. * P<0.01. ANOVA – analysis of variance; SEM4– standard error of mean; TBI – total body irradiation.
Figure 11. Effect of apraglutide on colon length following TBI and allogeneic transplantation. Data are shown as mean±SEM values for length of intestinal colon. n=5–10 per group. Each dot represents data for one mouse. Data show that the length of the colon of TBI/BMT animals was significantly shorter as compared with the vehicle group or the TBI/BMT group treated with apraglutide (Brown-Forsythe and Welch ANOVA tests). No difference was observed between the vehicle group and the TBI/BMT animals treated with apraglutide. TBI at 7.0 Gy was applied. * P<0.01. ANOVA – analysis of variance; SEM4– standard error of mean; TBI – total body irradiation. Tables
Table 1. Treatment regimens.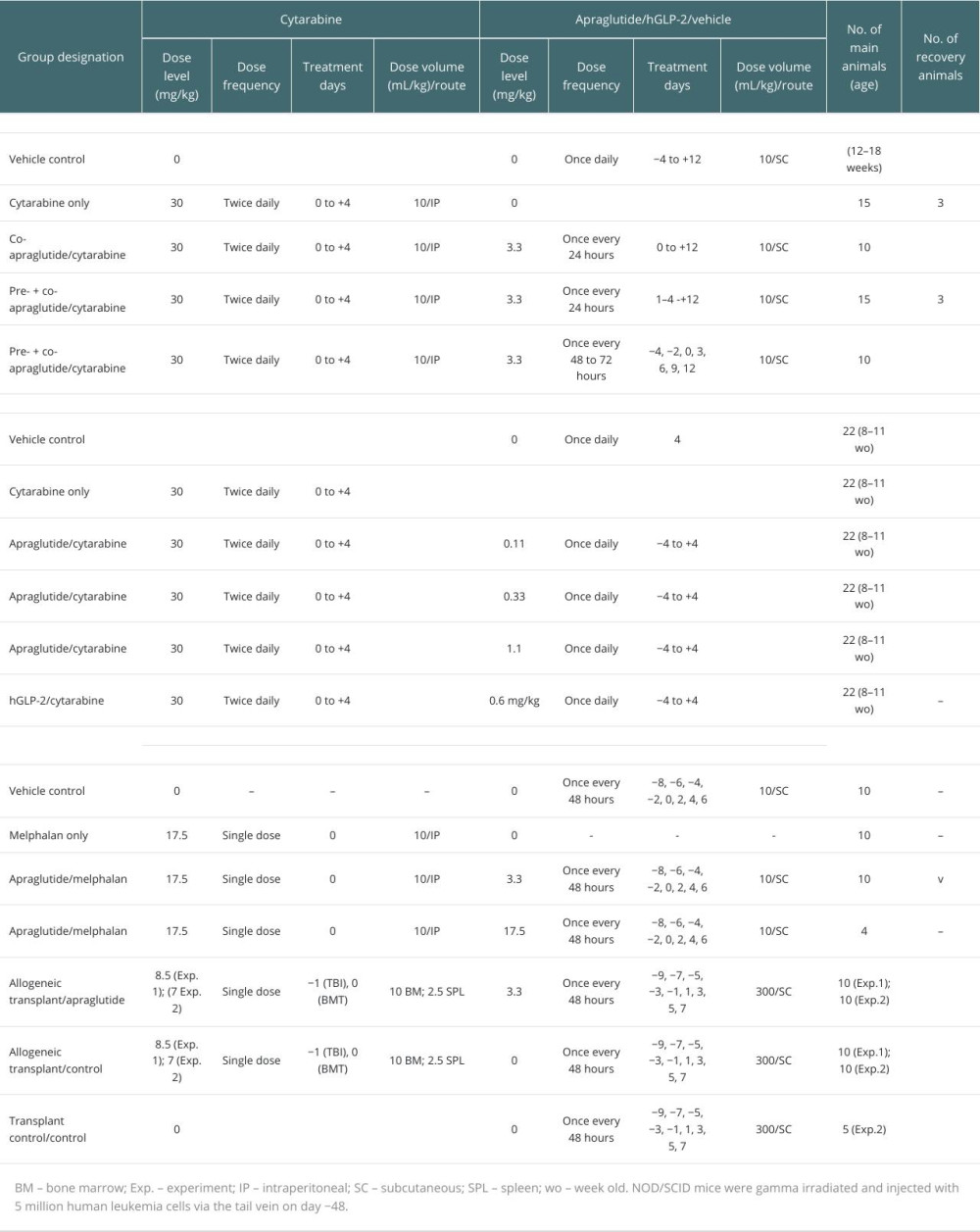
References
1. D’Souza A, Fretham C, Lee SJ, Current use of and trends in hematopoietic cell transplantation in the United States: Biol Blood Marrow Transplant, 2020; 26; 177-72
2. Zeiser R, Blazar BR, Acute Graft-versus-host disease – biologic process, prevention, and therapy: N Eng J Med, 2017; 377; 2167-279
3. Ferrara JL, Levine JE, Reddy P, Holler E, Graft-versus-host disease: Lancet, 2009; 373; 1550-61
4. Zeiser R, Polverelli N, Ram Rfor the REACH3 Investigators, Ruxolitinib for glucocorticoid-refractory chronic graft-versus-host disease: N Eng J Med, 2021; 385; 228-38
5. Loke J, Buka R, Craddock C, Allogeneic stem cell transplantation for acute myeloid leukemia: Who, when, and how?: Front Immunol, 2021; 12; 659595
6. Khorochkov A, Prieto J, Singh KB, The role of allogeneic stem cell transplantation in multiple myeloma: A systematic review of the literature: Cureus, 2021; 13; e18334
7. Greil C, Engelhardt M, Ihorst G, Allogeneic transplantation of multiple myeloma patients may allow long-term survival in carefully selected patients with acceptable toxicity and preserved quality of life: Haematologica, 2019; 104; 370-79
8. Dreger P, Allogeneic stem cell transplant in non-Hodgkin lymphomas: Still an indication?: Hematol Oncol, 2021; 39(Suppl 1); 100-3
9. Passweg JR, Baldomero H, Chabannon C, The EBMT activity survey on hematopoietic-cell transplantation and cellular therapy 2018: CAR-T’s come into focus: Bone Marrow Transplant, 2020; 55; 1604-13
10. Ruutu T, Gratwohl A, de Witte T, Prophylaxis and treatment of GVHD: EBMT-ELN working group recommendations for a standardized practice: Bone Marrow Transplant, 2014; 49; 168-73
11. Martin PJ, Rizzo JD, Wingard JR, First- and second-line systemic treatment of acute graft-versus-host disease: Recommendations of the American Society of Blood and Marrow Transplantation: Biol Blood Marrow Transplant, 2012; 18; 1150-63
12. The Japanese Data Center for Hematopoietic Cell Transplantation: Hematopoietic cell transplantation in Japan annual report of nationwide survey, 2020 http://www.jdchct.or.jp/en/data/slide/2020/
13. Ghimire S, Weber D, Mavin E, Pathophysiology of GvHD and other HSCT-related major vomplications: Front Immunol, 2017; 8; 79
14. Norona J, Apostolova P, Schmidt D, Glucagon-like peptide 2 for intestinal stem cell and Paneth cell repair during graft-versus-host disease in mice and humans: Blood, 2020; 136; 1442-55
15. Petersen PE: Community Dent Oral Epidemiol, 2003; 31(Suppl 1); 3-23
16. Drucker DJ, Yusta B, Physiology and pharmacology of the enteroendocrine hormone glucagon-like peptide-2: Annu Rev Physiol, 2014; 76; 561-83
17. Abdalqadir N, Adeli K, GLP-1 and GLP-2 orchestrate intestine integrity, gut microbiota, and mmune system crosstalk: Microorganisms, 2022; 10; 2061
18. Janssen P, Rotondo A, Mule F, Tack J, Review article: A comparison of glucagon-like peptides 1 and 2: Aliment Pharmacol Ther, 2013; 37; 18-36
19. Drucker DJ, Biological actions and therapeutic potential of the glucagon-like peptides: Gastroenterology, 2002; 122; 531-44
20. Tsai CH, Hill M, Asa SL, Brubaker PL, Drucker DJ, Intestinal growth-promoting properties of glucagon-like peptide-2 in mice: Am J Physiol, 1997; 273; E77-84
21. Litvak DA, Hellmich MR, Evers BM, Glucagon-like peptide 2 is a potent growth factor for small intestine and colon: J Gastrointest Surg, 1998; 2; 146-50
22. Amato A, Baldassano S, Mule F, GLP2: An underestimated signal for improving glycaemic control and insulin sensitivity: J Endocrinol, 2016; 229; R57-66
23. Markovic MA, Brubaker PL, The roles of glucagon-like peptide-2 and the intestinal epithelial insulin-like growth factor-1 receptor in regulating microvillus length: Sci Rep, 2019; 9; 13010
24. Kong S, Zhang YH, Zhang W, Regulation of intestinal epithelial cells properties and functions by amino acids: Biomed Res Int, 2018; 2018; 2819154
25. Zeiser R, Chen YB, Youssef NN, Ayuk F, Pathophysiology of gastrointestinal acute graft-versus-host disease and the potential role of glucagon-like peptide 2: Br J Haematol, 2023; 201; 620-27
26. Levine JE, Braun TM, Harris AC, A prognostic score for acute graft-versus-host disease based on biomarkers: A multicentre study: Lancet Haematol, 2015; 2; e21-29
27. Bow EJ, Infection risk and cancer chemotherapy: the impact of the chemotherapeutic regimen in patients with lymphoma and solid tissue malignancies: J Antimicrob Chemother, 1998; 41(Suppl D); 1-5
28. Taur Y, Jenq RR, Perales MA, The effects of intestinal tract bacterial diversity on mortality following allogeneic hematopoietic stem cell transplantation: Blood, 2014; 124; 1174-82
29. Clarke RT, Jenyon T, van Hamel Parsons V, King AJ, Neutropenic sepsis: Management and complications: Clin Med (Lond), 2013; 13; 185-87
30. Taur Y, Xavier JB, Lipuma L, Intestinal domination and the risk of bacteremia in patients undergoing allogeneic hematopoietic stem cell transplantation: Clin Infect Dis, 2012; 55; 905-14
31. Norona J, Apostolova P, Schmidt D, Glucagon-like peptide 2 for intestinal stem cell and Paneth cell repair during graft-versus-host disease in mice and humans: Blood, 2020; 136; 1442-55
32. Dimitriadou V, Chabot-Roy G, Audiger C, Apraglutide decreases severity of intestinal damage from gastrointestinal (GI) acute graft versus host disease (GvHD) following allogeneic transplantation (alloHSCT) without impacting engraftment: EBMT, 2022 Poster presentation P198
33. Hargrove DM, Alagarsamy S, Croston G, Pharmacological characterization of apraglutide, a novel long-acting peptidic glucagon-like peptide-2 agonist, for the reatment of short bowel syndrome: J Pharmacol Exp Ther, 2020; 373; 193-203
34. Herbers AH, Feuth T, Donnelly JP, Blijlevens NM, Citrulline-based assessment score: First choice for measuring and monitoring intestinal failure after high-dose chemotherapy: Ann Oncol, 2010; 21; 1706-11
35. Crenn P, Messing B, Cynober L, Citrulline as a biomarker of intestinal failure due to enterocyte mass reduction: Clin Nutr, 2008; 27; 328-39
36. Lutgens LC, Deutz NE, Gueulette J, Citrulline: A physiologic marker enabling quantitation and monitoring of epithelial radiation-induced small bowel damage: Int J Radiat Oncol Biol Phys, 2003; 57; 1067-74
37. Kim JW, Lee HJ, Yi HG, Mitoxantrone, etoposide, cytarabine, and melphalan (NEAM) followed by autologous stem cell transplantation for patients with chemosensitive aggressive non-Hodgkin lymphoma: Am J Hematol, 2012; 87; 479-83
38. Ali N, Adil SN, Shaikh MU, Autologous hematopoietic stem cell transplantation – 10 years of data from a developing country: Stem Cells Transl Med, 2015; 4; 873-77
39. Visani G, Malerba L, Stefani PM, BeEAM (bendamustine, etoposide, cytarabine, melphalan) before autologous stem cell transplantation is safe and effective for resistant/relapsed lymphoma patients: Blood, 2011; 118; 3419-25
40. Canadian Council on Animal Care: Guide to the Care and Use of Experimental Animals, 2018; 1
41. , Guide for the Care and Use of Laboratory Animals: The National Academies Collection: Reports funded by National Institutes of Health, 2011
42. Hill GR, Crawford JM, Cooke KR, Total body irradiation and acute graft-versus-host disease: The role of gastrointestinal damage and inflammatory cytokines: Blood, 1997; 90; 3204-13
43. Thompson JS, Chu Y, Glass JF, Brown SA, Absence of IL-23p19 in donor allogeneic cells reduces mortality from acute GVHD: Bone Marrow Transplant, 2010; 45; 712-22
44. Wang ZK, Yang YS, Chen Y, Intestinal microbiota pathogenesis and fecal microbiota transplantation for inflammatory bowel disease: World J Gastroenterol, 2014; 20; 14805-20
45. Szyska M, Na IK, Bone marrow GvHD after llogeneic hematopoietic stem cell transplantation: Front Immunol, 2016; 7; 118
46. Ran XZ, Shi CM, Zheng HE, Su YP, Cheng TM, Experimental research on the management of combined radiation-burn injury in China: Radiat Res, 2011; 175; 382-89
47. Boushey RP, Yusta B, Drucker DJ, Glucagon-like peptide (GLP)-2 reduces chemotherapy-associated mortality and enhances cell survival in cells expressing a transfected GLP-2 receptor: Cancer Res, 2001; 61; 687-93
48. Hytting-Andreasen R, Balk-Moller E, Hartmann B, Endogenous glucagon-like peptide-1 and 2 are essential for regeneration after acute intestinal injury in mice: PLoS One, 2018; 13; e0198046
49. Deniz MAB, Dane F, Can G, Radiation-induced oxidative injury of the ileum and colon is alleviated by glucagon-like peptide-1 and -2: JRRAS, 2015; 8; 234-42
50. Drucker DJ, Gut adaptation and the glucagon-like peptides: Gut, 2002; 50; 428-35
51. Secombe KR, Coller JK, Gibson RJ, The bidirectional interaction of the gut microbiome and the innate immune system: Implications for chemotherapy-induced gastrointestinal toxicity: Int J Cancer, 2019; 14; 2365-76
52. Peled JU, Hanash AM, Jenq RR, Role of the intestinal mucosa in acute gastrointestinal GVHD: Blood, 2016; 128; 2395-402
53. Goker H, Haznedaroglu IC, Chao NJ, Acute graft-vs-host disease: Pathobiology and management: Exp Hematol, 2001; 29; 259-77
54. Hill GR, Ferrara JL, The primacy of the gastrointestinal tract as a target organ of acute graft-versus-host disease: Rationale for the use of cytokine shields in allogeneic bone marrow transplantation: Blood, 2000; 95; 2754-59
Figures
Figure 1. Effect of cytarabine or melphalan±apraglutide on survival. Effect of cytarabine with or without apraglutide (3.3 mg/kg) on survival (group with daily dosing of apraglutide from day −4 not shown) (A); effect of cytarabine without apraglutide or with different doses of apraglutide on survival (B); and effect of melphalan with or without apraglutide 3.3 mg/kg on survival (high dose group 17.5 mg/kg apraglutide not shown) (C). (A) Kaplan-Meier curves. Animal survival was monitored daily. n=6–18 at time=0 for each treatment group. Apraglutide treatment initiated either before or concomitantly with the chemotherapy, showed significant difference relative to animals treated with cytarabine alone, as determined by log-rank (Mantel-Cox) test. When comparing to the vehicle/control group, survival of animals treated with cytarabine only was significantly different, as determined by log-rank (Mantel-Cox) test. No statistical difference was observed between the vehicle/control group and the groups that were treated with apraglutide. * P<0.0001. (B) Kaplan-Meier curves. GLP-2 receptor agonists (apraglutide, hGLP-2) were administered 4 days before and 5 days during cytarabine chemotherapy treatment. Animal survival was monitored daily. n=16 at time=0 for each treatment group; significant difference relative to vehicle/cytarabine-treated animals as determined by log-rank (Mantel-Cox) test. * P<0.05, # P<0.01. (C) Kaplan-Meier curves. Animal survival was monitored daily. n=10 at time=0 for each treatment group. When comparing to the vehicle/control group, survival of animals treated only with melphalan was significantly different as determined by log-rank (Mantel-Cox) test. No statistical difference was observed between the vehicle/control group or the melphalan-only group and the group treated with apraglutide 3.3 mg/kg. * P≤0.001. BID – twice daily; QD – once daily.Figure 2. Effect of cytarabine or melphalan±apraglutide treatment on body weight change. Effect of cytarabine with or without apraglutide on body weight change at day 7 (A); effect of cytarabine with or without apraglutide on body weight change (B); and effect of melphalan with or without apraglutide on body weight change (C). (A) Data are presented as mean±SEM values (n=12–16 per group). * Significant difference relative to cytarabine/vehicle-treated animals as determined by one-way ANOVA and Newman-Keuls multiple comparison post hoc analysis. (B) Animal body weight was monitored daily. n=6–18 at time=0 for each treatment group. Data are shown as mean±SEM values. The body weight change of animals treated with cytarabine alone or in combination with apraglutide was significantly lower as compared with control/vehicle animals (statistics not shown). (C) Animal body weight was monitored daily. n=10 at time=0 for each treatment group. Data are shown as mean±SEM values. Data were analyzed using the unpaired t-test per row (plus Holm-Sidak method for multiple comparisons correction); indicates days of treatment with apraglutide. * P≤0.001 vs control. NS – non-significant; LYMPH – lymphocytes; NEUT – neutrophils; recov – recovery; WBC – white blood cells.Figure 3. Effect of apraglutide on leukopenia in BALB/c mice. Effect on polymorphonuclear cell count following chemotherapy (A) and effect on the myelosuppressive activity of cytarabine (B). (A) Treatment group mean±SEM are shown (n=6 per treatment group); cell counts were determined in specifically designated animals. (B) Immunosuppressive activity was monitored at the end of the study. Samples were collected at euthanasia (n=3). Data are shown as mean±SEM values. As determined by the unpaired t-test according to the Holm-Sidak method for multiple comparisons, the mean number of WBC, NEUT, and LYMPH was significantly decreased in animals treated with cytarabine alone or in combination with apraglutide, compared with the control (* P<0.05, # P<0.01) and recovery groups (& P<0.05, $ P<0.01). No difference was observed between animals treated with cytarabine alone or in combination with apraglutide. No difference was observed either between the control mice and those in the recovery group treated with cytarabine plus apraglutide (NS).Figure 4. Apraglutide protects gastrointestinal epithelium structure from chemotherapy-induced injury. Representative micrographs of small intestine from animals treated with cytarabine (A) or melphalan (B), with and without apraglutide.Figure 5. Dose-dependent effect of apraglutide on serum citrulline concentration following treatment with cytarabine. Data are shown as treatment group mean±SEM values. n=3 per treatment group; citrulline levels were only determined in specifically designated animals. * Significant difference relative to vehicle-only control animals. # Significant difference relative to the cytarabine/vehicle-treated animals, as determined by one-way ANOVA and Newman-Keuls multiple comparison post hoc analysis. BID – twice daily; SEM – standard error of mean.Figure 6. Effect of apraglutide on the diversity of the intestinal microbiota after chemotherapy (relative mean abundance of taxa in feces at the phylum level). SD – standard deviation; SEM – standard error of mean.Figure 7. Effect of apraglutide on survival in TBI/BMT-treated mice (TBI 7 Gy). Kaplan-Meier curves. Animal survival was monitored daily. n=10 at time=0 for the irradiated groups and n=5 for the control group. Survival of animals treated with apraglutide initiated before TBI/BMT showed significant difference relative to TBI/BMT animals, as determined by log-rank (Mantel-Cox) test, but the difference was not significant compared with control animals. When comparing to the control group, survival of TBI/BMT was significantly different. TBI/BMT – total body irradiation/bone marrow transplantation.Figure 8. Apraglutide improves gastrointestinal pathological score following induction of aGvHD (TBI 7 Gy). Group A: TBI/transplanted mice treated with apraglutide; Group B: TBI/transplanted mice treated with vehicle; Group C: control mice treated with vehicle only and no transplantation. GvHD – graft-versus-host disease; TBI – total body radiation.Figure 9. Morphological changes induced by total body irradiation followed by allogenic bone marrow transplantation and protective effect of apraglutide (TBI 8.5 Gy).Figure 10. Effect of apraglutide on morphological damage of the jejunum and histological score induced by TBI (8.5 Gy) followed by allogeneic transplantation. Group A: TBI/transplanted mice treated with apraglutide; Group B: TBI/transplanted mice treated with vehicle. TBI at 8.5 Gy was applied. TBI – total body irradiation.Figure 11. Effect of apraglutide on colon length following TBI and allogeneic transplantation. Data are shown as mean±SEM values for length of intestinal colon. n=5–10 per group. Each dot represents data for one mouse. Data show that the length of the colon of TBI/BMT animals was significantly shorter as compared with the vehicle group or the TBI/BMT group treated with apraglutide (Brown-Forsythe and Welch ANOVA tests). No difference was observed between the vehicle group and the TBI/BMT animals treated with apraglutide. TBI at 7.0 Gy was applied. * P<0.01. ANOVA – analysis of variance; SEM4– standard error of mean; TBI – total body irradiation. In Press
Original article
The Anatomical Landscape of Living Donor Livers: A 101-Case Retrospective Single-Center Study in Indonesia ...Ann Transplant In Press; DOI: 10.12659/AOT.952031
Original article
Decreased Ventilation Duration and ICU Stay Associated With Early Percutaneous Dilatational Tracheostomy Af...Ann Transplant In Press; DOI: 10.12659/AOT.953143
Original article
Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients With Posttransplant Lymphoproliferati...Ann Transplant In Press; DOI: 10.12659/AOT.952021
Original article
Common Versus External Iliac Arterial Anastomosis in Kidney Transplantation: A Bicentric Retrospective Anal...Ann Transplant In Press; DOI: 10.12659/AOT.953269
Most Viewed Current Articles
24 Aug 2021 : Review article 20,864
Normothermic Machine Perfusion (NMP) of the Liver – Current Status and Future PerspectivesDOI :10.12659/AOT.931664
Ann Transplant 2021; 26:e931664
29 Dec 2021 : Original article 17,029
Efficacy and Safety of Tacrolimus-Based Maintenance Regimens in De Novo Kidney Transplant Recipients: A Sys...DOI :10.12659/AOT.933588
Ann Transplant 2021; 26:e933588
05 Apr 2022 : Original article 16,094
Impact of Statins on Hepatocellular Carcinoma Recurrence After Living-Donor Liver TransplantationDOI :10.12659/AOT.935604
Ann Transplant 2022; 27:e935604
22 Nov 2022 : Original article 16,067
Long-Term Effects of Everolimus-Facilitated Tacrolimus Reduction in Living-Donor Liver Transplant Recipient...DOI :10.12659/AOT.937988
Ann Transplant 2022; 27:e937988